Article Text

Abstract
Objective To compare the effectiveness and cost-effectiveness of eccentric loading exercises (ELE) with prolotherapy injections used singly and in combination for painful Achilles tendinosis.
Design A single-blinded randomised clinical trial. The primary outcome measure was the VISA-A questionnaire with a minimum clinically important change (MCIC) of 20 points.
Setting Five Australian primary care centres.
Participants 43 patients with painful mid-portion Achilles tendinosis commenced and 40 completed treatment protocols.
Interventions Participants were randomised to a 12-week program of ELE (n=15), or prolotherapy injections of hypertonic glucose with lignocaine alongside the affected tendon (n=14) or combined treatment (n=14).
Main outcome measurements VISA-A, pain, stiffness and limitation of activity scores; treatment costs.
Results At 12 months, proportions achieving the MCIC for VISA-A were 73% for ELE, 79% for prolotherapy and 86% for combined treatment. Mean (95% CI) increases in VISA-A scores at 12 months were 23.7 (15.6 to 31.9) for ELE, 27.5 (12.8 to 42.2) for prolotherapy and 41.1 (29.3 to 52.9) for combined treatment. At 6 weeks and 12 months, these increases were significantly less for ELE than for combined treatment. Compared with ELE, reductions in stiffness and limitation of activity occurred earlier with prolotherapy and reductions in pain, stiffness and limitation of activity occurred earlier with combined treatment. Combined treatment had the lowest incremental cost per additional responder ($A1539) compared with ELE.
Conclusions For Achilles tendinosis, prolotherapy and particularly ELE combined with prolotherapy give more rapid improvements in symptoms than ELE alone but long-term VISA-A scores are similar.
Trial registration number ACTRN: 12606000179538
Statistics from Altmetric.com
Tendinopathy of the Achilles tendon is a frequent cause of pain and disability in people with an active lifestyle.1 2 The condition is one of the most common overuse injuries in sports that repetitively load the Achilles tendon, such as athletics, orienteering, badminton, soccer and volleyball.1,–,3
Achilles tendinosis is the term used when structural changes in the Achilles tendon are observed on ultrasound. Painful Achilles tendinosis most commonly affects the mid portion of the tendon where collagen degeneration and new vessel and nerve formation exist in the absence of inflammation.4,–,7 Mid-portion Achilles tendinosis has proven very difficult to treat,8 with reported success rates of 0% to 36% for treatments including rest, anti-inflammatory medications, stretching and massage5 9 10 and from 70% to 85% with surgery followed by 4–6 months' rehabilitation.2 8 The current reference standard for the conservative treatment of Achilles tendinosis is an intensive programme of eccentric loading exercises (ELE) involving 180 eccentric calf muscle contractions daily for 12 weeks.9 10 This has a success rate of 60% to 100%.6 9 11 12 Clinical improvement is strongly associated with the disappearance of neovascularisation and structural changes in the tendon after ELE.6 Similar clinical and sonographic responses have been shown after the injection of polidocanol into the neovessels, but this requires ultrasound guidance and specialised ultrasonographic skill and equipment.13 14 Prolotherapy is a simpler injection treatment, not requiring ultrasound, where a solution of hypertonic glucose and local anaesthetic is injected alongside the painful areas of the tendon15 with the aim of stimulating inflammation followed by collagen deposition.16 A study of glucose/lignocaine injections versus saline injections into injured rat knee ligaments has shown additional thickening of healing ligaments but no differences in biomechanical properties.17 Prolotherapy also aims to reverse the neovascularisation accompanying tendinosis, but this effect is still speculative. Nonetheless, there is level 4 evidence of rapid and sustained reductions in pain and disability with courses of prolotherapy for both hip adductor tendinopathy15 and Achilles tendinopathy.18 19 Given that prolotherapy injections require much less time and patient effort than ELE, prolotherapy may be an attractive treatment alternative for people with Achilles tendinopathy.
There is evidence of a synergistic effect of ELE when combined with other treatments, such as low-level laser therapy20 and glyceryl trinitrate patches.21 This phenomenon has not been tested with prolotherapy. Thus, we performed a randomised clinical trial (RCT) of ELE, and prolotherapy injections were used singly and in combination for painful mid-portion Achilles tendinosis to examine differences in clinical and functional outcomes and treatment costs.
Methods
Setting and participants
The trial was conducted in Australia across five centres. The inclusion criteria were diagnosis of unilateral or bilateral mid-portion Achilles tendinosis with pain between 2 and 7 cm proximal to the calcaneal attachment in adults >18 years with activity-related pain for at least 6 weeks. The clinical severity of the tendinosis had to yield a score on the Victorian Institute of Sport Assessment—Achilles (VISA-A)2 of <80 of a maximum of 100 for participants involved in sport and <70 of 90 for people not involved in sport. The exclusion criteria were previous steroid or prolotherapy injections or surgery to the affected tendon, previous completion of >50% of the Achilles ELE protocol and any allergies or medical conditions that might limit completion of trial treatments.
The sample size was determined by the available resources and the slow recruitment rate rather than by an a priori sample size calculation. The participants were recruited from April 2006 to June 2007 via referrals from health professionals and through advertising in newspapers, brochures and a website. Applicant eligibility was assessed by phone interview followed by a clinical assessment and ultrasound with Doppler. Imaging protocols and reporting procedures were standardised across all the trial centres. The participants gave written consent at enrolment and were randomised to undertake ELE, prolotherapy injections or a combination of ELE and prolotherapy injections (combined treatment), using a computer-generated randomisation schedule with a block size of six. The randomisation schedule was generated and administered by telephone independently by the National Health and Medical Research Council Clinical Trials Centre in Sydney, Australia. Ethics approval for the study was given by the Griffith University Human Research Ethics Committee in Brisbane, Australia.
Patient evaluation
The primary outcome measure was the VISA-A questionnaire, an aggregate measure that comprised eight questions grading the domains of pain, stiffness, function in daily living and sporting activity. It has good reliability, validity and stability.2 The VISA-A questionnaire was administered during the clinical assessment at baseline and via telephone interview at 6 weeks and 3, 6 and 12 months. The criterion for success of treatment was set at an increase of 20 points in the VISA-A score. This was the minimum clinically important change (MCIC) estimated by investigators who estimate for the VISA-A Patella questionnaire used for patellar tendinopathy.22 We used this only because there were no published estimates of the MCIC for the VISA-A questionnaire. We defined fully recovered as attaining a score of ≥90.
Secondary outcomes included seven-point Likert scales for treatment satisfaction (from extremely dissatisfied to extremely satisfied)23 and the Patient Global Impression of Change (PGIC) scale (from very much worse to very much better)24 25 and 0 to 10 scales for worst pain in the last week, usual morning stiffness and limitation of usual activities. In the absence of MCIC values for these outcomes for Achilles tendinosis, we used MCIC values for other musculoskeletal conditions, that is, 1.75 for pain,26 1.75 for stiffness27 and 2.0 for limitation of activities,28 to assess the clinical importance of differences between groups. Achievement of two treatments goals, predetermined by each participant, was assessed. Use of other treatments was also recorded. All direct treatment costs related to the Achilles tendinosis from the preceding 3 months were recorded, including costs for general practitioner and specialist visits, outpatient visits with allied health professionals (eg, physiotherapists and podiatrists), aids and appliances and medications. These costs represented the costs to both the government and the patient. The cost of the interventions (ELE, prolotherapy and combined treatment) were calculated from the Australian Medicare Benefits Schedule with no patient copayment.29 Secondary outcome measures were administered at baseline (with the exception of the satisfaction and PGIC scales) and at 3 and 6 and 12 months. All outcome measures were administered by an assessor blinded to group allocation.
Treatment protocols
Each treatment was applied according to a standardised protocol described in a trial manual and adopted by all treating practitioners.
Eccentric loading exercises
The participants were instructed by a doctor or podiatrist in the ELE protocol described by Alfredson et al.9 The exercises are performed twice daily in three sets of 15 repetitions with the knee straight and three sets of 15 repetitions with the knee bent for a period of 12 weeks. The participants are told that the exercises may be painful but not to exceed an intensity of 4/10. As the pain eases over time, load is progressively increased by adding weights to a backpack. The participants had an initial training session and then reviews at 3, 6 and 12 weeks to check technique and progress. Written instructions for the exercises were supplied, and the participants kept a diary to document exercise load and compliance. Compliance was categorised by the percentage of the protocol performed.30
Prolotherapy injections
A doctor injected tender points in the subcutaneous tissues adjacent to the affected tendon with a solution consisting of 20% glucose/0.1% lignocaine/0.1% ropivacaine weekly for four to 12 treatments, using the technique described by Lyftogt.18 The tender points were most commonly the anterolateral and anteromedial margins of the tendon and on the most posterior aspect of the tendon 2–7 cm from the calcaneus attachment. At each point, 0.5–1 ml of solution was used to a maximum total of 5 ml. The number of treatments was determined by the time it took to reach a pain-free activity or until the participant requested to cease treatment.
Combined treatment
The protocols for ELE and prolotherapy injections were applied concurrently for this group. The participants in all the three groups were encouraged to gradually increase their activity levels while their symptoms reduced. They were discouraged from taking any anti-inflammatory medication but were allowed to take analgesics for pain relief.
Statistical analysis
Data analysis was performed blinded to group allocation on an intention-to-treat basis. Missing data occur intermixed with non-missing values (intermittent missing values), which are filled in by assuming a linear trend between the observed measurements. The proportion of missing final outcome measurements is small (<3% for the primary outcome measure), and they are imputed by carrying the last value forward method.31 The method assumes that there was no further change for an individual since the last available measurement. This assumption is not plausible in cases where the patients withdraw because of the treatment received. However, as the missing final measurements appear in the ELE and prolotherapy treatment groups only, the adoption of the last value forward method is conservative32 for estimating the effect size of the combined treatment group. The SAS version 9.1.3 software (PROC GENMOD) was used to analyse the longitudinal data using the generalized estimating equation (GEE), with a first-order autoregressive relationship (AR[1]) working correlation structure to account for within-patient correlation for repeated measurements.33 With the GEE, a normal distribution with an identity link was used for scale variable outcomes, whereas a binomial or multinomial distribution with a logit link was used for categorical variable outcomes. The assumption of normality within the framework of GEE was checked for scale variable outcomes. The effects of time (within-group differences), treatment (between-group differences) and treatment by time interaction (between-group differences over time) were included in all the models and assessed using the Wald χ2 test. Demographic and clinical variables at baseline were compared between treatment groups to assess the effectiveness of randomisation.
Economic analysis
A cost-effectiveness analysis for patient achieving MCIC at 12 months (responders) was performed. The ELE was the primary comparator, and the incremental costs and the additional benefit of prolotherapy and combined treatment was calculated. The incremental cost-effectiveness ratio (ICER; ie, additional costs divided by the additional benefit) is then used to determine the most efficient use of resources.33 A sensitivity analysis was undertaken to address any variation in the costs of the intervention, health care use and uncertainty around the effectiveness of the intervention. All the costs are reported based on the 2008 value of the Australian dollar currency ($A1≈€0.50).
Results
Patients
Figure 1 demonstrates the flow of participants through the study. A total of 145 people were interviewed by phone, from which 60 were clinically examined. A clinical diagnosis of mid-portion Achilles tendinopathy was made in 50 people. Of these, 43 had ultrasound findings of mid-portion tendinosis and consented to be in the study. A total of 15 participants were allocated to the ELE group, with 14 participants in each of the prolotherapy and combined treatment groups. By the end of the study, three participants had discontinued treatment, all of whom were from the ELE group. One participant had a heart attack, one discontinued because of time restraints and one sustained an unrelated injury during the study. One participant who was assigned to the prolotherapy group did not begin treatment because of work commitments.
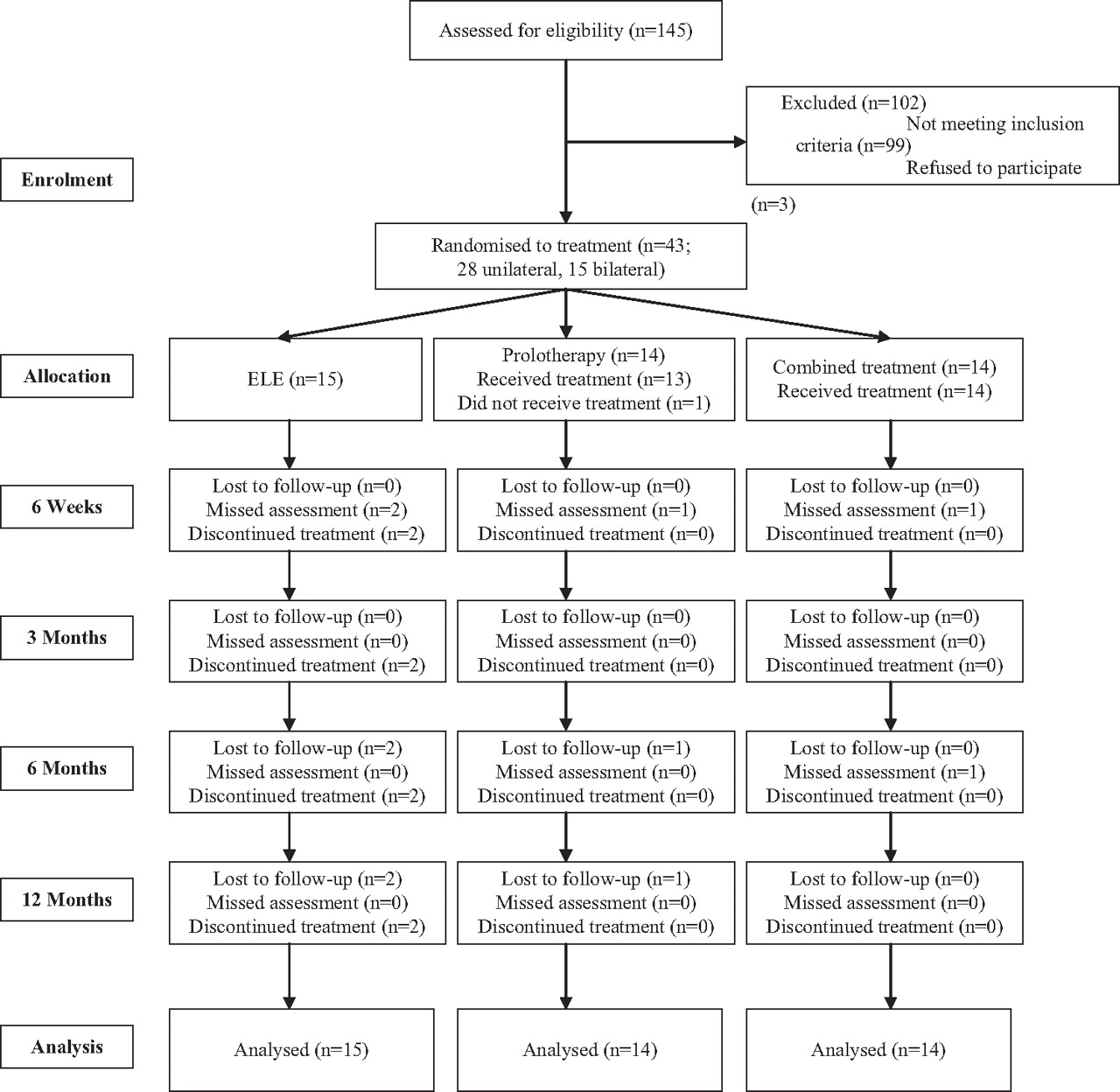
CONSORT flow diagram of trial applicants and participants.
The demographic and clinical characteristics of the three groups were similar, although the median duration of pain and the baseline VISA-A score in the combined treatment group were somewhat less than those in the exercise and prolotherapy groups (table 1).
Demographic and clinical characteristics and trial treatment details by treatment group
Treatment
The mean (SD) number of visits per group was 3.3 (1.9) for ELE, 9.5 (2.8) for prolotherapy and 8.7 (2.9) for the combined treatment. The mean (SD) number of injections per visit was 4.4 (1.7) for the prolotherapy group and 4.4 (1.6) for the combined treatment group.
In the ELE group, seven participants returned exercise diaries. Of these, exercise compliance was moderate (25% to 50%) for one, good (50% to 75%) for two and excellent (>75%) for four. In the combined group, nine participants returned exercise diaries. Of these, exercise compliance was moderate for one, good for three and excellent for five.
One adverse event was reported in the trial. A participant in the ELE group had a partial calf tear while playing tennis. An independent sports physician did not attribute this to the ELE programme.
VISA-A scores
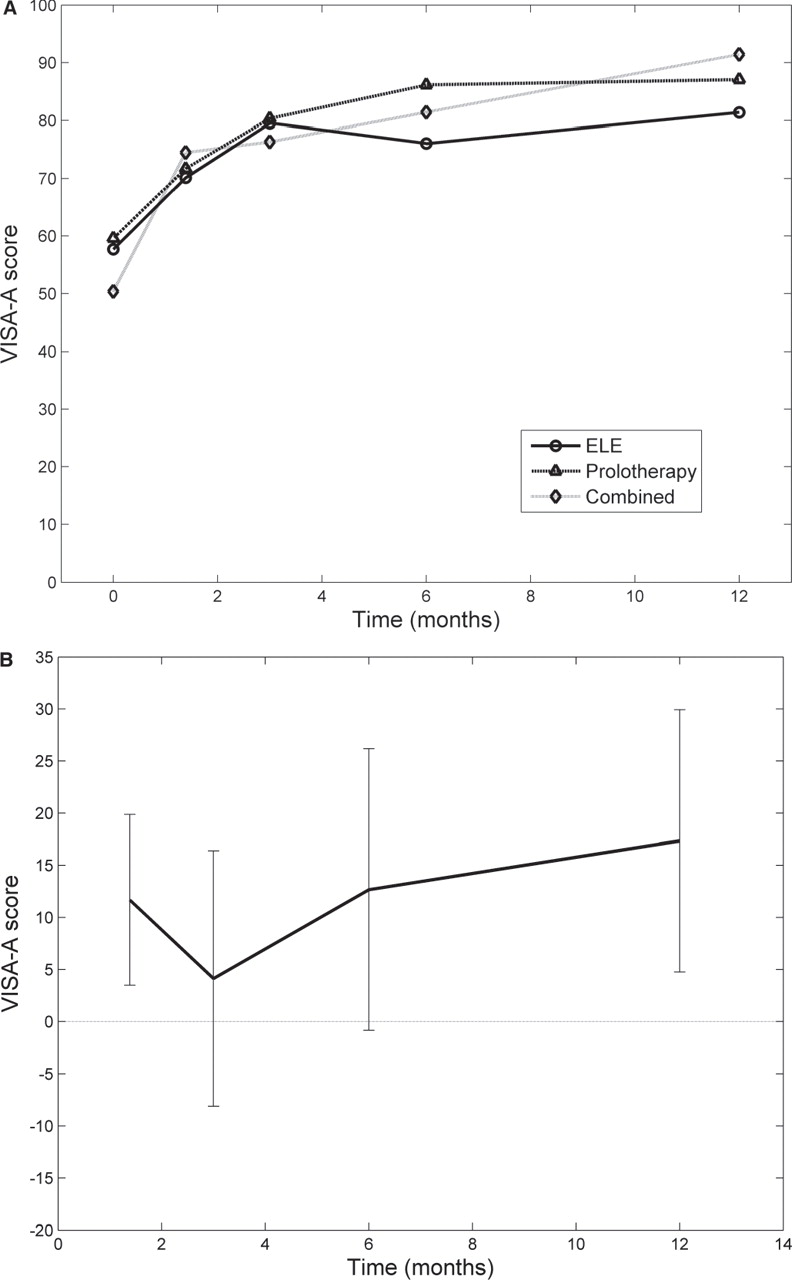
There were significant improvements in VISA-A scores at all times compared with those at baseline for all the groups (p<0.0005; fig. 2). These changes exceeded the MCIC threshold of 20 points by 3 months in all the groups. The mean (95% confidence interval [CI]) increase in VISA-A scores at 12 months was 23.7 (15.6 to 31.9) for ELE, 27.5 (12.8 to 42.2) for prolotherapy and 41.1 (29.3 to 52.9) for combined treatment. The increases from baseline for the ELE group were significantly less than for the combined treatment group at 6 weeks (difference −11.7; 95% Wald CI−3.5 to −19.9; p=0.005) and 12 months (difference −17.3; 95% Wald CI −4.8 to −29.9; p=0.007). There were significant differences between treatment groups over time (Wald χ2 statistics 23.7; df=8; p=0.003).

(A) Mean VISA-A scores by treatment group over 12 months; (B) Treatment differences (‘Combined’ relative to ‘ELE’) with associated 95% CIs.
The percentage within each group achieving the MCIC of 20 points in VISA-A scores from baseline increased significantly over time (p<0.0005) and was generally highest for the combined treatment group (table 2). However, there were no significant differences between groups or between groups over time.
Number (%) of participants achieving the minimum clinically important increase of 20 points or more in VISA-A scores from baseline over time by treatment group
The percentage achieving full recovery with a VISA-A score of ≥90 at 12 months was 53% for ELE, 71% for prolotherapy and 64% for combined treatment, but there were no significant differences between groups over time.
Pain, stiffness and limitation of activity scores
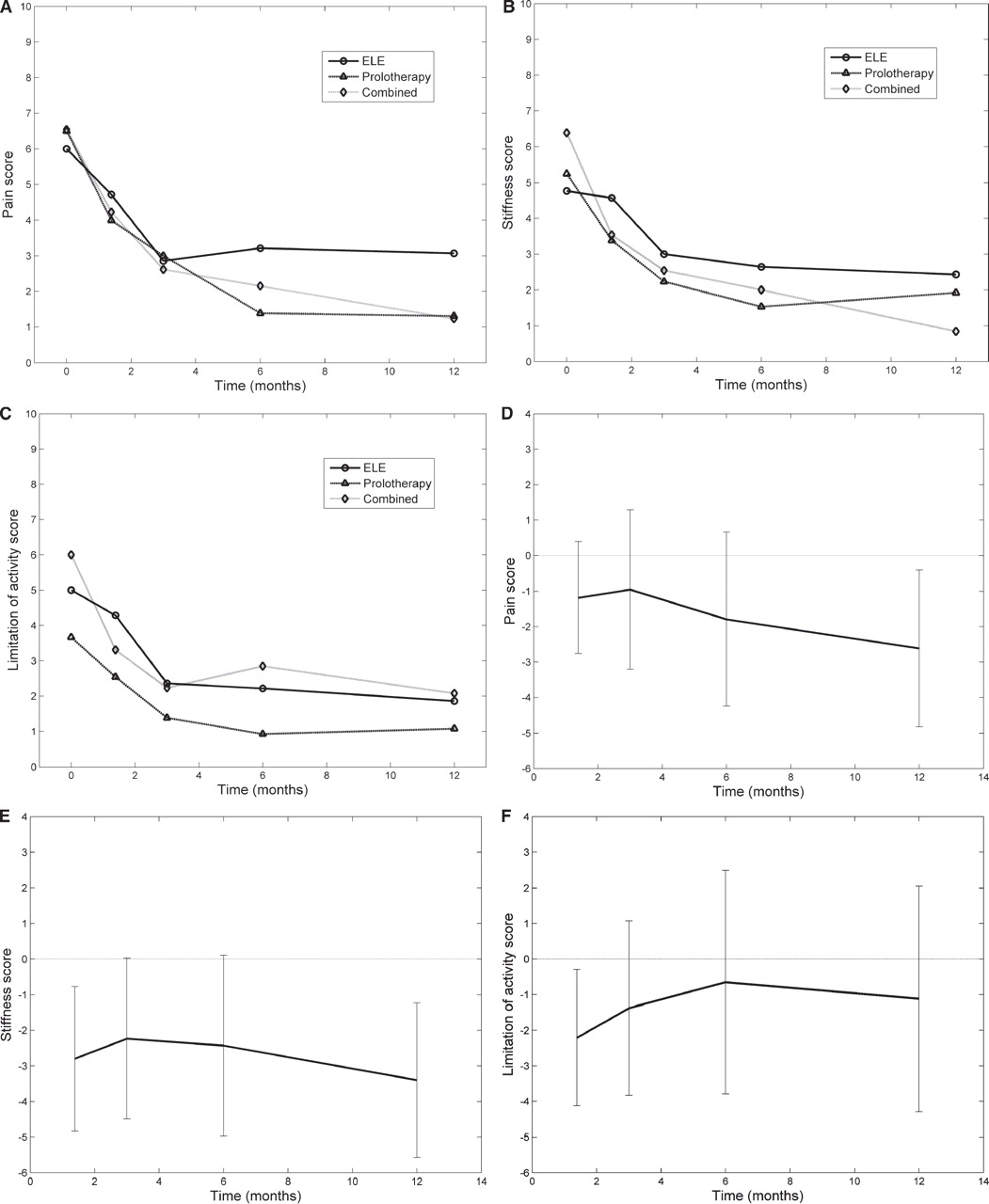
There were significant decreases in pain, stiffness and limitation of activity scores over time within all the groups (p<0.0005, fig. 3). The decreases in pain scores from baseline for ELE were significantly less by a clinically important difference than for prolotherapy at 6 months (difference 2.3; 95% Wald CI 0.3 to 4.4; p=0.028) and for combined treatment at 12 months (difference 2.6; 95% Wald CI 0.4 to 4.8; p=0.02). The difference between the treatment groups over time, however, was not significant overall (Wald χ2 statistics 13.2; df=8; p=0.105). The decreases in stiffness scores from baseline for ELE were significantly less by a clinically important difference than for prolotherapy at 6 months (difference 1.6; 95% Wald CI0.3 to 3.0; p=0.019) and for combined treatment at 6 weeks (difference 2.8; 95% Wald CI 0.8 to 4.8; p=0.007) and 12 months (difference 3.4; 95% Wald CI1.2 to 5.6; p=0.002). The difference between the groups over time was marginally significant (Wald χ2 statistics 16.0; df=8; p=0.043). However, it is cautioned that the significance must be adjusted for multiple testing of the three effects (within-group, between-group and between-group over time). The decreases in limitation of activity scores from baseline for ELE were significantly less by a clinically important difference than for combined treatment at 6 weeks (difference 2.2; 95% Wald CI0.3 to 4.1; p=0.024). The difference between groups over time, however, was not significant overall (Wald χ2 statistics 13.5; df=8; p=0.096).
{kind=link}
{kind=link}
{kind=link}
Mean scores for (A) pain, (B) stiffness and (C) limitation of activity for treatment groups over 12 months. Treatment differences (‘Combined’ relative to ‘ELE’) with associated 95% CIs for (D) pain, (E) stiffness and (F) limitation of activity.
It should be noted that for each of the above-mentioned clinically important differences between the groups, the CIs are very wide; so much smaller differences between the groups cannot be ruled out.
Satisfaction and global change ratings
There were no significant differences in satisfaction ratings or in PGIC ratings between the groups over time. The percentage reporting “satisfaction” or “extreme satisfaction” with treatment at 12 months was 50% for ELE, 69% for prolotherapy and 71% for the combined treatment. The percentage reporting a PGIC of “much improved” or “very much improved” at 12 months was 75% for ELE, 85% for prolotherapy and 64% for combined treatment.
Economic analysis
The costs of the specific interventions made up the largest proportion of total costs accounting for 65%, 94% and 73% of the total costs in the ELE, prolotherapy and combined treatment groups, respectively. Compared with ELE, prolotherapy cost an additional $90 in total and combined treatment cost $191 (table 3). For those additional costs, an additional 5.2% of the participants achieved a ≥20-point improvement in VISA-A score from prolotherapy at 12 months, whereas for the combined treatment, an additional 13% achieved this response. From the ICERs, it is apparent that combined treatment offers the best value for money (ie, the additional cost per responder is less than prolotherapy alone).
Costs and cost-effectiveness per participant by treatment group
These results were most sensitive to changes in the proportion of responders—for example, when this is reduced in the prolotherapy group by 10%, ELE is superior (lower cost and more responders) to prolotherapy. Reducing the cost of prolotherapy by 20% resulted in prolotherapy being superior to ELE. Reducing the cost of combined treatment by 20% resulted in a 45% reduction in the ICER (and vice versa for increases in the intervention costs). Varying the costs for healthcare by ±20% over the trial and follow-up periods made relatively little difference to the ICERs.
Discussion
This is the first trial to compare prolotherapy injections with the reference standard treatment of ELE. It offers a comprehensive picture of treatment inputs, clinical outcomes and costs to inform clinical decision making. Although the long-term outcomes summarised by VISA-A scores are similar, there are some differences in treatment inputs and reductions in symptoms. The ELE offers a low cost, self-management programme requiring considerable effort by the patient but with a slower reduction in symptoms. Prolotherapy is a relatively simple office procedure that offers a more time-efficient approach to treatment and a better reduction in pain and stiffness at 6 months but involves the pain of multiple injections, more doctor visits and a higher cost. Combined treatment requires the greatest input from the patient, clinician and health budgets but offers better reductions in pain and limitation of activity at 6 weeks and in pain and stiffness at 12 months and the lowest additional costs per additional responder. This is consistent with other studies comparing single treatment with combined treatment.20 21 The results could indicate some attention bias for those undergoing prolotherapy or combined prolotherapy, as this required an average of 9.5 and 8.7 treatments, respectively, compared with 3.3 visits for the ELE participants.
Strengths of this study include a comprehensive assessment of outcomes over 12 months, successful randomisation and blinding procedures, and a full economic evaluation. The blinded assessor was able to correctly identify the treatment group for 12 (28%) of 43 participants; he did not know in 15 of 43 (35%) cases, and was incorrect for 16 of 43 (37%) participants.
Although a trial design incorporating a no-treatment or at least a waiting list control group was desirable, we decided against this, believing that it would inhibit recruitment, which is already difficult enough in an RCT. We can find only one RCT on Achilles tendinopathy with a wait-and-see group.34 The outcomes for this approach were inferior to ELE in that trial and ELE in our trial.
To our knowledge, the only one other RCT of prolotherapy for tendinosis was for lateral epicondylosis, where injections of sodium morrhuate, glucose and local anaesthetic injections were more effective than saline injections.35 This is the first RCT of prolotherapy for Achilles tendinosis. The improvements in pain at 6–12 months were inferior to those in uncontrolled observational studies of prolotherapy.18 19 This could be because of our use of more comprehensive outcome measures, differences in patient populations, differences in technique or the greater experience of the treating doctors in previous studies. In the Results section, we have compared the treatment effects over time for the primary and the three secondary outcome measures separately. It should be noted that the overall experiment-wise type 1 error rate will be inflated when comparisons arisen from multiple outcome measures are considered.36
This trial provides valuable information for future treatment trials of Achilles tendinosis. Our concurrent collection of VISA-A scores and PGIC ratings allows an estimate of the MCIC for the VISA-A score. The best method for this is the sensitivity–specificity approach, which estimates the difference in VISA-A change scores between the much improved/very much improved group and the remainder.37 38 The MCIC is the threshold of this difference that discriminates between the two groups with equal sensitivity and specificity. Using this method, the MCIC value for the VISA-A questionnaire was 28, somewhat greater than the value used as the benchmark for success in this trial. At an MCIC of 28, the response rates at 12 months become 47% for ELE and 72% for combined treatment, a difference of 25%. This difference reduces the ICER for combined treatment to only $764 per additional responder.
Conclusions
In physically active people with painful Achilles tendinosis, most patients show sustained improvements with ELE and prolotherapy used singly or in combination, but that improvements in mean symptom scores occur earlier with prolotherapy and, particularly, with combined treatment than with ELE alone. Improvements in mean VISA-A scores are greater with combined treatment than with ELE alone, but the proportions achieving clinically important improvements in VISA-A scores are similar for all groups. Combined treatment involves a small increase in cost and temporary discomfort from treatment. A larger clinical trial is needed to further explore these findings.
What is already known on this topic
In painful Achilles tendinosis,
▶ ELEs are effective but the addition of other treatments may enhance their effect.
▶ There is level 4 evidence that prolotherapy injections are effective.
▶ The relative effectiveness of ELEs and prolotherapy used singly and in combination has not been established.
What this study adds
▶ In painful Achilles tendinosis, prolotherapy and, particularly, ELEs combined with prolotherapy injections give more rapid improvements in symptoms than ELEs alone, but long-term summary outcomes are similar.
▶ Cost-effectiveness analysis shows that ELEs was the lowest cost treatment, but when combined with prolotherapy, the cost per additional responder was exceptionally good value for money.
Acknowledgments
The authors thank Michael Yelland, Michael Oei, Vic Wilk and Scott Masters (Musculoskeletal Medicine Practitioners) for assessing and treating the participants in all the three groups; Lyndon Homeming (Podiatrist) for treating the participants in the ELE group; Mark Young, Kent Sweeting (Podiatrist) and Nicole Magner (Physiotheraist) for assessing the applicants; Mark Young (Sports Physician) for independently reviewing the participants who failed to improve; Natasha Morton, Elizabeth Pyke, Gemma Hynard and Xanthe Golenko for administrative assistance and Queensland X-Ray for standardising the ultrasound protocols.
References
Footnotes
-
Funding The trial was funded by grants from the Musculoskeletal Research Foundation of Australia, the Australian Podiatry Education and Research Foundation and the Griffith University Office of Research. Kent Sweeting was supported by a Primary Health Care Research, Evaluation and Development research fellowship. The funding bodies had no role in the study design; in the collection, analysis and interpretation of data; in the writing of the report or in the decision to submit the paper for publication.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Griffith University Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Patient consent Obtained.