Article Text

Abstract
Recent data suggest that the risk of paediatric sport injury is high and constitutes a significant public health burden. A concern regarding long-term consequences of youth sports injury is the risk of developing osteoarthritis (OA) at a young age. Based on the available evidence, a link between youth sports injuries, particularly acute injury of the knee and ankle, and OA, is likely. Early OA development and intense participation in high-impact, high-stress elite sports at an early age also may be associated, but follow-up of elite athletes into the early adult years is needed to examine this relationship. Given that some antecedents of early adult-onset OA may be traced to child and adolescent sports injury and related surgery, and perhaps intense training regimens, it follows that efforts to prevent sports-related joint injury should begin during the childhood years. Based on the results of recent research evidence, programmes addressing prevention of youth sports injuries may provide the rewarding results of OA prevention.
Statistics from Altmetric.com
Participation in children's and youth sports is increasingly popular and widespread in Western culture. In the USA, for example, approximately 27 million children and adolescents between the age of 6 and 17 years (about half of all the US children and adolescents) participate regularly in team sports, and an untold several million more are involved in individual sports.1 Trends over recent decades include increased numbers of participants, particularly girls, increased duration and intensity of training, earlier specialisation and year-round training, and increased difficulty of skills practised. Physical activity has important and wide-ranging health benefits, but engaging in sports and recreational activities at a young age also involves risk of injury.2
The young athlete may be particularly vulnerable to musculoskeletal injury owing to such growth-related factors as the adolescent growth spurt, susceptibility to growth plate injury, maturity-associated variation, non-linearity of growth, selection for heavier children and adolescents in sports such as football,3 4 and immature or underdeveloped coordination, skills and perception.5 Although problems do not ordinarily arise at normal levels of activity, the more frequent and intensive training and competition of young athletes today may create conditions under which these risk factors exert their influence.
Recent data suggest that the risk of youth sport and recreation injury is high and constitutes a significant public health burden. In a recent report,6 65% of all sports-, recreation- and exercise-related injury visits to the US emergency departments in 2000 and 2001 (out of 4.3 million visits) were sustained by individuals aged 19 years of age or younger. The incidence of sports injury rises dramatically through the middle- and high-school years, subsiding during adult life.6 A concern regarding long-term consequences of youth sport injury and sports participation is the risk of developing osteoarthritis (OA) at a young age.7 8
The objective of this article is to evaluate the long-term musculoskeletal outcomes of youth sports injuries and participation by reviewing the epidemiology of OA, acute injury and OA, frequency and severity of knee and ankle injury, epiphysial growth plate injury and OA, OA and level of sports participation, injury-prevention research in paediatric sports and prevention of OA during childhood.
Epidemiology of OA
OA is a clinical syndrome that results from a generally progressive loss of articular cartilage (dense connective tissue cushioning the ends of the bones and allowing for ease of joint movement) accompanied by attempted repair of cartilage, remodelling and sclerosis of the subchondral bone and in many instances the formation of subchondral bone cysts and marginal osteophytes, or bone spurs.9 OA is the most common form of arthritis and is a major cause of disability in adults aged 65 and older.10 Features conventionally defining radiographic OA in epidemiological studies include joint space narrowing, osteophytosis, subchondral sclerosis, cyst formation and abnormalities of bone contour.11 Symptoms of OA include joint pain, aching, tenderness, stiffness and limitation of movement.12
In the USA, OA affects 13.9% of adults aged 25 and older, and 33.6% (12.4 million) of those 65 and older.13 From 1995 to 2005, the number of Americans affected with clinically defined OA (based on the presence of symptoms and physical findings) has grown from 21 million to nearly 27 million in USA, probably reflecting the ageing of the population and the obesity epidemic.10 The number of adults 65 years of age and older is expected to double from the year 2010 to 2040, most likely contributing to a rise in the prevalence of OA and a greater burden for our nation's healthcare systems for the treatment of OA.14 Knee OA, the most frequent form of lower-extremity arthritis, contributes to 418 000 knee-replacement procedures in the USA annually and, in 2006, accounted for 496 000 hospital discharges and $19 billion in hospital charges.15
Oliveria et al16 reported the age- and sex-standardised incidence rates (incidence of new diagnosis by physician) of symptomatic hip, knee and hand OA (presence of symptoms with radiographic evidence) to be 88 240 and 100 per 100 000 person-years, respectively. Recently, Murphy et al17 estimated the lifetime risk (based on survival to the oldest age group) of developing symptomatic knee OA to be about 45%, rising to 66% in obese persons and the lifetime risk of developing symptomatic hip OA to be approximately 25%.18 Women, from perimenopausal ages and older, are more likely to develop OA of the knee, hip and hand than are men.19
The aetiology for the development and progression of OA is complex and likely involves an interplay of systemic (eg, age, sex, ethnicity, bone density, hormonal factors, genetics and nutrition) and biomechanical factors. Examples of biomechanical factors include prior joint injuries, obesity, occupation, sports and physical activity, malalignment, muscle weakness and abnormal joint biomechanics, including those associated with congenital anomalies like hip dysplasia.20 21
OA and acute sport injury
Although OA is typically a condition that presents during the adult years, in some instances the antecedents of this condition may be traced back to childhood or adolescent joint injury.
Knee
At the knee, OA in adults may be associated with a variety of joint injuries and damage, including fracture of the articular surface, prior joint dislocations, and ligament and meniscal ruptures.22 In a study of 1321 former medical students (mean age 22 years), joint injury at cohort entry or during a median 36-year follow-up significantly increased the risk of knee OA (RR=5.17; 95% CI 3.07 to 8.71).23 Of 47 men with knee injury during adolescence or young adulthood (mean age=16 years), 15 (32%) reported that the injury occurred during sport activity. Notably, the cumulative incidence of knee OA by age 65 in this study was 13.9% in participants who had a knee injury during adolescence or young adulthood and 6% in those without injury during this stage of life (RR=2.95; 95% CI 1.35 to 6.45); the cumulative incidence of knee OA by age 65 among those with knee injury due to sport during adolescence or young adulthood was not reported, although it is likely higher than the incidence among those without injury.
Anterior cruciate ligament
Von Porat et al24 reported on the prevalence of OA among Swedish male soccer players 14 years after anterior cruciate ligament (ACL) rupture (N=219; age range at injury=16–42 years). The incidence of radiographic advanced degeneration was 41% in the injured knees and 4% in the uninjured knees with no difference in incident OA by surgical or non-surgical interventions post-ACL injury. Similarly, among 102 Swedish female soccer players injured before the age of 20 years, the prevalence of radiographic OA was 51% compared with 8% in the uninjured knee, 12 years later.25
Meniscus
Athletes have commonly received meniscectomies (removal of part or entire damaged meniscus) after meniscus injury, complicating the examination of the association between meniscus tears and knee OA. The meniscus is a load-bearing cartilaginous structure of the knee, and removal of part or all of this tissue is a risk factor for knee OA due to the resulting alteration and magnification of stresses across the knee.26 Lohmander et al27 reviewed 41 follow-up studies of surgically treated isolated meniscus tears suggesting that roughly 50% of those undergoing meniscectomy 10–20 years earlier had radiographic knee OA. Although the mean age of patients diagnosed as having traumatic meniscal injuries was about 30, the age range included adolescents.27 In long-term follow-up studies of young athletes with meniscus surgery, more than 50% had knee OA and associated pain and functional impairment.28,–,34 Follow-up studies of young non-athletes exposed to meniscectomy during adolescence are consistent with these results.28 29 32 35
Ankle
Although the prevalence of ankle OA is much lower than the knee or hip, ankle OA is much more likely to be post-traumatic.36 Population-based studies of ankle injury and OA are lacking, particularly those examining the impact of injury during youth sport, but prior ankle trauma among patients with ankle OA is commonly reported. Valderraban et al37 evaluated retrospective data from medical charts in 30 patients referred to an ankle arthritis centre with post-ligamentous-traumatic OA, and 18 of a total of 33 ankles with OA (55%) were sprained during sport (mean age 24, range 15–38), with 39% (seven of 18 ankles) of these injuries occurring during adolescence (ages 15–19). Although not specific to youth sport, Zinder et al38 examined the prevalence of ankle OA following a history of ankle sprain in retired professional football players, many of whom played football during adolescence. Retired players suffering at least one ankle sprain in their professional careers had 2.3 times the prevalence of ankle OA (8.9%) than those without ankle injury (3.8%). The authors did not report whether some of these ankle sprains experienced during professional play were recurrent injuries beginning during youth sport, a likely scenario considering that the rate of recurrence of ankle sprains may be as high as 80% among athletes.39
Frequency and severity of knee and ankle injury
Given the relation between joint injury, particularly ACL or meniscal injury and subsequent OA, knowledge of the incidence and severity of these injury types in youth sports is necessary. A systematic review of the incidence and distribution of injuries in youth sports revealed that the knee and ankle are the most common injury locations.40 In a nationally representative sample of 100 high schools involved in nine sports during the 2005–2007 school years, the second most frequently injured body site among athletes was the knee (1383 injuries accounting for 15.2% of all injuries), behind the ankle (20.9%).41 However, the knee was the most common severely injured (>21 days time loss) anatomical location (29%) and accounted for 44.6% of all surgeries.42 The 1383 practice- and competition-related knee injuries occurred during 3 551 000 athletic-exposures (AEs) for an overall rate of 3.89 knee injuries per 10 000 AEs. The most common knee injuries were ligament tears (45.4%), contusions (15.2%) and torn cartilage (8.0%).
Ankle injuries constitute the most common injury in children's and youth sports, and accounted for 22.6% of all injuries sustained by high-school athletes during the 2005–2006 school year.40 43 During this period, an estimated 326 396 ankle injuries occurred nationally, yielding an injury rate of 5.23 ankle injuries per 10 000 AEs.43 During 2005–2008, the US high school injuries most often involved the ankle (28.3%), followed by the knee (16.8%).44 Ankle injuries were most frequently diagnosed as ligament sprains with incomplete tears (83.4%), followed by fractures (5.2%). During 2005–2008, recurrent injuries, which accounted for 10.5% of all injuries affecting the nationally representative sample of 100 high schools, most often involved the ankle (28.3%), followed by the knee (16.8%) and head/face (12.1%).44
Epiphysial growth plate injury and OA
Growth plate cartilage is less resistant to stress than adult articular cartilage, and is also less resistant than adjacent bone to shear and tension forces.45 In addition, the growth plate may be two to five times weaker than surrounding fibrous tissue.46 For these reasons, forces experienced during injury that may result in a complete ligament tear or joint dislocation in an adult or older adolescent may produce a separation of the growth plate in a child. Emergency department data indicate that physial injuries account for between 15% and 30% of all skeletal injuries in children.47
Disturbed physial growth as a result of sports injury can result in limb-length inequality (LLI) (paired limbs are of unequal length), angular deformity or altered joint mechanics.48 OA may result from chondral damage at the time of growth plate injury, articular incongruity or joint malalignment.49 50 For example, articular surface incongruities may increase local contact stresses that accelerate the development of OA.51 Whether an arrest of growth occurs depends on several factors as summarised in table 1.
Factors related to growth insult
A systematic review of 25 case-series reports of sports-related growth plate injuries reported that 38.3% of 826 acute cases were sport-related, and among these 14.9% were associated with some degree of growth disturbance during short-term follow-up.52 These injuries were incurred in a variety of sports, although football was most often reported.
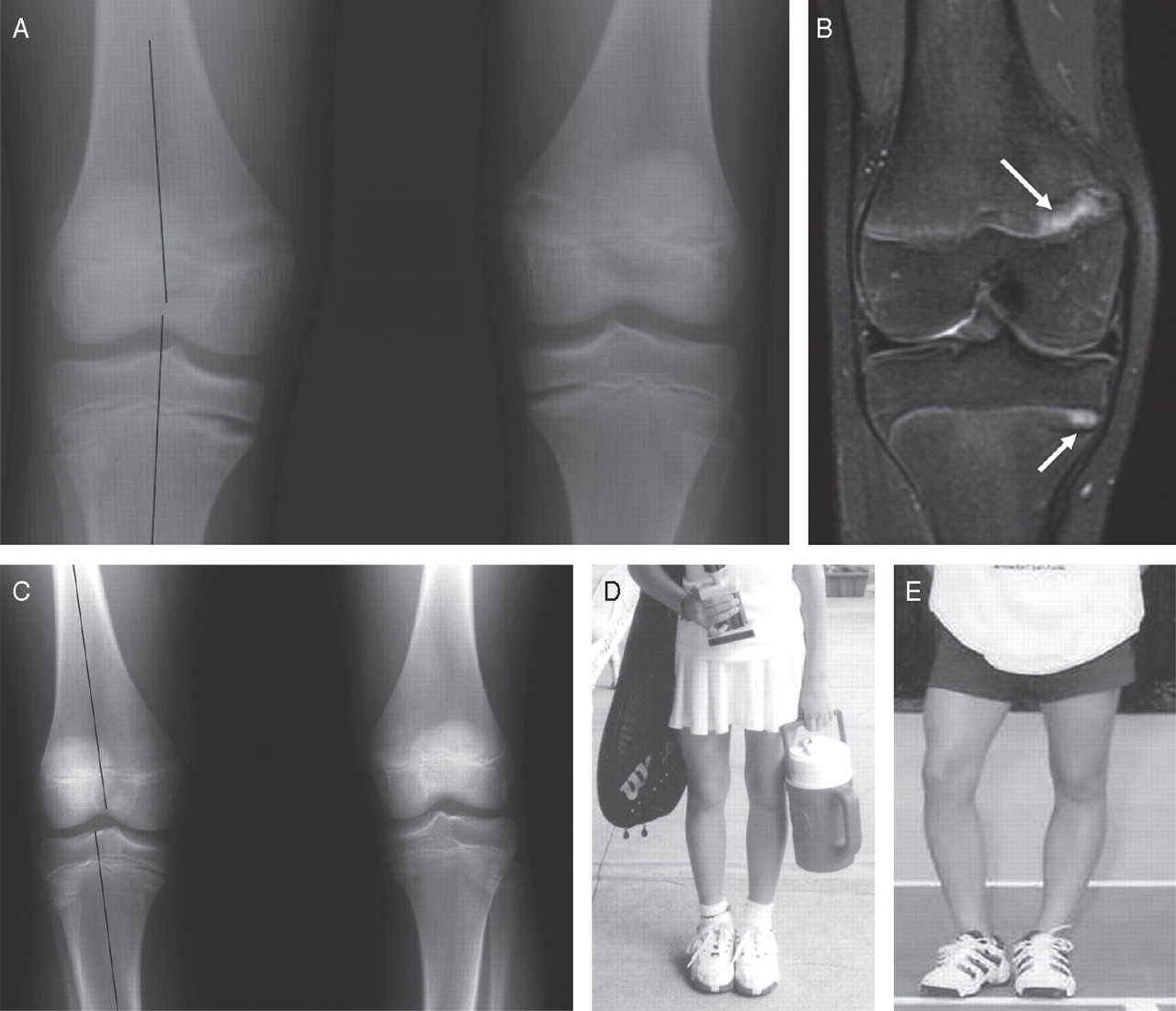
Many reports also suggest that stress-related physial injuries affect young athletes participating in a variety of sports.52 Although most of these injuries resolved without growth complication during short-term follow-up, reports are accumulating of stress-related growth disturbance in young athletes, including partial or complete premature epiphysial closure and deformity.53,–,60 These data indicate that sport training, if of sufficient duration and intensity, may precipitate pathological changes in growth plate and, in extreme cases, produce growth disturbance.52 An example of a 11-years-and-6-month-old female tennis player (Figure 1D) at initial visit who presented with physial widening of both medial distal femoral physes and both medial proximal tibial physes is shown in Figure 1A, B.58 This child was non-compliant and continued vigorous tennis training. Between her initial visit and age 17 years, 6 months she developed relative varus alignment of her lower extremities (Figure 1C, E).
{kind=link}
(A) Standing frontal radiograph of both knees showing physial widening of both medial distal femoral physes and both medial proximal tibial physes. Lines have been drawn along axes of the right femur to the tibia to illustrate normal varus alignment. (B) Coronal fast spin-echo proton density-weight image (TR/TE, 4000/34) with fat suppression of the right knee. Widening of the medial distal femoral and medial proximal tibial physes (arrows) shows a signal that is isointense to the rest of the physes. (C) Standing frontal radiograph of both knees obtaining 2 years after (A), during which time the child continued to play tennis intensely. There is relative varus alignment of both knees. Her physes have begun to fuse. (D) Frontal radiograph of patient obtained 1 month before (A) showing that she has normal alignment of her lower extremities. (E) Frontal photograph obtained 6 years after (A) showing relative varus alignment of her lower extremities. (A)–(E) are from Laor et al,58 reprinted with permission from the American Journal of Roentgenology.
Lishen and Jianhua61 followed 28 top-level gymnasts, aged 11–17 years, who were training 58–61 h per week. Gymnasts received a physical examination twice each year and an x-ray examination of the wrist once each year. During 9 years' follow-up, six of 18 girls and eight of 10 boys developed progressive wrist pathology. Initially, gymnasts developed chronic wrist pain associated with upper-extremity weight-bearing without radiographic abnormalities. Overtime, radiographs revealed stress changes in distal radial growth plate, with accompanying decreased range of motion at the wrist. Finally, radiographs revealed hindered radial growth, a relatively lengthened ulna and arthritic changes to the wrist.
The number of sport-related epiphysial injuries leading to early-onset OA is unknown. In the USA, most epiphysial injuries are cared for at tertiary centres or children's hospitals which typically do not follow patients after 18–20 years of age. However, Caterini et al62 found radiographic signs of OA in 11.8% of 68 patients followed for an average of 27 years from the initial ankle injury. A concern related to epiphysial fractures is that some may be dismissed or misdiagnosed as sprains.63 If the diagnosis is delayed or the treatment is not appropriate, some physial fractures can lead to premature physial closure, thereby resulting in angular deformity and/or shortening of an extremity.64 This may result in an LLI of the lower extremities, a condition associated with OA of the knee and hip among middle-aged to older adult populations.65,–,67
LLI may contribute to the development of radiographic knee and hip OA by causing asymmetrical joint mechanics between limbs during weight-bearing activities.68,–,70 To compensate for LLI, movement patterns may differ between limbs (ie, the longer limb may exhibit greater knee flexion or hip adduction during stance than the shorter limb to attempt to functionally shorten the longer limb).67 Changes in movement patterns to equalise limbs may result in altered or magnified forces across lower-extremity joints, leading to the development of OA.
OA and level of sports participation
The health of cartilage and other joint tissues requires regular joint loading. Self-reported physical activity and sports in children who participated in very active sports is associated with higher cartilage accrual rates than those who participated in less active sports (identified by the frequency of vigorous exercise or watching more than 3 h per day of television or video games).71 However, if loading is extreme in frequency or intensity, the tolerance of a joint could be exceeded, and OA may develop.9 Although data on this outcome in child and youth athletes are lacking, results of studies involving adult workers and athletes may be instructive. Repetitive and excessive joint loading that accompanies specific rigorous occupational activities increases the risk of developing OA in the stressed joints in adults.11 For example, in a systematic literature review of occupational activity and OA, Maetzel et al72 noted a strong positive relationship between work-related knee bending and knee OA. Similarly, in a review of elite sports participation and OA, Hunter and Eckstein73 concluded that adults who had normal joints and participated in low-impact exercises did not have an increased risk of developing OA of the knee or hip as they aged, independent of joint injury. However, elite athletes who perform high-impact activities and put undue stress on the joints may increase the risk of hip and knee OA,74 75 particularly in the presence of joint injury.73
Injury-prevention research in paediatric sports
The potential for OA after sport-related knee and ankle injury highlights an opportunity to improve population health and is a strong rationale to direct increased efforts toward primary prevention of these injuries. The results of recent randomised controlled trials (RCTs) directed at preventing these injuries show promise. Home-based balance-training programmes prevented self-reported reoccurrence of ankle sprains,76 reduced acute-onset injuries in high school basketball players77 and reduced all injuries, including ankle injuries, among high-school physical-education students.78 A significantly lower rate of ankle sprains among high-school basketball and soccer players exposed to both a pre- and in-season balance-training programme has also been reported.79
Two studies80 81 involving female adolescent team handball players and using a multifaceted training programme which included proprioceptive balance training demonstrated a protective effect for all injuries. Another study,82 also involving adolescent team handball players, demonstrated a protective effect of a structured warm-up programme to improve motor performance as well as neuromuscular control, balance and strength in decreasing risk of acute ankle and knee injuries.
Several studies have incorporated plyometric exercises (ie, repetitive exercise where a rapid eccentric muscle contraction is immediately followed by rapid concentric contraction) focusing on neuromuscular control in conjunction with strength and balance training of youth female soccer players. Although Steffen et al83 noted no effect of their programme on injury risk, Soligard et al84 reported a 29% decreased risk of lower-extremity injuries. Another RCT85 showed that cardiovascular conditioning, plyometrics and strength and flexibility training decreased the risk of injury compared with the control group.
Prevention of OA should start during childhood
Based on the available evidence, a link between youth sports injuries, particularly acute injury of the knee or ankle and OA, is likely. Early OA development and intense participation in high-impact, high-stress elite sports at an early age also may be associated, but follow-up of elite young athletes into their early adult years is needed to examine this relationship.
What is already known on the topic
▶ A high incidence of knee osteoarthritis (OA) in the years following anterior cruciate ligament injury or meniscal injury is well documented.
▶ Elite athletes who perform high-impact activities and put undue stress on the joints may increase the risk of hip and knee OA
What this paper adds
▶ Based on the available evidence, a link between youth sports injuries, particularly of the knee or ankle and OA is likely.
▶ Early OA development and intense participation in high-impact, high-stress elite sports at an early age may be associated, but longitudinal follow-up of elite young athletes into their early adult years is needed to examine this relationship.
▶ Efforts to prevent sport-related early-onset OA should begin during the childhood years.
Given that some antecedents of early onset OA may be traced to child and adolescent sports injury and surgery, and perhaps intense training regimens, efforts to prevent sports-related joint injury should begin during the childhood years. As stated by John H Klippel, MD, president and chief executive officer of the Arthritis Foundation, ‘Today's young athletes may become tomorrow's OA patients unless parents and coaches take an active role in sports-injury prevention.’86 Reduction in the dramatically high occurrence of sports injury during adolescence (eg, through injury-prevention programmes) may diminish the burden of early-onset OA.8 Injury and OA preventive measures that seem worthy of consideration include:
▶ the prescription of vigorous (but not excessive) motor activity for optimum joint development in children;71 vigorous activity would also help to reduce childhood and possibly adult obesity—a risk factor for knee OA;87
▶ systematic injury surveillance of young athletes to provide up-to-date information on the incidence and distribution of injury and to monitor injury trends;2 88
▶ preparticipation medical examination to identify injury status and predisposition to joint injury;89
▶ provide specific opportunities for knee-injury screening and subsequent neuromuscular training in high sports-injury risk groups—for example, a team from Cincinatti Children's Hospital has set up a combination of OA screening and training programmes for schools and teams across USA;90
▶ employment of pre- and in-season multiple component injury prevention strategies (warm-up, balance training and neuromuscular control);91
▶ include in the price structure funding to hire qualified sports medicine personnel who would provide early recognition and treatment of sports injury;92
▶ sports organisations should adopt available injury-prevention strategies, including injury surveillance, as part of their policies93 94
Based on the evidence, programmes addressing prevention of youth sports injuries may provide the rewarding results of OA prevention.8
References
Footnotes
-
Provenance and peer review Commissioned; externally peer reviewed.