Article Text

Abstract
Objective Knee abduction moment (KAM) during landing predicts non-contact anterior cruciate ligament (ACL) injury risk with high sensitivity and specificity in female athletes. The purpose of this study was to employ sensitive laboratory (lab-based) tools to determine predictive mechanisms that underlie increased KAM during landing.
Methods Female basketball and soccer players (N=744) from a single county public school district were recruited to participate in testing of anthropometrics, maturation, laxity/flexibility, strength and landing biomechanics. Linear regression was used to model KAM, and logistic regression was used to examine high (>25.25 Nm of KAM) versus low KAM as surrogate for ACL injury risk.
Results The most parsimonious model included independent predictors (β±1 SE) (1) peak knee abduction angle (1.78±0.05; p<0.001), (2) peak knee extensor moment (0.17±0.01; p<0.001), (3) knee flexion range of motion (0.15±0.03; p<0.01), (4) body mass index (BMI) Z-score (−1.67±0.36; p<0.001) and (5) tibia length (−0.50±0.14; p<0.001) and accounted for 78% of the variance in KAM during landing. The logistic regression model that employed these same variables predicted high KAM status with 85% sensitivity and 93% specificity and a C-statistic of 0.96.
Conclusions Increased knee abduction angle, quadriceps recruitment, tibia length and BMI with decreased knee flexion account for 80% of the measured variance in KAM during a drop vertical jump.
Clinical relevance Females who demonstrate increased KAM are more responsive and more likely to benefit from neuromuscular training. These findings should significantly enhance the identification of those at increased risk and facilitate neuromuscular training targeted to this important risk factor (high KAM) for ACL injury.
Statistics from Altmetric.com
Introduction
Female athletes are currently reported to be four to six times more likely than males to sustain a sports-related non-contact anterior cruciate ligament (ACL) injury.1 2 Altered neuromuscular strategies or decreased neuromuscular control during the execution of sports movements, as evidenced by abnormal lower limb joint mechanics (motions and loads), may underlie the increased risk of ACL injury in female athletes.3,–,8 Prospective measures of external knee abduction moment (KAM) during landing predict non-contact ACL injury risk in young female athletes (figure 1).5 In addition, a large-scale prospective study found that military cadets who sustained ACL injury demonstrated increased valgus alignment during the landing phase of a drop vertical jump (DVJ).9 Female athletes exhibit a related increase in lower extremity valgus alignment (figure 2) and KAM (figure 3) compared with males during landing and pivoting movements.3 7 10,–,17 Similar lower extremity valgus alignments are often demonstrated by females during injury.18,–,21 While these investigations provide an important understanding of a risk factor related to injury, it is relevant to define the inciting mechanisms that underlie the high injury risk mechanics, in order to provide increased potential to target modifiable contributors to injury with neuromuscular training.22

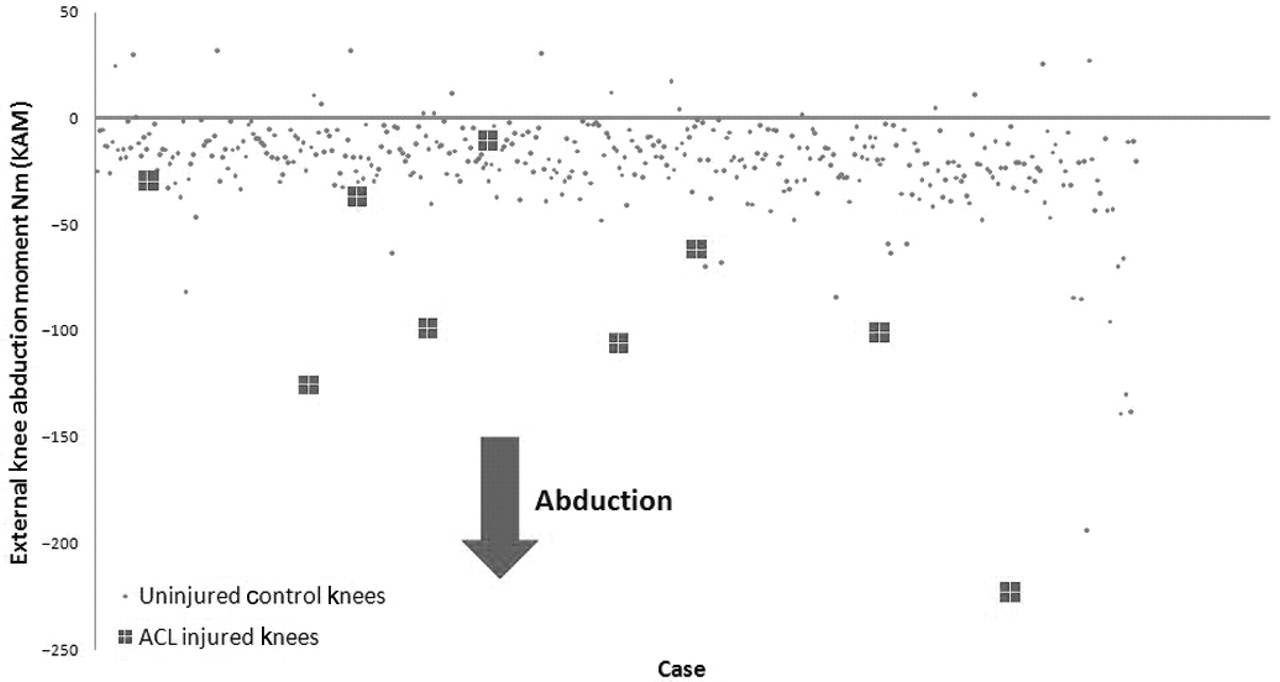
Scatter plot of data (N=399) utilised to define the cut-point used to classify the dependent variable high or low knee abduction moment status. Data were treated with logistic regression analyses to determine the value that would provide the maximal sensitivity and specificity for prediction of anterior cruciate ligament (ACL) injury risk during a drop vertical jump.

Videographic depiction of athlete with kinematic pattern that is likely to demonstrate a high knee abduction moment.

Motion analysis depiction of athlete with kinematic and kinetic pattern indicative of a high knee abduction moment.
The mechanics of growth and development may underlie dangerous biomechanics that lead to increased risk of ACL injury among female athletes.12 23 While strong evidence exists to show that there is a sex difference in ACL injury rates in postpubertal athletes, there is no evidence that this trend is observed in prepubescent athletes.24,–,27 However, knee injuries do occur in preadolescent athletes; up to two-thirds of these sports-related injuries in children are reported as joint sprains, with the majority of sprains presenting at the knee.27 Specific sprains such as injuries to the ACL are rarer and do not represent sex differences in children prior to their growth spurt.24,–,26 However, following the growth spurt, female athletes have higher rates of knee sprains, and this trend continues into maturity.28 In addition to increased injury prevalence, which peaks at age 16, female athletes also demonstrate incremental increases in KAM as they increase in chronological age. Interestingly, the knee abduction loads that are related to increased knee injury risk also peak concurrently at age 16 in female athletes.29–30 These data demonstrate a relationship between maturational development and the tendency for high-risk female athletes to demonstrate a preferential, increased frontal plane load strategy, as opposed to a sagittal plane load absorption strategy, during dynamic sports-related activities. Preferential loading in the frontal plane and increased KAM during competitive play alter desirable sagittal plane mechanics, destabilise the knee, load the ACL and increase knee injury risk in female athletes.3,–,6 10 14 22 31,–,33
The purpose of the current study was to employ the sensitive laboratory driven (lab-based) tool to determine predictive mechanisms that underlie increased dynamic KAM during dynamic tasks. The central hypothesis that drove the statistical model development was: following the onset of puberty, rapid increases in bone length and body mass, in the absence of matched increases in strength and recruitment of the posterior musculature of the lower extremity kinetic chain, underlie the tendency for increased KAM during landing tasks in female athletes. Specifically, we hypothesised that measures related to bone length and body mass, in the absence of relative strength and recruitment of the posterior musculature and sagittal plane control of the lower extremity kinetic chain, would yield robust prediction of KAM.
Methods
Subjects
Between the years 2004 and 2008, all sixth- through 12th-grade female basketball and soccer players were recruited from a county public school district with five middle schools and three high schools to participate in a prospective longitudinal study. The goal of the study was to determine potential underlying mechanisms that increase ACL injury risk. The recruited schools yielded six high school and 15 middle school basketball teams, and seven high school and three middle school soccer teams. From the identified teams, 744 unique subjects' first time visits were designated for inclusion into the current analyses. Subjects were excluded (n=46) from the study if they did not complete biomechanical testing or if errors were found in the calculation of the dependent variable, KAM, leaving 698 subjects to be included in the analyses (mean±1 SD) (age 13.9±2.4 years; height 159.3±8.6 cm; body mass 54.0±12.5 kg; percentage of each maturational status 17.2% prepubertal, 29.9% pubertal and 52.8% postpubertal). For the initial model development, 598 of the 698 eligible subjects were randomly assigned to formulate the optimised prediction models. The data from the remaining randomly assigned (N=100) subjects were used for verification of the optimised multivariable linear and logistic prediction models.
Procedures
Cincinnati Children's Hospital Medical Center and Rocky Mountain University of Health Professions Institutional Review Boards approved the data collection procedures and consent forms. Parental consent and athlete assent were received prior to data collection. Subjects were tested prior to the start of their basketball or soccer competitive season. The testing consisted of a knee exam, medical history, maturational estimates, dynamic strength and landing biomechanical analysis.
Anthropometrics and maturational assessment
Height was measured with a stadiometer with the subject in bare feet. Body mass was measured on a calibrated physician scale. Body mass index (BMI) Z-score was calculated using SAS (gc-calculate-BIV.sas, available on the Centers for Disease Control and Prevention (CDC) website). Generalised joint laxity tests consisted of fifth-finger hyperextension greater than 90°, elbow hyperextension greater than 0°, wrist and thumb to forearm opposition and knee hyperextension greater than 0°.34 35 Anterior/posterior tibiofemoral translation was quantified using the CompuKT knee arthrometer (Medmetric Corp, San Diego, California) to measure total anterior–posterior displacement of the tibia relative to the secured femur. A modified Pubertal Maturational Observational Scale (PMOS) was used to classify the subjects into one of three pubertal categories (prepubertal, pubertal and postpubertal). The PMOS36 used both parental questionnaires and observations, all performed by a single investigator, to classify subjects into one of the three pubertal categories.12 37,–,39
Dynamic strength
Isokinetic knee extension/flexion (concentric/concentric muscle action) strength was measured on a Biodex System II (Shirley, New York) and consisted of 10 knee flexion/extension repetitions for each leg at 300°/s.40 Concentric hip abduction strength was measured on a Biodex System III (Shirley, New York) with the subject standing erect, fully supported, with a stabilisation strap around the pelvis and her hands gripping a stable hand rest. The test session consisted of five maximum-effort hip abductions with passive adduction repetitions at 120°/s.41
Landing biomechanics
Three-dimensional hip, knee and ankle kinematic and kinetic data were quantified for the contact phase of three DVJ tasks. Each subject was instrumented by a single investigator with 37 retroreflective markers placed on the sacrum, left posterior superior iliac spine, sternum and bilaterally on the shoulder, elbow, wrist, anterior superior iliac spine, greater trochanter, mid-thigh, medial and lateral knee, tibial tubercle, mid- shank, distal shank, medial and lateral ankle, heel, dorsal surface of the mid-foot, lateral foot (fifth metatarsal) and toe (between second and third metatarsals). A static standing trial was conducted in which the subject was instructed to stand still with foot placement standardised to the laboratory coordinate system. The static standing trial was used to calculate segment lengths as the estimated distance between the proximal and distal joint centre (eg, thigh segment distance was equal to the distance between the hip joint centre to knee joint centre). In addition, the static trial was used to calculate standing anatomical alignment measures. The mass and inertial properties for each segment (based on sex-specific parameters from de Leva42) were used to calculate the height of the centre of mass. This static measurement was used as each subject's neutral (zero) alignment; subsequent kinematic measures were referenced in relation to this position.43 The DVJ involved the subject starting on top of a box (31 cm high) with their feet positioned 35 cm apart. They were instructed to drop directly down off the box and immediately perform a maximum vertical jump, raising both arms while jumping for a basketball rebound.3
All trials were collected by a single investigator with EVaRT (version 4; Motion Analysis Corporation, Santa Rosa, California) using a motion-analysis system consisting of 10 digital cameras (Eagle cameras; Motion Analysis Corporation, Santa Rosa, California) positioned in the laboratory and sampled at 240 Hz. Prior to data collection, the motion-analysis system was calibrated based on the manufacturer's recommendations. Two force platforms (AMTI, Watertown, Massachusetts) were sampled at 1200 Hz and time synchronised with the motion-analysis system. The force platforms were embedded into the floor and positioned 8 cm apart so that each foot would contact a different platform during the stance phase of the DVJ.43
Following data collection, the motion and force data were further analysed in visual3D (version 4.0; C-Motion, Germantown, Maryland, USA). The procedures within visual3D first consisted of the development of a static model customised for each subject.43 3D marker trajectories from each trial were filtered at a cut-off frequency of 12 Hz.43 3D knee joint angles were calculated according to the Cardan/Euler rotation sequence.44 Kinematic and force platform data were utilised to calculate knee joint moments using inverse dynamics.45 46 The ground reaction force data were filtered through a low-pass fourth order Butterworth filter at a cut-off frequency of 12 Hz in order to minimise possible impact peak errors.47 48 Net external knee moments were described in this paper and represent the external load on the joint. Lower extremity kinetics and kinematics were calculated during the deceleration phase of landing from the stance phase of the DVJ. The deceleration phase was operationally defined from initial contact (vertical ground reaction force first exceeded 10 N) to the lowest vertical position of the body centre of mass. The left side data were used for statistical analysis. The described landing and biomechanical landing analysis techniques have demonstrated reliable measurements.43
Statistical analyses
Data were exported to SPSS (SPSS for Windows version 16.0, Chicago, Illinois) and SAS, V.9.1 (SAS Institute, Cary, North Carolina) for statistical analysis. Pearson correlation coefficients were calculated to assist in the initial selection of independent variables by removing non-significant correlates of the dependent variables; that is, associations with p>0.05 were not included in the regression models. For the model development, a multivariable linear regression with a backward elimination strategy was used to develop the prediction model for the continuous outcome of external knee abduction load. Inclusion and removal of each independent variable in the regression were examined. Those variables that did not reduce the R2>1% when removed were eliminated from the model. The ‘best’ model was determined based on the overall R2, MSEp, Mallow Cp and Fp.49 The final model was tested for validity based on examination of the variance inflation factor to quantify the degree of multicollinearity. Jackknife residuals were plotted, and along with the inspection of Cook's distance statistics, possible outliers were identified. Finally, the residuals were plotted, and the Kolmogorov–Smirnov statistic was used to test for possible deviations from normality.
Multivariable logistic regression analyses were performed to examine the dichotomised outcome variable. The cut-point used to classify the dependent variable status was >25.25 Nm of KAM, and this was based on published KAM data to determine a cut-score that would provide the maximal sensitivity and specificity for prediction of ACL injury risk during a DVJ (figure 1).5 22 Using this classification, subjects were categorised into a dichotomous (high KAM; ‘yes’ or ‘no’) dependent variable. All potential predictor variables following cluster variable reduction, as previously described, were introduced into a logistic regression model to predict high KAM status (>25.25 Nm of KAM). The logistic regression model was estimated using a logit link, assuming a binomial distribution for the outcomes and a general (unstructured) covariance structure. An α level of 0.05 was used to judge statistical significance in all models. The multivariable regression model's predictive accuracy was quantified with the use of the C-statistic, which measures the area under the receiver operating characteristic curve (ROC curve).
The regression equation developed in the training dataset was validated in the randomised subsample (n=100) by comparing predicted values of KAM and the actual measured values. Similarly, the logistic model was validated by solving the prediction equation for each subject in the validation group to determine into which group (high KAM vs low KAM) they would be classified. The non-informative prior probability of group membership observed in the test subjects included approximately 57% low KAM subjects and 43% high KAM subjects. The sensitivity, specificity and percentage correctly classified were calculated for the resulting 2×2 table of actual versus model-predicted classifications.
Results
Means and 95% CI for the dependent and independent variables used in the training dataset (N=598) model development are presented in table 1. The most parsimonious linear regression model, including the independent predictors (β±1 SE) (1) peak knee abduction angle (1.78±0.05; p<0.001), (2) peak knee extensor moment (0.17±0.01; p<0.001), (3) knee flexion range of motion (ROM) (0.15±0.03; p<0.01), (4) BMI Z-score (−1.67±0.36; p<0.001) and (5) tibia length (−0.50±0.14; p<0.001), explained 78% of the variance in KAM during landing. The optimised regression model coefficients were confirmed in the validation sample and yielded a significant correlation for the predicted peak KAM and the actual measured value (R2=0.83; p<0.001).
Means and 95% CI for the dependent and independent variables used in the training dataset (N=598) model development
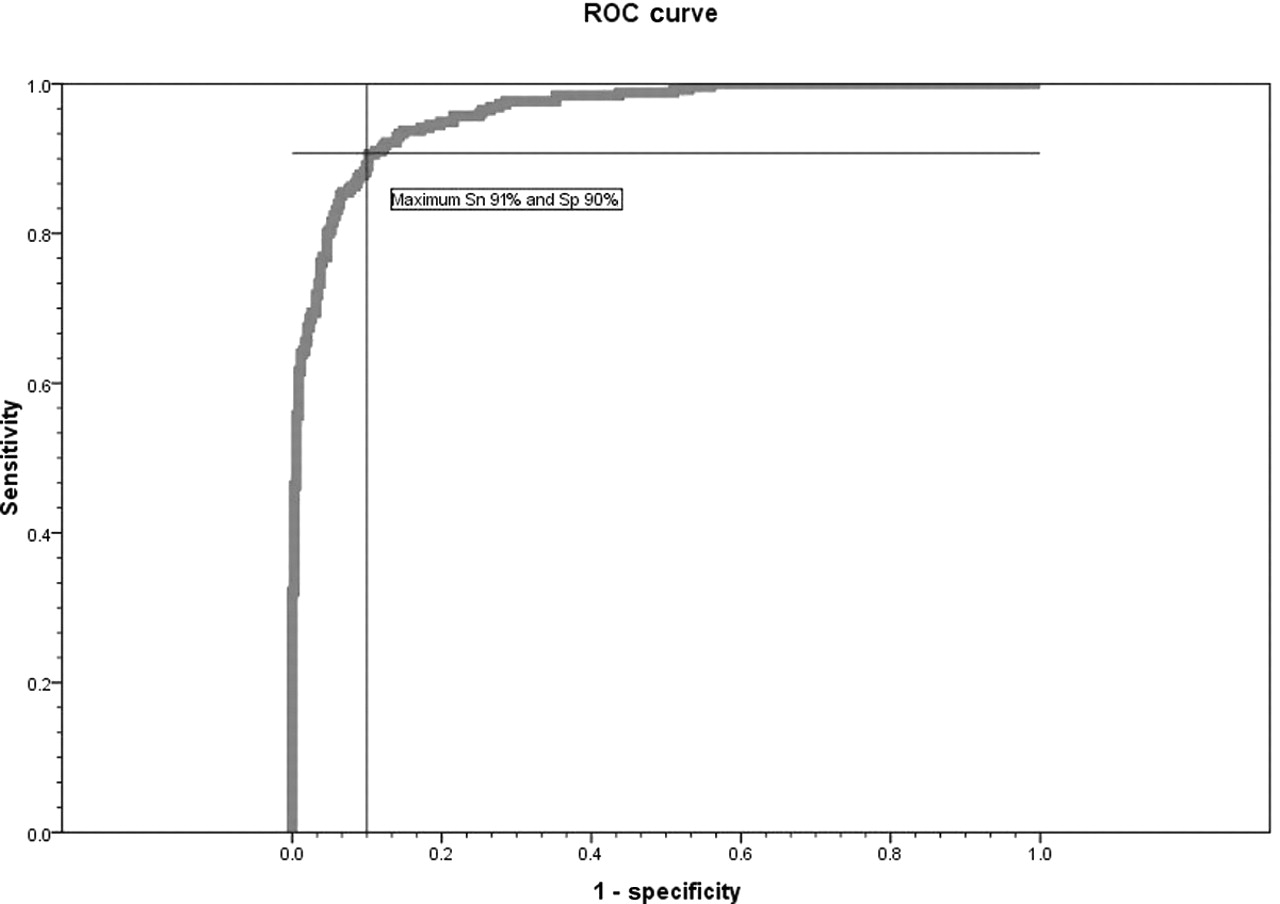
To further evaluate the prediction of KAM, variable selection was performed in a logistic regression analysis using the training dataset (N=598). The dependent variable of KAM was categorised into a dichotomous variable (high KAM; ‘yes’ or ‘no’), based on the established cut-point (25.25 Nm of KAM) which provided the most sensitive and specific KAM for predicting knee injury in females during landing. Importantly, the same independent predictors as found for the optimised linear regression model were optimal in the reduced variable set determined from the logistic regression modelling. Table 2 presents the ORs and 95% confidence limits for the predictors of high KAM. The final logistic regression model, which employed the independent predictors of peak knee abduction angle, peak knee extensor moment, knee flexion ROM, BMI Z-score and tibia length, predicted high KAM status with 85% sensitivity and 93% specificity (p<0.001). This model was predictive of high KAM status with a C-statistic of 0.96. The ROC curve for this model is presented in figure 4. The logistic model was validated by solving the prediction equation for each subject in the validation group and determining into which group (high KAM vs low KAM) they would be classified. The resultant prediction equation (C-statistic=0.959) yielded a sensitivity of 79% and a specificity of 89% to predict >25.25 Nm of KAM during landing.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curve determined in training dataset (N=598) for prediction of high knee abduction moment. The cross bar indicates the maximum sensitivity and specificity of the prediction model. Sn, sensitivity; Sp specificity.
OR estimates and 95% CI for independent variables used in training dataset (N=598) model development
Predictor variables were further assessed to determine if significant interactions with maturational status existed. A significant interaction was found between maturational status and knee abduction angle (p<0.01). In order to confirm that the multivariable regression that included peak knee abduction angle, peak knee extensor moment, knee flexion ROM, BMI Z-score and tibia length maintained robust prediction of KAM, both the linear and logistic models were tested separately in athletes grouped by maturational stage (prepubertal: N=120; pubertal: N=209; postpubertal: N=369). Linear regression modelling in prepubertal, pubertal and postpubertal female athletes accounted for 76%, 78% and 77% of the variance of continuous measurement of KAM, respectively (p<0.001). In addition, using the logistic model separately for each maturational stage, similar model performance based on C-statistic values was observed in the prepubertal (ROC=0.98), pubertal (ROC=0.97) and postpubertal (ROC=0.95) female athletes (p<0.001).
Discussion
Frontal plane knee alignment
The absence of active neuromuscular control, as evidenced by increased knee abduction motion,3 12 and passive stability of the joint, as indicated by increased joint laxity,36 demonstrate a puberty-related divergence between female and male athletes. The decreased active and passive controls of knee alignments may destabilise the knee and are purported to be measures related to increased risk of ACL injury in female athletes, as they mature.5 35 In the current dataset, maximum knee abduction alignment was also strongly correlated with the dependent variable KAM. Knee abduction angular measures at landing were 8° greater in athletes who subsequently experienced ACL injury compared with uninjured athletes.5 ACL injury likely occurs under conditions of high dynamic multiplanar loading of the knee joint.50 The knee joint, which is a hinge joint articulation of the body's two longest levers, is equipped with strong active muscular restraints to adequately dampen knee joint loads in motions aligned in the sagittal plane.51
The active restraints about the knee have a poor mechanical advantage to adequately control excessive frontal plane knee abduction motion commonly presented in young female athletes. In addition, females also demonstrate unbalanced contraction of the knee musculature that may further exacerbate the potential for increased KAM.52 Sell et al demonstrated that disproportional recruitment of the vastus lateralis musculature also influences increased anterior shear force in female athletes.53 54 Rozzi et al55 reported that female athletes demonstrate a disproportionate (four times greater) firing of their lateral hamstrings, as assessed by electromyographic (EMG) measurements, compared with males during the deceleration of a jump landing. Palmieri et al reported that females demonstrated unbalanced (decreased medial hamstrings and quadriceps) muscular recruitment that predicted KAM.52 Accordingly, a recent investigation of elite female handball and soccer players found that increased lateral quadriceps and decreased medial hamstrings was demonstrated by females who would go onto ACL injury.56 It has been hypothesised that an unbalanced or low ratio of medial to lateral quadriceps recruitment may combine with increased lateral hamstring firing to compress the lateral joint, open the medial joint and increase anterior shear force.57 Without the muscular power required to resist initial contact valgus or adequate medial knee musculature co-contraction to counteract initial contact KAM scenarios, the tibia and femoral articulation may open and translate allowing for excessive peak KAM loads52 57 Ultimately, movement patterns with high KAM may increase the potential for an athlete to stress their passive ligament structures that exceed the failure strength of the ligament.58 59
Active neuromuscular control is required to prevent potential high KAM and is required to maintain dynamic knee stability during landing and pivoting.58 60 61 The current findings indicate that disrupted mechanics of active muscular control may increase knee abduction alignments and lead to high KAM, which increase the risk of ACL injury.
Relative hamstrings recruitment
Increased hamstrings and quadriceps coactivation may be a potential method to protect the knee during sports-related tasks via increased dynamic joint stabilisation that limits the potential for increased knee abduction motions and reduces the potential of high KAM.59 61,–,63 Joint stability and absorption of KAM through hamstrings and quadriceps co-contraction may be necessary when the joint experiences high quadriceps activation during deceleration activities or when the passive structures are compromised.64 65 Withrow et al reported that increased hamstrings force during the flexion phase of simulated jump landings greatly decreased relative strain on the ACL.63 Hamstrings activation can decrease the load on the passive restraints of the knee,66 increase the knee joint compression force and stabilise the knee from external varus/valgus load.67 Electromyographical studies have demonstrated that females may have sex-related neuromuscular imbalances in muscle recruitment patterns proposed to be related to increased risk of ACL injury.53 68
Hewett et al reported that females demonstrated relative hamstrings recruitment (knee flexor moment), measured using inverse dynamics, that were threefold lower than males when decelerating from a landing.32 Accordingly, this group of females with greatly reduced relative hamstrings recruitment also demonstrated increased KAM compared with male subjects.32 The increased KAM was the only significant predictor of peak impact forces during landing in these female athletes.5 32
Ford et al reported that females showed an absence of matched increases in hamstrings muscle activation relative to quadriceps and overall low hamstrings EMG amplitude during increased intensity of the landing phase of a jump.69 This tendency of female athletes to preferentially activate the quadriceps relative to the hamstrings during high demand activities may limit their ability to maintain dynamic knee control during high-risk manoeuvres. This defined quadriceps dominance, or decreased recruitment of hamstrings relative to the quadriceps, has also been observed in elite female collegiate athletes.70 71 Female athletes reacted to a forward translation of the tibia primarily with a muscular activation of the quadriceps muscles, while male athletes relied on their hamstrings muscles to counteract the anterior tibial displacement.71 Sigward and Powers,72 examined a side-step cutting manoeuvre and found that skilled female soccer players had less relative hamstrings co-contraction than novice players. Decreased hamstrings relative to quadriceps strength and recruitment is implicated as a potential mechanism for increased lower-extremity injuries,63 69 73,–,75 and specifically ACL injury.76 The current study results also indicate that deficits in relative hamstrings recruitment also contribute to increased KAM, which creates a secondary link to increased ACL injury risk in female athletes.5 76 In corroboration with the current study findings, Lawrence et al reported that females in a decreased hamstrings strength group demonstrated increased relative knee extensor activity, ground reaction force and KAM when landing on a single leg.77 Cumulatively, this evidence indicates that decreased relative hamstrings strength and recruitment may underlie high KAM biomechanics and subsequent high risk for knee injury in female athletes.5 32 40 65 77
Sagittal plane knee alignment
Sagittal plane movement patterns during dynamic tasks may also contribute to the current sex disparity in non-contact ACL injury rates.7 11 Specifically, the relative decreases in knee flexion typically observed in females at initial contact and throughout stance during sports movements are proposed to elicit anterior tibial shear loads large enough to injure the ACL.54 78 Importantly, the current study results also indicate that small knee flexion motions during landing also contribute to high KAM.
The tendency to land with a straighter knee during high-intensity tasks could be exacerbated by early quadriceps, or delayed or decreased hamstrings recruitment, during a weight-bearing stance that are exhibited by female athletes.79 Chappell et al concluded that the increased anterior shear force demonstrated by female athletes was potentially due to the combination of increased quadriceps force, decreased hamstrings force and decreased knee flexion.7 A sagittal plane position of the knee near full extension when landing or cutting is commonly observed in video analysis of ACL injuries in female athletes.18 20 In addition, a prospective study indicated that female athletes that subsequently sustained ACL injuries demonstrated significantly less (10.5°) knee flexion during a DVJ than those that did not subsequently sustain injury.5
Increased hamstrings strength and recruitment may decrease ACL injury risk via increased relative hamstrings co-contraction that may lead to increased knee flexion and reduced KAM and potentially anterior tibial shear during dynamic tasks.5 8 18 20 32 64 68 80 81 The female subjects in the current study with decreased knee flexion ROM increase their potential for high KAM and subsequent risk for ACL injury. Improved lower-extremity movement strategies during high-risk sports movements, in particular those that contribute to increased sagittal plane motion and decreased frontal plane motions and KAM, may reduce risk and possibly prevent ACL injuries in female athletes.5 18 20
Skeletal growth
Beynnon et al82 reported that increased thigh length was an injury risk factor in female skiers. The current study results indicate that increased tibia length was associated with increased KAM. During peak growth (height and mass) velocity in pubertal athletes, the tibia and femur grow at rapid rates in both sexes.83 Rapid growth of the two longest lever arms in the human body initiate height increases concomitant with increased height of the centre of mass, making muscular control of the trunk more challenging. In addition, increased body mass with longer joint levers initiates greater joint forces that are more difficult to balance and dampen at the lower-extremity joints during high-velocity manoeuvres.12 84 85 During this developmental period, male athletes naturally demonstrate a ‘neuromuscular spurt’ (increased strength and power during maturational growth and development) to match the increased demands of growth and development, but do not demonstrate the same increases in KAM observed in females.12 37 84 86 87 Conversely, female athletes do not demonstrate similar neuromuscular adaptations to match the increase demands created from structural and inertial changes during pubertal development.12 37 84 86 87
Cumulatively, these factors contributed to the driving hypothesis of the current study that following the onset of puberty, rapid increases in bone length and body mass, in the absence of matched increases in strength and recruitment of the musculature of the lower extremity posterior chain, underlie the tendency for increased KAM during landing tasks in female athletes.12 88 If female athletes reach maturity in the absence of adaptation in core power and control to match whole body increases in inertial load, their tendency to demonstrate increased ground reaction forces and KAM during dynamic tasks is increased.12 84 85 89 91 The current results support this hypothesis, as increased tibia length contributed directly to increased KAM.
Body mass relative to stature
Increased body mass relative to height (BMI) has been implicated as a risk factor for ACL injuries, especially among female adolescent soccer players,25 92 college recreational athletes93 94 and female army recruits.95 However, other authors have reported that BMI in and of itself may not be directly linked to increased risk of ACL injuries in female athletes.96,–,98 Uhorchak et al95 reported that women with a body weight or BMI greater than 1 SD above the mean had a 3.2- and 3.5-fold greater risk of ACL injury than did those with lower body weight or BMI, respectively. A longitudinal study of children 5–12 years of age in youth soccer demonstrated that there is no gender difference in knee injury risk in prepubescent athletes. However, being older than 11 years of age was a significant risk factor for knee injury in girls. For female players older than 8 years, BMI was also a significant risk factor for increased knee injury risk.25 Based on these data, we chose to calculate BMI Z-scores, which yield a value for the BMI in terms of units of SD from the mean, based on data from the 2000 CDC growth charts, according to height, weight, age (months) and gender of each child. 99 These age- and sex-specific measures of BMI likely yielded a more appropriate measure of BMI for comparison among adolescent children than that used previously in epidemiological studies of injury risk. Accordingly, we found that increased BMI Z-score, or those children with increased mass relative to their height and that of their peers, was strongly related to the potential for increased KAM. Similarly, Griffin et al postulated that an increased BMI would result in a more extended lower-extremity position that would influence decreased knee flexion upon landing.93 The current study results indicate that increased measures (from the mean of the distribution) of age- and gender-specific BMI Z-score play a role in altered knee mechanics that are related to increased risk of ACL injuries in female athletes.92
Considering the significant short- and long-term debilitation associated with non-contact ACL injury, the prevention of these injuries is crucial. Currently, prevention appears to be the only effective treatment for these devastating injuries. The current study addresses the increased potential to reduce ACL injury and long-term osteoarthritis risk by defining the lower-limb mechanical parameters that underlie increased propensity to demonstrate high KAM and which increase the risk of ACL injury.5 100 Specifically, we have identified lower-extremity growth, recruitment and biomechanical strategies that contribute to high-risk landing biomechanics. An important initial step in the treatment of a particular injury aetiology is to define the risk factors for the injury.5 The next step should aim to define the mechanisms that modulate the identified risk factors so that appropriate application of treatment strategies can be employed to the population at risk. The current study has taken this important second step in ACL injury prevention by identification of the mechanisms that underlie increased high KAM. Future research should aim to apply these results to improve the identification of high-risk female athletes in all sport populations and target them with specific interventions designed to decrease knee abduction angles, and increase relative hamstrings recruitment and knee flexion ROM during dynamic tasks. If these future aims are achieved, an increased potential to counteract the effects of growth and development associated with maturation that increases ACL injury risk will be possible.
Summary and conclusions
Increased knee abduction angle and increased knee extensor torque with decreased knee flexion ROM, concomitant with increased tibia length and mass normalised to body height that accompanies growth, contribute to approximately 80% of the measured variance in KAM during landing. Athletes who demonstrate high KAM are more likely to sustain an ACL injury, and recent evidence indicates that this injury mechanism may also increase the risk for long-term osteoarthritis. Prior work indicates that female athletes who demonstrate increased KAM are more likely to achieve benefits from neuromuscular training. Hence, the results of this investigation, which identify the underlying mechanics related to increased KAM using lab-based measurement and analysis techniques, may improve the potential for identifying those likely to demonstrate this risk factor and may potentially better define neuromuscular training techniques to target the treatment of this risk factor for ACL injury.
What is already known on this topic
▶ Female athletes who demonstrate high knee abduction moment (KAM) during landing are more likely to sustain an anterior cruciate ligament (ACL) injury during competitive play.
▶ Female athletes who demonstrate increased KAM are more likely to achieve benefits from neuromuscular training that will reduce their risk of ACL injury.
▶ Prevention of ACL injury is currently the only method to prevent the high risk for long-term osteoarthritis associated with this type of knee injury.
What this study adds
▶ Increased knee abduction angle and increased knee extensor torque, with decreased knee flexion range of motion, concomitant with increased tibia length and mass normalised to body height that accompanies growth, contribute to approximately 80% of the measured variance in knee abduction moment (KAM) during landing.
▶ Screening for underlying mechanics related to increased KAM may improve the potential to identify those individuals likely to demonstrate this risk factor and to be at high risk for anterior cruciate ligament (ACL) injury.
▶ The current results may also help develop neuromuscular training techniques that target the treatment of high KAM as a significant risk factor for future ACL injury.
Acknowledgments
The authors would like to thank Boone County Kentucky, School District, especially School Superintendent R Poe, for participation in this study. The authors would also like to thank M Blevins, E Massey, B Blavatt and the athletes and coaches of Boone County public school district for their participation in this study. All authors are independent of any commercial funder, had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
References
Footnotes
-
Funding The authors would like to acknowledge funding support from National Institutes of Health Grant R01-AR049735, R01-AR055563 and R01-AR056259.
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the Cincinnati Children's Hospital Medical Center and Rocky Mountain University of Health Professions Institutional Review Boards.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Patient consent Obtained.