Article Text

Abstract
Background To test whether working body schema of the trunk is disrupted in people with back pain using a motor imagery task in which one decides whether a pictured model has their trunk rotated to the left or to the right. The authors hypothesised that chronic back pain is associated with reduced accuracy of left/right trunk rotation judgements.
Methods 21 Patients with back pain and 14 controls completed two tasks, each involving two trials of 40 images: a left/right hand judgement task, which was used as a control task, and the left/right trunk rotation judgement task. Two (task) × three (group: bilateral back pain, unilateral back pain and control) analyses of variance were undertaken on mean response time and accuracy.
Results Response time was similar across participants and tasks (NS). Accuracy was not. The patients with bilateral back pain made more mistakes on the left/right trunk rotation task than patients with unilateral back pain, who in turn made more mistakes on that task than the controls (body part × group interaction; p<0.001). The mean (95% CI) accuracy for left/right trunk rotation judgements was 53.4% (44.5% to 62.3%) for the patients with bilateral back pain, 67.2% (60.2% to 74.1%) for the patients with unilateral back pain and 87% (75% to 98%) for the control participants. This pattern was not observed on the left/right-hand judgement task, on which all three groups made correct judgements about 83% of the time (NS).
Discussion Chronic back pain is associated with disruption of the working body schema of the trunk. This might be an important contributor to motor control abnormalities seen in this population.
Statistics from Altmetric.com
People with chronic painful conditions often find movement difficult, painful or both. Potential explanations that have been proposed for these movement difficulties are that movement stimulates nociceptors in the painful body part, proprioceptive information is disrupted by tissue damage or during transmission to the brain1 and motor strategies2 3 or behavioural selections4 are shifted, perhaps by pain-related beliefs5 or fear of (re)injury.6 Another potential explanation but one that has not been empirically interrogated is that the brain is unable to integrate cortical proprioceptive representation or working body schema with motor processes.
There is a growing body of literature that shows chronic pain to be associated with disruption of cortically held body schema. For example, somatosensory-evoked potentials are shifted in people with complex regional pain syndrome (CRPS),7,–,9 phantom limb pain10 11 and back pain.12 Distorted body image or perceived size, shape and orientation of the painful body part has also been reported in these groups.13,–,15 16
Mapping the surfaces of the body in primary sensory cortex is relatively straightforward because one can stimulate a particular location on the body surface and record the electrical response. Mapping the working body schema is less straightforward, in part because several body maps seem to contribute (eg, body surface maps, visual field maps, vestibular-derived maps and primary motor maps)17 and a clear neural correlate of working body schema has not been identified.
A pragmatic way to investigate the integrity of the working body schema is via motor imagery.18,–,20 For example, when we recognise a pictured limb as belonging to the left or the right side of the body, we make an initial judgement and then confirm or correct that judgement by mentally rotating our own limb to match the posture of that shown in the picture.21 That is, left/right judgements of pictured limbs requires an intact working body schema.22 When one first performs left/right judgements, the motor imagery is explicit: one is aware that one is mentally rotating one's own limb to match that in the picture. In fact, it is often difficult to keep one's limbs still during the task. After practice (about 80 pictures), the motor imagery becomes implicit: one is no longer aware of mentally rotating one's own limb. Imaging studies corroborate this observation: in addition to posterior parietal and sensory cortices, left/right limb judgements initially activate premotor, supplementary motor and primary motor cortices. After practice, only premotor and supplementary motor cortices are activated by the task.23 Frank disruption of the body schema is associated with disruption of left/right limb judgements—for example, in people with CRPS,20 24 amputees25 26 and those with spatial neglect after stroke.18
We modified the left/right limb judgement task to interrogate the working body schema of the trunk; the participants make judgements about whether a pictured model has their trunk turned to the left or right. Increased error rate is likely to reflect disruption of the working body schema. In contrast, increased reaction time on such a task is likely to reflect a disruption of information processing that manifests as a bias towards one choice over the other; the mental movement to match the posture reveals the choice to be wrong, which delays the final response.27 Thus, there is an increase in reaction time, but responses are accurate. We used this left/right trunk rotation task to investigate whether the working body schema of the trunk is disrupted in people with back pain. We hypothesised that people with back pain would make more errors on this task than people without back pain.
Methods
Informed consent was obtained from all the participants. All the procedures were approved by institutional ethics committees and conformed to the Helsinki Declaration. First, we interrogated the repeatability of this new task in patients and controls. Second, we undertook a cross-section study of patients with back pain and healthy controls.
Repeatability of left/right trunk rotation judgement task in the patients and the controls
A convenience sample of five patients with back pain were recruited (one was male, and three were right-handed; mean (SD): age 46(16) years; duration of symptoms of this episode 305 (561) weeks; duration since the first episode 559 (620) weeks; 100 mm visual analogue scale (VAS) in response to the question “What was your average pain over the last 2 days?” 46(23) mm). A convenience sample of five control participants without back pain (two were male; 40(4) years) were also recruited.
Control task: left/right judgements of pictured hands
The participants undertook the left/right hand judgement task using the established protocol.24 Fifteen photographs of a right hand in various postures were copied and digitally mirrored to produce photographs of a left hand in identical postures. Photographs were displayed in random order on a screen using commercially available software (Recognise; Neuro Orthopaedic Institute, Adelaide, Australia; http://www.noigroup.com). The participants respond by pressing one button if the photograph shows a left hand and a different button if it shows a right hand. Emphasis is placed on the speed and accuracy of the responses. That is, they are instructed to make accurate responses as quickly as possible. Forty pictures constituted a trial. Two trials constituted the task. The number of correct responses was expressed as a percentage of the total number of pictures displayed and was called accuracy. The mean response time for correct responses (RT) was called response time. Thus, RT and accuracy were the primary outcome variables.
Left/right trunk rotation judgements
Twenty-eight photographs of a male model were taken in a variety of positions. In each position, the trunk was rotated to the right between 5° and 90°. The photographs were digitally mirrored to construct otherwise identical pictures of the same model in various degrees of left rotation of the trunk. This produced a picture bank of 56 photographs, which was integrated into the Recognise programme. The photographs were then displayed in random order using Recognise. The participants responded by pressing one button if the photograph showed the model in left trunk rotation and a different button if it showed the model in right trunk rotation. Emphasis was again placed on the speed and the accuracy of the responses. Two trials of 40 images constituted the task. RT and accuracy were again the primary outcome variables.
Protocol
The participants sat in front of a monitor and keyboard with both forearms resting on the table. They positioned themselves so that they were comfortable. The index and middle finger of the dominant hand were placed on the appropriate response keys: “a” for left and “d” for right. The participants then performed the left/right-hand judgement task and the left/right trunk rotation task. The five patients and the five control participants completed the left/right judgements of pictured hands and left/right trunk rotation judgement tasks in five separate sessions, separated by at least 1 day (mean (range) 4(1 to 7)). The order of the tasks was randomised and counterbalanced across the sessions. Each trial was preceded by a practice trial of 80 pictures.
Statistical analyses
All statistics were undertaken using SPSS V.11.0.0 (SPSS, Chicago, Illinois, USA). Four separate two-way random effects intraclass correlation coefficients (ICCs) were calculated: RT and accuracy for the patients and the controls.
Experiment: is back pain associated with increased error rate of left/right trunk rotation judgements?
A separate convenience sample of 21 patients with back pain (six were male, and 17 were right-handed; mean(SD): age 44(13) years; duration of symptoms of this episode 122(296) weeks; duration since the first episode 374(446) weeks; VAS of the present pain intensity, 0–100 mm from the left anchor, “no pain” 37(21) mm) were recruited from a private physiotherapy practice (table 1). The participants were excluded if they had systemic disease, visual or motor impairment including dyslexia, arm or leg pain or abnormality or if they were pregnant.
ICCs for the left/right trunk rotation task and the left/right hand judgement task in the patients with back pain and the healthy controls
Fourteen asymptomatic participants (five were male, and all were right-handed; 43(7) years) were recruited as healthy controls. Control participants were excluded if they had back pain or an episode of back pain sufficient to limit activities of daily living within the past year; if they had systemic disease, visual or motor impairment including dyslexia, arm or leg pain or abnormality or if they were pregnant. The controls were not specifically matched to the patients, but the age, sex mix, body mass index and activity level of the groups were evaluated.
Assessments
The patients completed the Short-Form McGill Pain Questionnaire28 and the habitual physical activity questionnaire,29 both of which have established reliability and validity for back pain. The control participants completed only the habitual physical activity questionnaire.
Protocol
Demographic and clinical data were collected in an interview and a standard full physical examination was undertaken by a senior musculoskeletal physiotherapist (HB). These assessments determined the location and the characteristics of the participants' back pain. The participants then completed the questionnaires. The participants then undertook the two left/right judgement tasks. The order of tasks was randomised and counterbalanced between the participants. Each trial was preceded by a practice trial of 80 pictures, and the participants sat quietly for 3 min between trials.
Statistical analysis
To test the hypothesis that left/right trunk rotation judgements are disrupted in patients with back pain, we undertook two repeated measures analyses of variance, one on RT for correct judgements and one on accuracy. For each analysis of variance, the within-participant factor was body part (two levels: hand or trunk) and the between-participant factor was group (three levels: patients with unilateral back pain, patients with bilateral back pain and controls). We hypothesised that patients with unilateral back pain would perform worse than controls, and on the basis of the notion that a wider area of pain would be associated with a wider disruption of the working body schema, we hypothesised that those with bilateral back pain would perform worse than those with unilateral back pain.
In the secondary analyses, linear regression was used to investigate the relationship between (1) duration of symptoms and (2) present pain intensity, as measured on the McGill Pain Questionnaire, and each of the primary outcome variables, RT and accuracy.
Results
Repeatability of left/right trunk rotation judgement task
The variance and the repeatability of both the RT and accuracy measures obtained from the left/right trunk rotation judgement task were acceptable for the patients and the controls and comparable with that of the established left/right hand judgement task. Table 1 shows the ICCs for both measures and both tasks.
Experiment: is back pain associated with disrupted left/right judgements of trunk rotation?
Complete data sets were obtained from all the participants. The patient characteristics including pain intensity, duration and location are shown in table 2. The age, the sex mix, the body mass index and the activity level of the groups were similar (p>0.27 for all).
Patient characteristics
Reaction time for correct responses
RT was affected neither by group nor by task. That is, patients with back pain were neither slower nor quicker at either task than the healthy controls (no main between-participants effect of group: F(2,36)=1.539, p=0.228; no main within-participants effect of body part: F(1,36)=0.342, p=0.562). There was no body part × group interaction (F(2,36)=2.209, p=0.146). The mean (95% confidence interval (CI)) RT for left/right trunk rotation judgements) was 2.4 seconds (2.2 to 2.6 seconds) for patients with back pain and 2.4 seconds (2.2 to 2.5 seconds) for the healthy controls.
Accuracy of left/right trunk rotation judgements
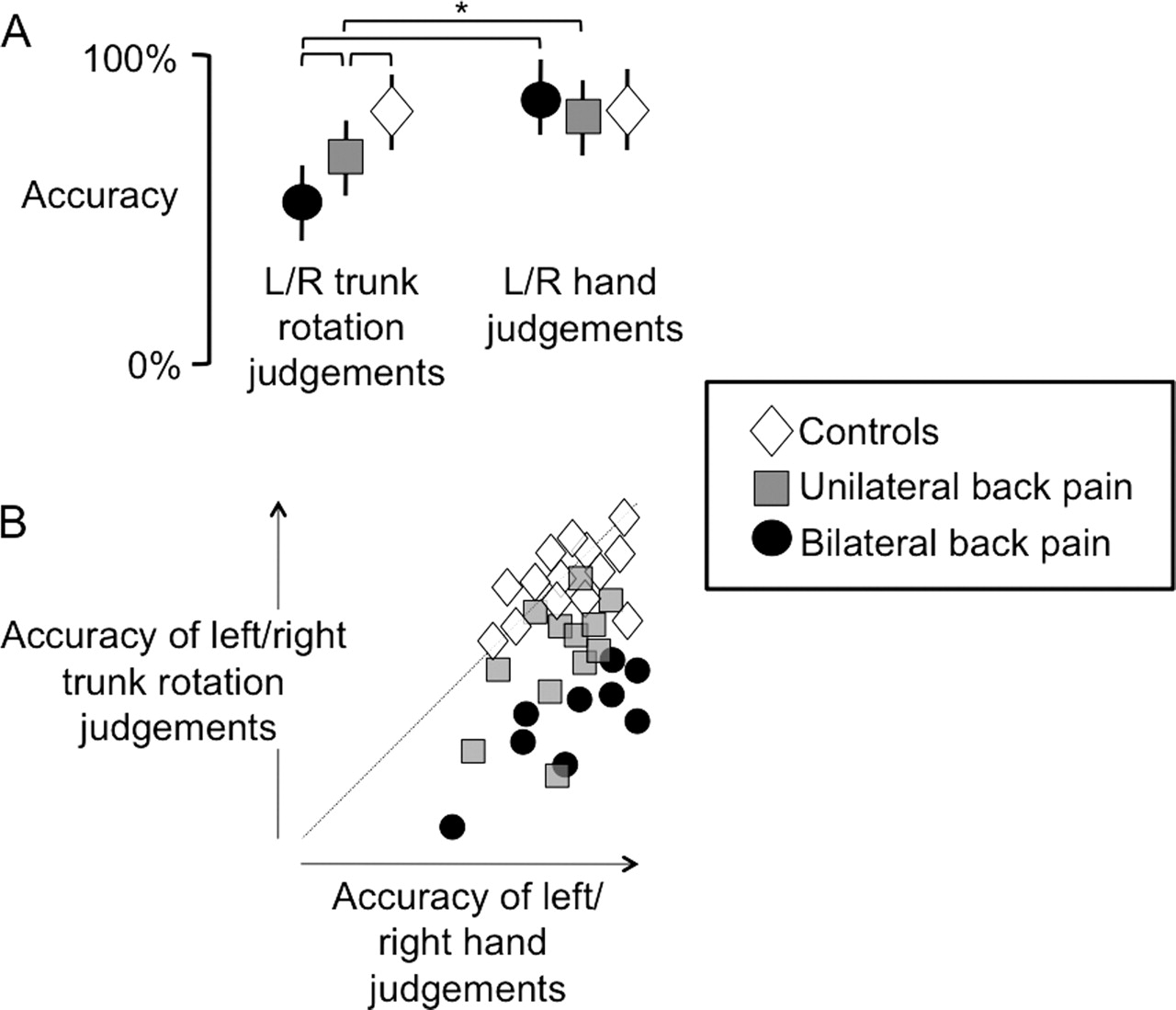
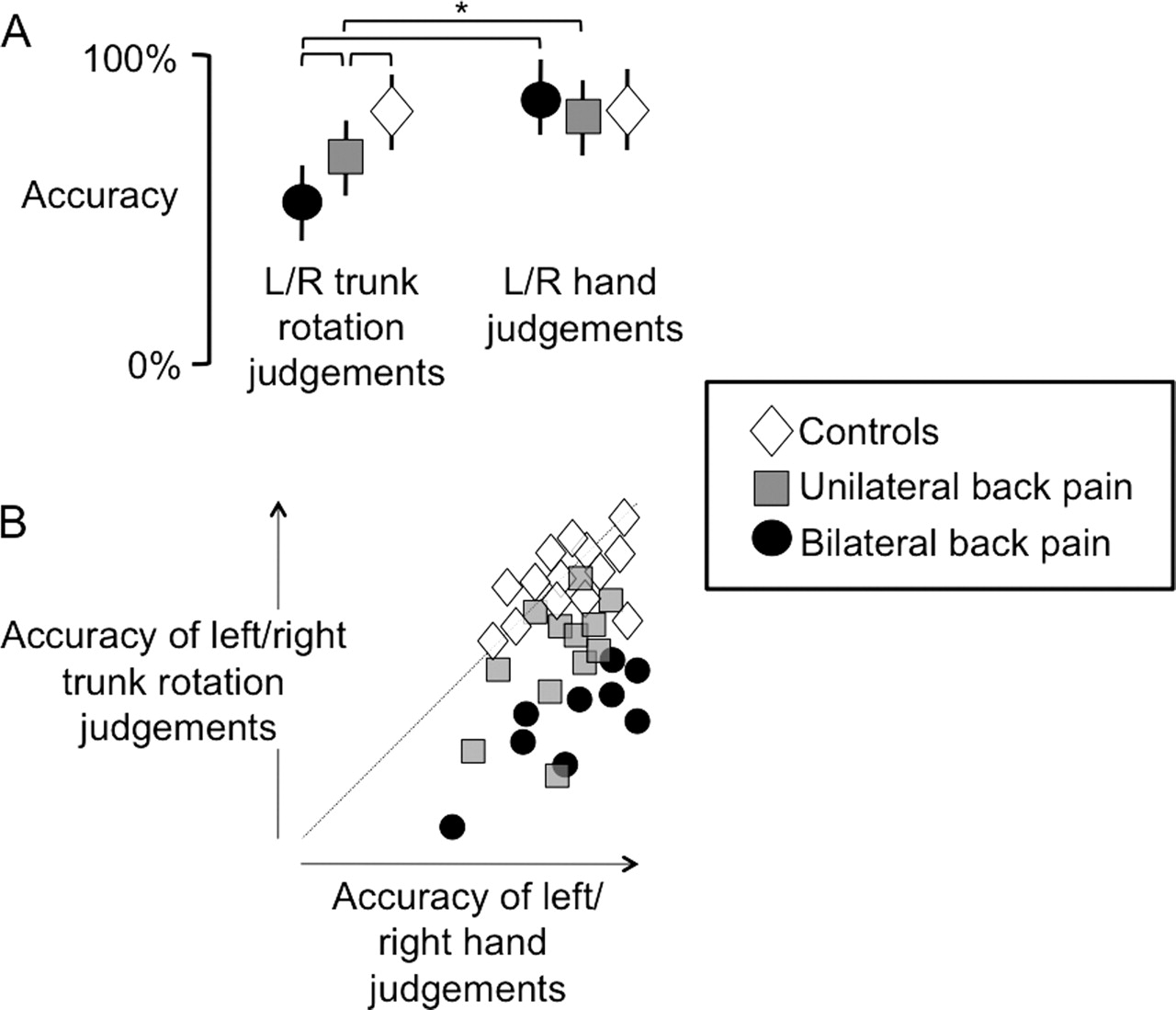
Accuracy was affected by the group and by the task (figure 1). That is, patients with bilateral back pain made more errors overall than the controls (main between-participants effect of group: F(2,36)=4.720, p<0.015; Scheffe post hoc test: mean difference 11.89%, p=0.022), but there was no difference overall between the patients with bilateral back pain and those with unilateral back pain (p=0.987). The participants made more mistakes on the trunk rotation judgement task than on the hand judgement task, regardless of group (main within-participants effect of body part: F(2,36)=69.26, p<0.001).
{kind=link}
A, Mean (shapes) and SD (error bars) accuracy for the controls (diamonds), the patients with unilateral back pain (squares) and the patients with bilateral back pain (circles) at making left/right trunk rotation judgements and left/right hand judgements. The asterisk denotes significance at p<0.05. B, Individual participant data showing accuracy at left/right hand judgement (x-axis) versus left/right trunk rotation judgement. Shapes to the right of the diagonal line indicate less accuracy for trunk rotation judgements than for hand judgements. Note that the fi lled circles (bilateral back pain) are furthest from the diagonal line and the diamonds (controls) are clustered around the diagonal line.
The above main effects were driven by a strong body part × group interaction (F(2,36)=18.217, p<0.001), which revealed that the patients with bilateral back pain made more mistakes on the left/right trunk rotation task than the patients with unilateral back pain, who in turn made more mistakes on that task than the controls. The mean (95% CI) accuracy for left/right trunk rotation judgements was 53.4% (44.5% to 62.3%) for patients with bilateral back pain, 67.2% (60.2% to 74.1%) for patients with unilateral back pain and 87% (75% to 98%) for the control participants. This pattern was not observed on the left/right hand judgement task, on which all three groups made correct judgements about 83% of the time (fig 1).
Are left/right trunk rotation judgements related to pain intensity or duration of symptoms?
Neither the mean RT for the correct responses nor the accuracy for the left/right trunk rotation judgement task was related to current pain intensity or to the duration of symptoms (F change (2,18)=0.798 and p=0.466 for RT; F change (2,18)=0.093 and p=0.912 for accuracy).
Discussion
We hypothesised that patients with back pain would make more errors on a left/right trunk rotation judgement task but not a left/right hand judgement task than healthy controls. The results support that hypothesis because the patients with bilateral back pain made more mistakes on that task than those with unilateral back pain who made more mistakes than the healthy controls. In fact, the patients with bilateral back pain were no better than chance at judging whether a pictured model had their trunk turned to the left or to the right. Importantly, the patients with back pain performed similarly to the healthy controls on the left/right hand judgement task, which rules out disruption of mechanisms common to both—for example, reduced central nervous system processing resources. The current data are consistent with those of a previous work: the left/right hand judgement task data for both the patients and the controls were similar to the data from healthy controls in previous studies.20 24 27 30 31
That patients with back pain perform badly at a trunk-related implicit motor imagery task but not at an arm-related motor imagery task is a new finding, although it is not altogether surprising. The patients with arm pain perform badly on an arm-related motor imagery task but not on a leg-related one.24 The novel aspect of the current results is the nature of the disruption: decreased accuracy and normal RT. Although this is the first study to interrogate implicit motor imagery of the trunk, there are a large number of studies on limb laterality recognition that suggest a likely interpretation of this result. Three processes contribute to left/right limb judgements: an initial automatic selection, integration of the body schema with motor processes and response.22 Disruption of the initial automatic selection would probably increase RT rather than decrease accuracy because confirmation via motor imagery would lead to correction of the initial response. The response would be delayed but correct. A left/right difference in RT probably reflects an information processing bias toward one side over the other.27 Pain and the expectation of pain in one hand both cause an increase in RT for correct judgement of the non-painful hand, which can be interpreted as reflecting a bias in information processing toward the painful side.27 32 This investigation using left/right trunk rotation judgements RTs would seem unlikely to detect such a bias because we had too few patients with unilateral back pain to make the comparison. Furthermore, back pain is seldom as spatially discreet as limb pain; back pain often spreads or moves across the midline and limb pain does not.
Disruption of the final response phase of the task is also unlikely to explain the increased error rate in back pain because the response phase would be similarly disrupted in both the trunk rotation judgement task and the hand judgement task. This leaves the middle process, the integration of the working body schema with motor processes.
There is mounting evidence that the body schema is disrupted in people with back pain. For example, back pain is associated with reorganisation of the primary somatosensory cortex (S1); the area of activation in response to electrical stimuli applied to the back is substantially increased and is shifted 2–3 cm medially.12 Consistent with that, a two-point discrimination threshold that is dependent though not solely upon S1 neurons is increased in the area of usual pain in patients with back pain.15 33 Importantly, this increase in two-point discrimination threshold is positively related to a loss of voluntary lumbopelvic control.33 The representation in primary motor cortex of the deepest abdominal muscle, an important muscular controller of the lumbar spine,34 is shifted in patients with back pain.35 Finally, perceptual characteristics are also distorted: when asked to draw the perceived outline of their back, patients with back pain report that they “can't find it” in the area of their usual pain.15
It has been suggested that disrupted cortical representations are actually a cause of ongoing pathological pain.36 In phantom limb pain and CRPS, the extent of S1 reorganisation correlates with pain37 and recovery is associated with normalisation of S1 organisation,38,–,40 which lend support to this theory. However, there are also problems with this theory: S1 holds maps of the surfaces of the body, and these maps can be altered without causing pain or disturbing movement.41 It is likely that the mechanisms that underpin the change in somatosensory-evoked responses induced by altering sensory input41 and those associated with chronic pathological pain37 are different.42 However, if disrupted working body schema of the trunk contributes to back pain, we would have expected to see a relationship between disruption of left/right trunk rotation judgement and present pain intensity, which we did not. Regardless of whether or not disrupted working body schema contributes directly to pain, it has clear functional implications. For example, disrupted working body schema is likely to introduce error in motor commands, which will affect movement outcome and may predispose to injury. Finally, although the current work does not demonstrate a causative link between back pain and disrupted working body schema, it raises the possibility that one exists, which in turn raises the possibility that therapeutic strategies that normalise working body schema may be helpful in rehabilitation. Such a possibility seems worthy of further investigation.
Interpretation of the current results should consider several limitations to this study. First, we recorded neither muscle activity nor autonomic response, so we cannot completely exclude peripheral mechanisms or autonomic input as confounders, although they seem unlikely. Experimentally manipulating muscle activity does not decrease accuracy on a left/right judgement task.30 Second, we used a convenience sample of patients and healthy controls, which were not matched in a participant-by-participant fashion, although the average age and proportion of males to females was similar.
In summary, the patients with bilateral back pain made more errors than those with unilateral back pain, who in turn made more errors than the healthy controls, on a left/right trunk rotation task, but they all performed similarly on a left/right hand judgement task. The reduced accuracy is probably mediated by disruption of the working body schema and integration of with motor processes, which raises implications for our understanding and management of this patient group.
References
Footnotes
Both authors contributed equally to this study.
-
Funding The Nuffield Oxford Medical Fellowship granted support to GLM. The National Health & Medical Research Council of Australia granted support to GLM.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Royal Free and University College Medical School, University College London, London, UK.
-
Provenance and peer review Not commissioned; externally peer reviewed.