Article Text

Abstract
Objective To study the injury characteristics in professional football and to follow the variation of injury incidence during a match, during a season and over consecutive seasons.
Design Prospective cohort study where teams were followed for seven consecutive seasons. Team medical staff recorded individual player exposure and time-loss injuries from 2001 to 2008.
Setting European professional men's football.
Participants The first team squads of 23 teams selected by the Union of European Football Associations as belonging to the 50 best European teams.
Main outcome measurement Injury incidence.
Results 4483 injuries occurred during 566 000 h of exposure, giving an injury incidence of 8.0 injuries/1000 h. The injury incidence during matches was higher than in training (27.5 vs 4.1, p<0.0001). A player sustained on average 2.0 injuries per season, and a team with typically 25 players can thus expect about 50 injuries each season. The single most common injury subtype was thigh strain, representing 17% of all injuries. Re-injuries constituted 12% of all injuries, and they caused longer absences than non re-injuries (24 vs 18 days, p<0.0001). The incidence of match injuries showed an increasing injury tendency over time in both the first and second halves (p<0.0001). Traumatic injuries and hamstring strains were more frequent during the competitive season, while overuse injuries were common during the preseason. Training and match injury incidences were stable over the period with no significant differences between seasons.
Conclusions The training and match injury incidences were stable over seven seasons. The risk of injury increased with time in each half of matches.
Statistics from Altmetric.com
The Union of European Football Associations (UEFA) has expressed its concern over the physical and mental load on modern professional footballers and the possible risk of injury as a result of such loads. A research project, specifically aimed at evaluating the exposure to football and the risk of injury for top-level football players in Europe, was, therefore, initiated in 1999.1
Studies that describe injury risk and injury patterns in senior men's football are typically conducted over one season2,–,12 or during tournaments,13,–,15 and some include only part of a season.16 17 Only few published studies have included data from two or more seasons,18,–,21 and thus, little is known about the natural variations between seasons.
The aims of this study were to investigate the injury characteristics in professional men's football teams and to describe the variations of injury incidence during a match, during a season and over seven consecutive seasons.
Material and methods
A prospective cohort study of European professional men's football was carried out during the years 2001–2008. The study covered seven consecutive seasons (July to May). In 2000, 14 of the top European men's clubs (clubs that had participated at the highest level in Europe over the last decade) were selected by UEFA and invited to take part in the study. Eleven teams agreed to participate and delivered complete data for the 2001/02 season.11 Over subsequent seasons, 12 more teams were selected by UEFA and included in the study, the inclusion criteria being that they delivered complete material over full seasons (table 1). Seven teams participated through all seven seasons. The full methodology is reported elsewhere.1 All contracted players in the first teams were invited to participate in the study.
Teams in the study over the seven seasons
Data collection
The study design followed the consensus on definitions and data collection procedures in studies of football injuries outlined by International Federation of Association Football (FIFA)22 and UEFA.1 Baseline data were collected once yearly, at the start of the season. Individual player exposure in training and matches was registered by the clubs on a standard exposure form. This included the first and second team, as well as national team exposure for all players, and was returned on a monthly basis. The team medical staffs were responsible for recording each injury immediately after the event on a standard injury form, and these were sent to the study group each month together with the exposure forms. The injury form provided information on the date of injury, scheduled activity, type and location of injury, re-injury, foul play and, from 2006/7, also the match minute when the injury occurred.
Definitions
The definitions applied in the study are shown in box 1. All injuries resulting in a player being unable to fully participate in training or match play (ie, time-loss injuries) were recorded, and the player was considered injured until the team medical staff allowed full participation in training and availability for match selection. Injuries were categorised under four degrees of severity based on the number of days' absence. All injuries were followed until the final day of rehabilitation.
Box 1 Operational definitions
Analyses
Analysis of variance was used for group comparisons of continuous normally distributed data. The variation of injuries during matches was analysed for two seasons (seasons 2006/07 and 2007/08). The χ2 test was used for comparison of proportions between groups and for pairwise comparisons. Yates' correction for continuity and the Bonferroni correction were used for multiple pairwise comparisons. Injury incidence was calculated as the number of injuries per 1000 player hours. The significance level was set at p<0.05.
The study design underwent an ethical review and was approved by the UEFA Football Development Division and the UEFA Medical Committee.
Results
There were, on average, 25 players per team (range 15–36).
Exposure
The exposure details are shown in table 2. In total, 566 000 h of exposure (475 000 of training and 91 000 of match play) were registered over the seven seasons. The average (mean) player participated in 34 matches and had 162 training sessions each season (median values being 35 and 173). The mean overall exposure to football during the full season was 254 h with 213 training hours and 41 match hours (median values being 269, 222 and 40).
Team, player and exposure characteristics from 2001 to 2008
Frequency and nature of injuries
In total, 4483 injuries were registered, with 2546 (57%) occurring during matches and 1937 (43%) during training. On average, a player sustained 2.0 injuries per season, resulting in 50 injuries per season in a team of 25. The types and locations of injuries are shown in table 3. Eighty-seven per cent of the injuries affected the lower extremities. Muscle strain, ligament sprain and contusion were the most common injury types. The thigh, knee, ankle and hip/groin were the most common injury locations.
Injury pattern by severity of injuries
The single most common injury subtype was thigh strain, representing 17% (n=743) of all injuries, with posterior thigh strains (hamstrings, n=525, 12%) more common than anterior ones (quadriceps, n=218, 5%). A team of 25 can thus expect about 10 thigh muscle strains each season, 7 of them affecting the hamstring muscles and 3 the quadriceps. Other common injury subtypes were adductor pain/strain (n=399, 9%), ankle sprain (n=318, 7%) and medial collateral ligament (MCL) injuries (n=220, 5%). Injuries resulting from trauma represented 81% in matches and 59% in training. Overuse injuries represented 28% of all injuries.
Injury severity
Severe injuries (causing absence of >28 days) accounted for 16% of all injuries.
The most common subtypes of severe injuries were hamstring strains (n=83, 12%), MCL injuries (n=63, 9%), quadriceps strains (n=48, 7%) and adductor pain/strain (n=42, 6%). The average (mean) team at this level can expect eight severe injuries per season. On average, each player missed 37 days due to injury each season. This means that approximately 12% of the season is lost due to injury if we assume that a season lasts 300 days.
Foul play
Twenty-one per cent (n=538) of the match injuries were due to foul play according to the referee, with the majority being due to foul play by an opponent (n=520). The most common foul play injuries were ankle sprains (15%), knee sprains (9%) and thigh contusions (10%). In the two seasons where the match minute of injury was registered (2006/07 and 2007/08), foul play injuries were evenly distributed among the two halves (74 vs 84, p=0.47).
Re-injuries
Re-injuries constituted 12% of all injuries, and they caused significantly longer absences than non re-injuries (24 vs 18 days, p<0.0001).
Variation of injury risk during matches
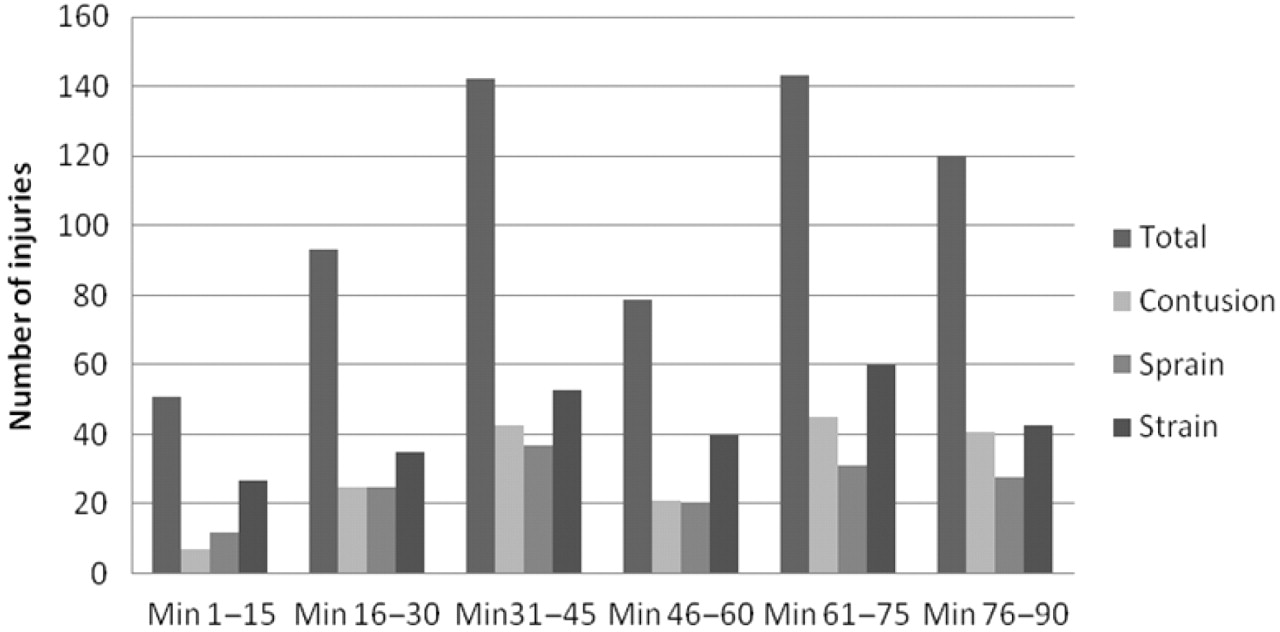
The incidence of traumatic match injuries showed an increasing tendency over time in both the first and second halves (p<0.0001; fig 1). A similar trend (increasing over time in each half) was observed for contusions (p<0.0001), ligament sprains (p=0.011) and muscle strains (p=0.005).

Distribution of traumatic injuries during a match (data from the 2006/07 and 2007/08 seasons).
Variations in injury incidence over a season
Figure 2 shows the distribution of traumatic and overuse injuries over the season. Traumatic injuries were more common during the competitive season (September to May), while overuse injuries peaked during the preseason preparation period in July.

Distribution of traumatic and overuse injuries over the football season.
Figure 3 shows the variations in the most common match play injuries during the season. The risk of sustaining a hamstring strain was substantially higher during the competitive season, while the risk of sustaining a quadriceps strain, ankle sprain or MCL sprain of the knee remained fairly equal.

Distribution of the most common match play injuries over the football season.
Variations in injury incidence over seven seasons
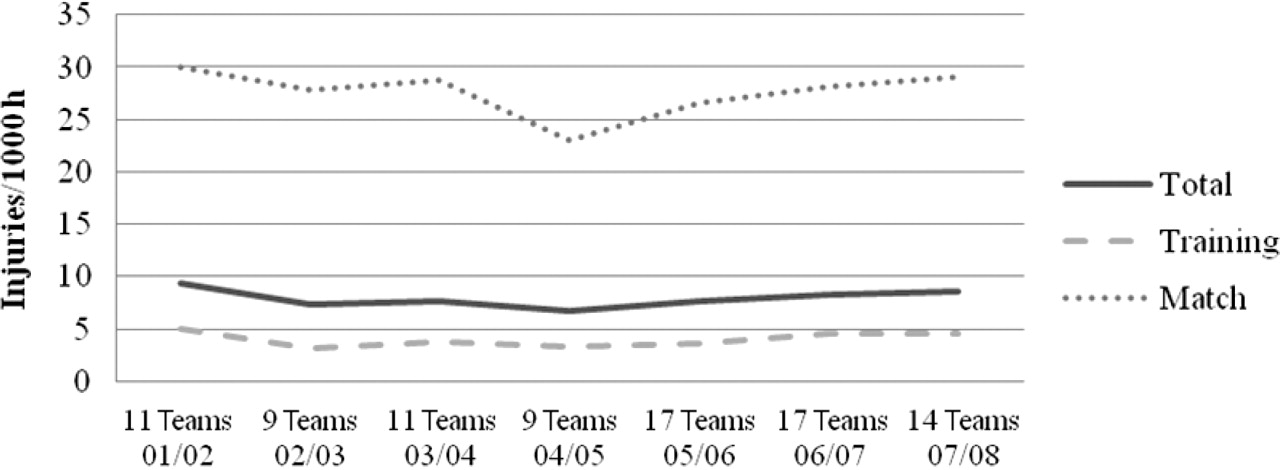
The mean total injury incidence for all teams during all seasons was 8.0±3.4/1000 h. The injury incidence during matches was significantly higher than during training (27.5±10.8/1000 h vs 4.1±2.0/1000 h, p<0.0001). The total injury incidence, as well as the training and match injury incidences, were stable over the period with no significant differences between seasons (fig 4).
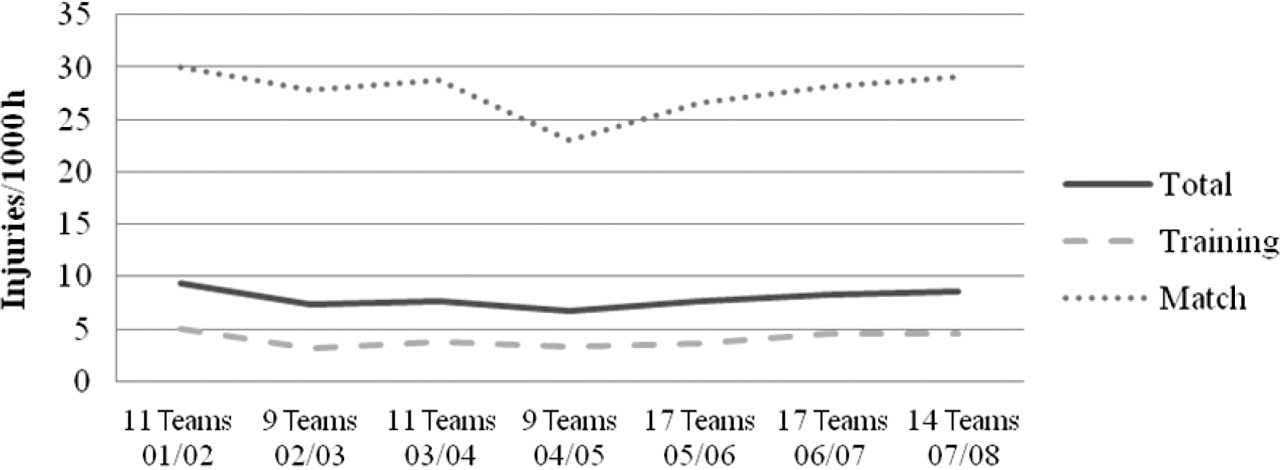
Incidence of injury per season across the seven-season study period (injuries/1000 h).
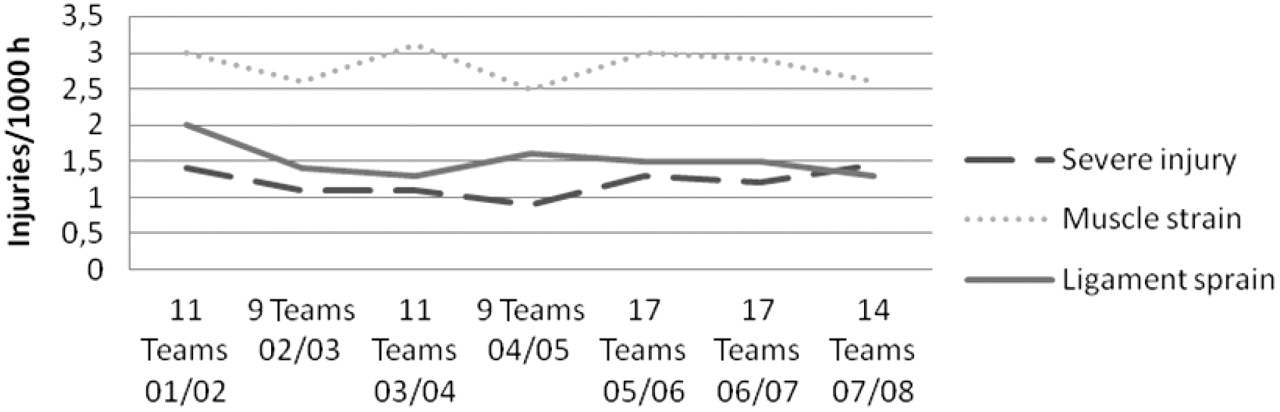
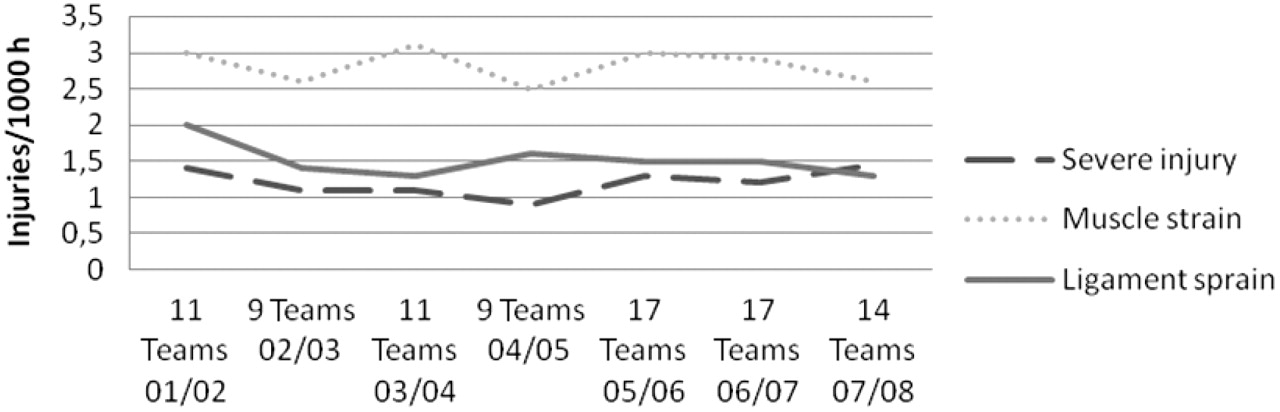
The incidence of severe injuries and muscle injuries did not differ significantly between seasons (fig 5). The risk of ligament sprains decreased between seasons 2001/02 and 2003/04 (p<0.05), remaining stable during subsequent seasons.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Injury pattern across the seven-season study period (injuries/1000 h).
Discussion
The principal finding in this study was that the injury risk in this group of professional teams has not changed over a 7-year period. Continuous data over several seasons are needed not only to observe the development of specific trends over time but also to screen for areas of concern and form injury prevention hypotheses.
Frequency and nature of injuries
The injury incidences in training and match play in our study are consistent with recent data from the Swedish Premier League,9 11 21 as well as in England and in Norway.20 23 An elite team with 25 players in the squad can expect about 50 injuries each season, half of them minor and causing absences of less than a week, but as many as eight or nine severe and causing absences of >4 weeks. Hamstring strain was the most common diagnosis, which is in accordance with findings in other studies carried out at elite level using the consensus study design. A typical 25-player squad can thus expect about seven hamstring strains each season. It can be speculated that the high risk of hamstring strain reflects the high intensity of modern professional football.
Reporting of concussions
Head injuries accounted for 2% of all injuries. This figure incorporates all types of head injuries including not only concussions but also facial fractures, lacerations and eye injuries. Over the 7-year period, only 34 concussions were registered, representing an incidence of 0.06 concussions/1000 h of exposure or, as a mean, one concussion per team every second season. When examining concussion rates, the figures may be vastly underestimated because the diagnosis of a concussion is dependent on a player volunteering his symptoms to medical personnel.24 Concussion may involve a graded set of clinical symptoms, which may or may not involve loss of consciousness.25 Hence, some of the other 33 head injuries sustained by the players in the present study may have led to unrecognised concussive injuries, and the incidence may have been underreported. A worrying finding is that, in spite of current consensus recommendations to ensure a structured rehabilitation with sufficient physical and cognitive rest following concussion, more than half of the players diagnosed with concussion returned to full training and match availability within 1 week.26
Re-injuries
Previous injury and inadequate rehabilitation are commonly suggested to be risk factors for football injuries.4 21 27 28 Recent studies in Scandinavian elite football, using the consensus statement definition of an early recurrent injury22 as in this study, have found re-injury rates between 22% and 30%.9 12 16 21 In the present study, the rate of re-injury was substantially lower (12%), with most injuries being strains and sprains. One possible explanation for the difference might be that top-level clubs in Europe have greater medical support, providing for more personalised rehabilitation of injured players. Still, one might speculate that improvements in controlled rehabilitation with functional tests before returning to team training and match play might reduce the risk of re-injury even more.29
Re-injuries caused longer absence than non-re-injuries, which is in accordance with previous findings.12
Increased injury risk towards the end of each half
The incidence of match injuries showed an increasing tendency over time in both the first and second halves. This increase was evident for the total of traumatic injuries, and the same pattern was seen for the three most common injury subtypes (strains, sprains and contusions). One might speculate that fatigue might be an explanation for these findings. Studies of physical demands in football have shown that fatigue is developed towards the end of a game, and the amount of high-intensity running and technical performance is lowered.30,–,32
Seasonal variations in injury incidence
The preseason period (mainly July) is predominantly devoted to physical training with few matches, which could explain the finding that overuse injuries were more common and traumatic injuries less common than during the rest of the season.
The incidence of ankle sprains, MCL injuries and quadriceps strains was fairly constant over the season. The incidence of hamstring strains, however, was low during the preseason period but two or three times higher during the competitive season (September to May), when most high-intensity matches are played.
Methodological considerations
The collection of data followed the international consensus agreements on procedures for epidemiological studies of football injuries recommended by FIFA and UEFA.1 22 In these papers, the strengths and limitations of injury surveillance studies such as this one are thoroughly discussed. Nevertheless, the obvious strength of this study is the plentiful, homogenous material on male professional players in Europe and the fact that the study is based on an injuryrecording system specifically developed to address the issue under review. Another advantage of studies at elite level is that official match data and other exposure data are frequently published on the UEFA website as well as the websites of the clubs. Our exposure data are believed to be accurate since it was regularly verified against official reports found on websites, in newspapers, etc.
A limitation of this study, and all prospective cohort studies, is that no causal relationship between findings can be established. However, studies like this are important sources for hypotheses which can be tested in further investigations.
What is already known on this topic
▶ The match injury incidence in professional men's club football is high.
▶ Hamstring strain is the single most common injury type at elite level.
What does this study add
▶ Injury incidence does not change over consecutive seasons.
▶ Injury risk increases with time in each half of matches.
Acknowledgments
The authors gratefully acknowledge the clubs involved in the study. The help we received from the medical personnel and contact persons is greatly appreciated: Rodolfo Tavana and Bill Tillson (AC Milan), Piet Bon and Edwin Goedhart (AFC Ajax), Leo Groenweghe and Jose Huylebroek (RSC Anderlecht), Joao-Paolo Almeida and Paulo Rebelo (SL Benfica), Egid Kiesouw (BV Borussia Dortmund), Gary Lewin (Arsenal FC), Bryan English and Alex Nieper (Chelsea FC), Dimitri Dobbenie, Jan de Neve and Michel D'Hooghe (ClubBrugge KV), Jordi Ardevol, Lluis Til, Gil Rodas, Ricard Pruna and Ramon Canal (FC Barcelona), Dieter Gudel, Oliver Dierk and Nikolaj Linewitsch (Hamburger SV), Francesco Benazzo, Franco Combi, Giorgio Panico, Cristiano Eirale and Pier-Luigi Parnofiello (FC Internazionale Milano), Fabrizio Tencone and Antonio Giordano (Juventus FC), Mark Waller (Liverpool FC), Roddy McDonald (Newcastle United FC), Mike Stone and Steve McNally (Manchester United FC), Hakim Chalabi (Paris St Germain FC), Nelson Puga (FC Porto), Cees-Rein van den Hoogenband and Luc van Agt (PSV Eindhoven), Ian McGuiness (Rangers FC), Denis Bucher (RC de Lens), Luis Serratosa (Real Madrid CF), Paco Biosca and Viktor Kirilenko (Shakhtar Donetsk) and Pierre Rochcongar (Stade Rennais FC). The statistical advice of Henrik Magnusson (Bsc) is also gratefully acknowledged.
References
Footnotes
-
Funding The study was funded by UEFA.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the UEFA Medical Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.