Article Text

Abstract
Objective To collect medical data on women's boxing.
Design Cross-sectional and longitudinal study.
Setting Medical examinations requested by Italian laws.
Participants A retrospective study was conducted on all female boxing competitions in Italy from April 2001 to December 2007. Sixty-one amateur female boxers were evaluated longitudinally.
Interventions (1) Retrospective study: All pre-/postmatch medical reports were analysed. (2) Prospective study: Breast, gynaecologic, brain, eyes, ear, nose and throat examinations were carried out.
Main outcome measurements (1) Retrospective study: Any injury assessed before/after the match. (2) Prospective study: Health problems which could be related to boxing activity.
Results (1) Retrospective study: Data from 5600 examinations were collected. Precompetition, a medical problem was recorded in three athletes (one conjunctiva hyperemia, one zygomatic bruise, one eyelid haematoma). Post competition, 51/2800 medical checks showed mild common injuries, such as soft tissue facial lesions, epistaxis and hand-wrist problems. Only one concussion was recorded with hospitalisation (for a thorough evaluation). Another athlete was hospitalised for a nasal fracture. (2) Prospective study: Two fibroadenomas, three ovarian cysts and one intramural uterine myoma were diagnosed. In four boxers, non-specific electroencephalographic abnormalities were detected, however, with a normal brain MRI in three (the fourth is still waiting for the radiologic procedure). Nasal septum deviation was common (42.6%) and a transmissive hypoacusia was observed in two athletes. No major eye injuries were reported.
Conclusions Female boxing seems to be a safe sport with a very low incidence of events requiring hospitalisation. No specific diseases in female boxers could be observed, in particular regarding the breast and reproductive system.
Statistics from Altmetric.com
Introduction
In Italy, participation in competitive sports is regulated by laws with the aim of safeguarding athletes' health.1 2 In 2001, a new law allowed Italian women to compete in boxing (both at amateur and professional level), even though in an experimental way, with the Italian Boxing Federation (Federazione Pugilistica Italiana, FPI), collecting data about the safety or the risks linked to this sport.3 This particular situation consented the publication of a short report in 2005 stating the overall low health risk in female boxers4 and the need to continue collecting data regarding competitions taking place over a 7-year period (2001–2007) in Italy as well as in international competitions abroad involving Italian athletes. The objective of this new study was to expand the observations of our previous report with a further 4-year period of analysis. The final collected data included the previous data of years 2002 and 2003.
Materials and methods
We monitored all female boxing competitions taking place in Italy from 4 April 2001 (official day in which the Italian law started regulating women boxing)3 to 31 December 2007. All athletes were informed on the aims of this research (or their guardians if under-aged), and they gave all their free consent to take part of the study. This study has been carried out in accordance with the Declaration of Helsinki and has been approved by the ethics committee of the involved institutions.
Our research was designed in two separate parts:
A retrospective study of all the data regarding female competitions (amateur and professional) in Italy from 1 January 2002 to 31 December 2007.
A prospective study started in 1 January 2002 to 31 December 2007 on amateur athletes affiliated in Lazio Region, which was chosen as it is the most active regional boxing committee in Italy. In this section, we considered mainly injuries involving breasts, reproductive and nervous systems, the eye, ear, nose and throat.
In compliance with the Italian laws,3 5 young women who applied for affiliation to FPI as competitive boxers had to pass, besides all mandatory tests for male athletes,1 2 the following medical exams:
Before affiliation:
▶ gender confirmation upon starting competitive activity;
▶ annual breast examination and mammary ultrasound;
▶ annual pelvic ultrasound;
▶ mammary x-ray precompetitive activity (only for professional athletes) and post-examination only after clinical indication. Likewise, it was also requested in amateur boxers after clinical suspicion.
Before competition:
▶ medical examination aimed in checking the breast/abdomen and pelvis areas; athletes were also required to provide a negative pregnancy laboratory report (performed <14 days earlier) and a self-signed statement, as requested by the Italian law (5) declaring that they did not suffer from vaginal bleedings (other then normal menses), pelvic tumourous masses, genital or urinary symptoms or recent surgery or traumas.
After competition:
▶ medical examination (carried out by ring-side physician immediately after the match) was aimed in checking the breast, abdomen and pelvis areas.
Results
Technical information
Amateur female boxers, during the period of study, competed in three rounds of 2 min each, with 1 min of rest between two following rounds. Since 2009, following the new rules issued by the International Federation of Amateur Boxing (Association Internationale de Boxe Amateure, AIBA), female Olympic-style boxers compete in bouts of four rounds of 2 min each, with 1 min of rest between two following rounds.
On the other hand, professional female boxers still compete from 4 up to 10 rounds of 2 min each, with 1 min of rest between two following rounds. All boxers wear 10 oz (284 g) gloves and a mouth-guard during matches. Abiding Italian laws, both amateur and professional boxers are to wear breast and genitalia protectors while a head guard is mandatory for amateurs (as requested by AIBA). Head guard, however, was mandatory also for professional female boxers in Italy, from 2001 to August 2005, as requested by Italian laws.3
All abbreviations used to indicate a boxing verdict when matches are stopped before the time limit, are shown in table 1.
Possible verdicts when matches are stopped before the time limit
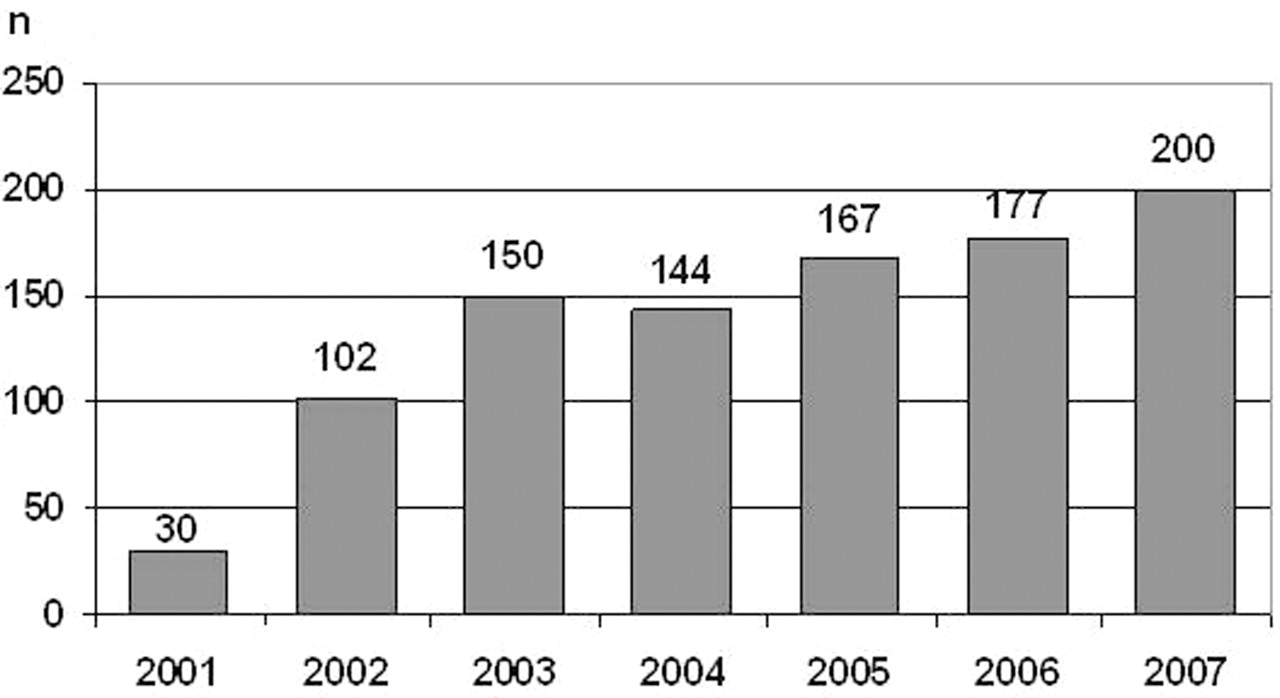
The data collected over the initial 7 years activity showed on increasing number of women turning to boxing. The number of female boxers is constantly increasing, from 30 to 200 in years 2001–2007 (fig. 1). Moreover, competitive results of Italian female boxers are promising, even at international levels, both amateur (one European and World confirmed Champion, and several top-ranking athletes in European championships) and professional (four European and two World champions). In table 2 are summarised trends of amateur and professional women boxers affiliated to FPI from 2001 to 2007, number of competitions and number (and decisions) of matches stopped before time limits.
Female boxers in Italy from 2001 to 2007.
Number of amateur and professional female boxers who competed in Italy from 2001 to 2007 and number (and decisions) of matches stopped before time limits in the same period
Boxing female activity in Italy from 2002 to 2007: retrospective study
As a whole, in the time span from 1 January 2002 to 31 December 2007, we collected data on 5600 medical examinations carried out in official competitions (2800 before and 2800 after competition). All prematch declarations were normal, as well as all pregnancy laboratory tests. In short, there was no declared recent or ongoing vaginal bleeding (other than normal menses), known pelvic tumourous masses, genital urinary symptoms or recent surgery and/or trauma.
Upon precompetition examination, only three amateur athletes (0.11%) complained of minor conditions: mild hyperemia of the right eye, one bruising in the zygomatic region in the second and an evident haematoma in the ocular soft tissue of the left eye in the last case, who was not allowed to take part in the competition.
After competition, medical examination was negative in 2749 cases (98.2%): in 51 exams in actions (1.8%, fig. 2), the following clinical conditions were highlighted:
▶ Twenty-two cases (21 amateur and 1 professional) for mild soft tissue contusion in the face (minor haematoma or ecchymosis in the zygoma, peri-ocular soft tissue and eyelid arm and shoulder).
▶ Twelve cases (11 amateur and 1 professional) suffered epistaxis, one with right inferior eyelid ecchymosis, one with left inferior eyelid ecchymosis, one for nasal bones fractures.
▶ In 11 cases (all amateur), mild contusion to the upper limb (hand, wrist and/or shoulder) was observed.
▶ Two amateur boxers had minor facial bruises not requiring surgery.
▶ Two professional athletes had periorbital lacerations that required suturing.
▶ Mild contusions to the lower limb were observed in three amateur boxers.
▶ One amateur athlete, who lost by knock-out (KO) after having received a blow to the nose, suffered a fracture to the nasal pyramid, and she was sent to the hospital for further assessment.
▶ One amateur athlete, who lost by KO after having received a blow to the head, lost consciousness for a few seconds. Complying with the rules of FPI medical section, also applicable to male boxers, in the events of blows to the head resulting in suspect head concussion (or more severe neurological conditions), the athlete was sent to hospital: however, she refused hospitalisation and denied further clinical examination and MRI of the brain when contacted 1 month later.

Medical problems after 2800 competitions disputed by female boxers.
No haematoma, ecchymosis or cysts were found in mammary region, and athletes did not report abdominal or pelvic acute conditions after competitions.
Boxing female activity in Italy from 2002 to 2007: Prospective study within Lazio Region
From 1 January 2002 to 31 December 2007, 61 amateur athletes (mean age 24.14±4.13 years) were affiliated as “female boxers” with FPI in the Italian Region Lazio and, therefore, subject to medical tests as specified by Italian laws.1 5 One particular athlete applying for affiliation was excluded from our study because she underwent aesthetic breast surgery in 2001, with positioning of prosthesis. Complying with the 2001 Italian law,3 in force at that time and confirmed by the new law in 2005,5 she was declared not eligible for competitive boxing.
During 84 months (mean follow-up 31.3±17.2 months), 40 athletes out of 61 (65.6%) took part in official competitions (ranging from 1 to a maximum of 35 bouts), for a total amount of 296 competitions (4.4±4.5 matches per boxer), which were stopped before the time limit in 18 cases (6.1%, 13 referee stop contest outclassed (RSCO), 4 referee stop contest head (RSCH) and 1 KO). No athlete was presented more than once in RSCH and/or KO verdicts.
Out of 61 athletes examined during follow-up, 32 underwent more than one medical examination either for yearly re-affiliation (28 cases) or for re-admission after loosing a competition before the time limit (referee stop contest (RSC), RSCH, abandon).1
One athlete, who lost by KO and had a fracture of nasal pyramid (see previous chapter), did not show up for the medical examination for re-admission and had decided to give up competitive boxing.
Mammary area
During the first visit, after clinical examination, diagnostic ultrasound and radiogram (when obtained), signs of fibrocystic mastopathy were showed in 9 out of 61 athletes (14.7%), even though these conditions are not to be considered harmful to boxing activities, according to the breast specialists consulted by FPI. Out of the nine athletes with positive findings, follow-up was possible only in three cases showing no changes either in radiological and clinical appearance.
Out of the 32 athletes who underwent more then one medical examination over the 84 months of our study, two cases, during yearly re-affiliation tests, were found by ultrasound to have developed a small fibroadenoma. Both athletes were declared eligible to boxing, according to the breast specialist consultants of FPI, although with a mandatory check-up every 6 months which showed no considerable change in size over the time (follow-up of 30 and 62 months, respectively).
One athlete, at echography for yearly re-affiliation, showed three small cystic lesions in the upper sectors of the left breast. When checked again in the following 3 months with subsequent echo scans, given the changes in size of such lesions along the menses and after consulting the breast specialist and endocrinologist, she was granted eligibility for 6 months (see following paragraph).
Reproductive system
At their first visit, all athletes reported regular menses as rhythm, quantity and duration, and they had menarche at the age of 12.4±1.0 years. Two athletes (3.3%) reported to be on oral contraceptive, and none of them had ever carried out any pregnancy.
Examination of reproductive system was negative in all cases, but echography revealed an ovarian cyst in two athletes (3.3%): in both cases, FPI consultants, once performed additional tests, decided this condition did not contraindicate boxing activity.
Among the 32 athletes who underwent more than one medical examination during the period of our study, a pelvic ultrasound only confirmed one ovarian cyst, unchanged in size, in one of the two athletes who showed such finding in their first examination. Although in the second athlete, the size of the cyst did not change (maximum diameter 22 mm) but oligo-amenorrhea occurred, she was sent for surgery after consulting her gynaecologist, because pharmacological treatment was not effective. Six months after surgery, she started training again and took part to five competitions (two wins, three losses by the score), without any problems related to the reproductive system (follow-up 40 months).
One athlete, with unremarkable gynaecologic findings at the first examination and ultrasound, was discovered to have a small left ovarian cyst in subsequent echography to the purpose of yearly re-affiliation. As this cyst changed size along the menses, as it happens in functional cysts, a yearly eligibility was granted. She did not report any troubles related to the reproductive system in a follow-up of 48 months; in the meanwhile, she took part to 25 competitions (13 wins, 1 draw, 11 losses by the score).
At the re-affiliation examination, one athlete who fought in two competitions over 12 months (one win, one loss, both by the score) reported polymenorrhea. Pelvic ultrasound showed an intramural myoma (maximum diameter 14 mm) which was not found in her previous examination. Such condition did not contraindicate competitive boxing, according to the specialists, although she was asked to have pelvic ultrasound check every 6 months. This athlete, however, decided to discontinue competitive boxing, and no more data are available about her condition.
Lately, at yearly re-affiliation, one athlete showed ovarian polycystosis by ultrasound, which was not found 12 months earlier: she is the same athlete also showing small mammary cysts, suffering, moreover, from hypothyroidism on pharmacological treatment. After consulting the specialists in endocrinology and gynaecology, she was granted eligibility, although on a 6-month basis, to better evaluate her clinical and laboratory history. At this time, we do not have any further follow-up information data for this athlete.
Nervous system
At their first visit, neurological examination was normal in all 61 athletes, while the EEG showed “non-specific anomalies” in four cases (6.6%).
In one athlete, we decided to postpone eligibility and take a second EEG after 6 months, which confirmed the same anomalies. We asked the athlete to take MRI of the brain that showed normal results, and she was re-admitted to competitive boxing. Subsequent EEGs and examinations for yearly re-affiliation did not show any worsening of EEG anomalies, although she had intense competitive activity (27 matches over 4 years, 14 wins, 1 draw, 3 losses by RSCO, 1 WO and 8 losses by score).
MRI was also obtained in the three further cases showing EEG “non-specific anomalies” in their first exam. Two of them did not show any anomalies of note to cranial-encephalic and cerebellar areas and eligibility was, therefore, granted (by now, we do not have any further follow-up information). The third one is still suspended from competitions as she is waiting to take her MRI.
One athlete (included in our previous study) was found to have non-specific EEG anomalies upon her re-admission after losing a competition by RSCH: she also showed, as neurological finding, first degree nystagmus when looking leftwards and right-side deviation in the straight marching test. We requested MRI, which was normal. Because her neurological findings and EEG anomalies subsided, she was granted eligibility to competitive boxing. Since then, she has taken part to additional 18 competitions, 4 wins, 2 draws, 12 losses (1 by RSCO, 11 by the score), and neither EEG anomalies nor neurological signs were found at her subsequent three yearly re-affiliation examinations.
The three athletes who lost before the time limit (one RSC, two RSCH) did not show any adverse neurological signs. The athlete who lost by KO and reported nasal bones fracture did not apply for re-affiliation; therefore, she did not undertake any further examination.
The eye
At their first examination, 16 athletes out of 61 (26.2%) had myopia, which was moderate in six of them (overall visual acuity of 8/10, with at least 4/10 at each eye): they were all granted eligibility but were compelled to wear soft contact lenses during training and competition. One athlete out of the 16 myopic athletes was disqualified from competitive boxing for a high-degree myopia (non-corrected visus in left and right eye of 1/50), as provided by the medical rules of FPI.
Fundus oculi showed a mild dystrophia of lower peripheral retina in one athlete with high-degree myopia (non-corrected visus in the left and right eye of 1/10), although it was judged non-significant to practice boxing. Another athlete with high-degree myopia (1/10 not corrected visus in both eyes) showed signs of successful therapeutic laser for peripheral retinal degeneration and microlesions. This case was also judged to be eligible to competitive boxing. Last, a mild inferior retinal dystrophy was found in a young woman with normal visus, although not contraindicating competitive boxing, along with ophthalmologists' opinion.
A paving stone degeneration in the upper retina was demonstrated at first examination in one athlete with moderate myopia (non-corrected visus in the right and left eye 1/10). After consulting the eye specialist, we decided to grant eligibility only for 6 months to follow properly such condition. We do not have further data regarding this athlete, as she still has to take her control examination.
In the study period, two athletes out of six with moderate myopia had surgical treatment (photorefractive keratotomy) with a good outcome, and they reached, respectively, not corrected visus of 10/10 in the right eye and 9/10 in the left eye in one athlete, and 9/10 in both eyes in the other athlete.
Fundus oculi confirmed mild dystrophia of the lower retina in the athlete who showed such findings in her first examination. This young woman came back for yearly re-affiliation, and she took part to six competitions during the year (four wins, two losses by the score). In the second athlete with dystrophic retina and normal visus, the latest fundus oculi examination was normal.
Along a follow-up of 13 months, one athlete who took part to three matches (one win, two losses by the score) at fundus oculi examination showed a vitreoretinal adhesion in the right eye, although our consulting ophthalmologists did not consider it an excluding criterion for competitive boxing.
In one more athlete (follow-up 54 months, 21 competitions, 14 wins, 5 losses by the score, 2 losses by RSCO), fundus oculi examination demonstrated a new area of hyperpigmentation in the middle peripheral retina of the right eye, also judged of no importance by consultants.
Peri-ocular soft tissue, lenticular apparatus and eye tonometry were normal in all athletes both at first examination and at their last visit.
Ear, nose and throat
At their first examination, one athlete showed a mild bilateral tympanic retraction and a mild bilateral transmissive hypoacusia at high frequencies. The finding of mild bilateral high-frequency hypoacusia was also demonstrated in one more athlete (2 out of 61, 3.3%). In both cases, such anomalies did not contraindicate competitive boxing, although only the first of the two athletes (follow-up 25 months) took part to official competitions, fighting only one match (lost by the score). Subsequent otoscopy and audiometry were unchanged in this athlete at yearly re-affiliation examination.
Among the 61 athletes examined, four (6.6%) showed signs of fracture of nasal pyramid at their first examination, while nasal septum was found to be mildly deviated in 26 of them (42.6%). Four cases (6.6%) had signs and symptoms of rhinitis probably on allergic basis (pollinosis) also found in other four athletes at yearly re-affiliation examination. Mild hypertrophy of lower turbinates was found in 22 athletes (36.1%) at first examination and in 17 during follow-up, two of them with previous normal findings.
At re-admission examination, one athlete with nasal pyramid previously normal and not deviated nasal septum was found to have signs of past fracture of nasal bones and mild septum deviation, which she suffered in a match lost by RSCH. Nasal septum deviation was newly found also in one athlete at yearly re-affiliation examination (18 competitions during 24 months of follow-up, 4 wins, 2 draws and 12 losses by the score).
Discussion
Boxing is a millenary sport, traditionally limited to men. Since 1995, starting with the first official women competitions in Germany, a new trend is now leading to an increasing participation of women to competitive boxing. Year after year, a number of events were held, such as Continental and World Championships, and the AIBA is now aiming to the acknowledgment of female boxing as Olympic sport. Since April 2001, following an Italian law (later modified in 2005), female boxing is now permitted in Italy, although still under experimental basis.3 5 Data gathered along the first years of practice have confirmed an increased attention towards this sport, as shown by the steady increase in the number of athletes affiliated to the Federation and the important results obtained during competitions.
Data regarding all female boxing competitions held in Italy during the first 6 years show that health problems caused by boxing competitions are 0.30% per year, less frequent than in male boxing6 7 and lower than what was stated in our previous study on women's boxing.4 As shown by fig. 3, which compares data in the first 2 years of the study (2002–2003) to those in the four following years (2004–2007), there is an important decrease in average prevalence (from 2.86% to 1.50%) and incidence (from 1.56% to 0.37% per year) in the conditions observed at medical examination after competition, while overall mean prevalence and incidence were, respectively, 1.82% and 0.30% in the 6-year period of study.

{kind=link}
{kind=link}
{kind=link}
Prevalence and incidence of medical problems occurred in female boxers competing in Italy from 1 January 2002 to 31 December 2007. In respect to a previous report of our group on a lower number of athletes and for a shorter period,4 global prevalence and incidence clearly decreased.
Such apparent reduction in health conditions related to official competitions can be explained by a larger sample size, but it also follows the increase in technical skills of the athletes participating to competitions and, probably, a greater experience of the referees monitoring the safety of women boxers. Moreover, we did not find any severe lesions, and we have no reports of conditions regarding the genitourinary system or the breast clearly related to boxing. The most frequent lesions were mild haematoma/ecchymosis in the face, and epistaxis, with four cases of bruise in the eyebrow region, requesting surgical closure in two professional athletes. Both bruises occurred after the new law regulating female boxing in Italy that allowed removing the obligation of wearing a head guard5 for professional athletes.
Since April 2001, when female boxing was initially permitted in Italy, hospitalisation was necessary only in two athletes (prevalence 0.07%, incidence 0.012% per year), who lost by KO due to a blow to the head, in one case with a momentary loss of consciousness. In both cases, unfortunately, no further information is available following hospital discharge, because both athletes decided to abandon competitive boxing and did not re-affiliate. However, we can speculate that they did not have any significant lesions, as they did not bring on any insurance applications.
The prospective study in Lazio Region over 6 years (1 January 2002 to 31 December 2007) seems to rule out the presence of lesions to the genitourinary tract and the breast clearly related to boxing. In fact, only 3 (4.9%) among 61 athletes had an ovarian cyst, requiring surgery in one case. Although the study sample is limited, such finding is consistent with data in literature, showing a prevalence of benign ovarian cysts of 4.8–6.6% in women of age 25–40.8 9 Moreover, it is not clear the relation between presence or appearance of ovarian cysts and trauma to the pelvic region, just as there are no data available in scientific literature regarding abdominal and pelvic trauma and occurrence of intramural myoma. For this reason, the finding of one case of myoma seems to appear accidental. However, it should be considered that when large masses are found in the womb or annexes, it is advisable to forbid boxing, as well as all other sports with risk of abdominal trauma.
Regarding the breast, two athletes (3.3%) had fibroadenoma, the most frequent benign lesion of the breast, with a prevalence ranging from 7%10 to 25% in asymptomatic women11 and peak incidence in the third decade.12 13 After all, there are no reports in scientific literature regarding the relation between fibroadenoma and trauma to the breast. During our study, lastly, we did not observe any haematoma or inflammatory disease of the mammary tissue in the examined athletes.
As for neurologic, eye and ear–nose and throat issues, apparently, there were no differences between men and women in the risk of lesions related to boxing. Nevertheless, with the aim to better describe the traumatological risk of women's boxing, we carried out a close analysis regarding these systems. In our study, four athletes (6.6%) showed non-specific EEG anomalies at their first visit, therefore, requiring a brain MRI. Except for one athlete, who is waiting to take her MRI, in three cases, no anomalies were found, and athletes were regularly admitted to competitive boxing. Only in one of the four athletes do we have an adequate follow-up (about 4 years) showing how, notwithstanding her full competitive career (27 matches, 14 wins, 1 draw, 3 losses by RSCO, 1 by WO and the remaining 8 losses by the score), there were no significant changes in her EEG.
After a match lost by RSCH, another athlete showed first-degree nystagmus and rightwards deviation in the marching test, associated with the recently onset of non-specific EEG anomalies. For this reason, the young woman had a brain MRI, which did not demonstrate any focal or diffused lesions, and for this, also supported by the receding of the neurological findings and EEG normalisation, she was allowed to return to boxing after the period of rest prescribed by Italian laws and FPI medical rules. Since then (2003), this athlete took part in 18 competitions, with 4 wins, 2 draws and 12 losses, showing no neurological signs or complains and no EEG anomalies in the three subsequent visits for yearly re-affiliation.
Concerning the eye, the prevalence of myopia in amateur female boxers in Lazio Region (26.2%) is similar to what described in scientific literature in the general population,14,–,16 and one athlete was not allowed competitive boxing, due to high-degree myopia. Two myopic athletes (3.3%) showed mild peripheral retina dystrophy, a condition frequently associated with myopia.17 This specific condition, also found in one athlete with normal visus, according to the consulting specialists, does not predispose to traumatic detachment of the retina, such as the results of retinal laser therapy18,–,21 performed in one case with degeneration and microholes, possibly related to severe myopia.17 22
One athlete with myopia, lastly, was given a 6-month eligibility, with the aim of keeping a closer follow-up on a small area of paving stone degeneration in the upper retinal sector. No further data are available, unfortunately, as the athlete did not show up again for examination.
In one athlete fighting three times along 13 months of follow-up (one win, two losses by the score) examination of the eye showed a peripheral vitreoretinal adhesion in her right eye, which our consulting specialists did not consider significant to eligibility to boxing. In another athlete (follow-up 54 months, 21 matches, 14 wins, 5 losses by the score and 2 losses by RSCO), her recent eye examination showed a middle-peripheral area of hyperpigmentation in her right eye, also considered non-significant by consulting specialists.
Regarding ear–nose and throat, the prevalence of binaural mild high-frequency hypoacusia observed in our athletes (3.3%) resembles what is described in scientific literature in the general population23 24 and, similarly related to the incidence of post-competition health issues in fig. 3, lower than what we had observed (7.1%) in the first 2 years of medical surveillance on female boxing.4 However, it should be considered that trauma to the ear can cause a tympanic perforation which, when underestimated, can lead to the development of transmissive hypoacusia of higher severity than it was previously found.
Regarding trauma of the nose, fracture of the nasal bones is the most frequent lesion in boxing,25 26 as it is commonly observed in different sports involving contact or impact.27,–,29 The outcome of previous fractures was observed in four athletes at their first examination (6.6%) and in one athlete at re-affiliation visit. Nasal septum deviation was found in 26 athletes (42.6%) at their first examination, resembling the prevalence found in age-matched general population (about 40%),30 31 anyway lower than what we had found in the first 2 years of medical surveillance on female boxing.4 Such reduction in prevalence (from 67.9% to 42.6%), similar to what observed in the rate of post-competition health issues in fig. 3, can be explained moreover by the larger sample size examined (from 28 athletes in the previous report in 2005, to the present 61 athletes). The prevalence of hypertrophic lower turbinates, found in 22 athletes out of 61 at first examination (36.1%), is a condition widely found in the general population, frequently associated with nasal septum deviation in 14 out of 22 athletes (63.6%).32 33
Conclusions
Seven years have passed since female competitive boxing firstly appeared in Italy as an official sport, and acute events are very rare.
Presently, no mammary or gynaecologic diseases to be specifically correlated to boxing practice (both at amateur and professional level) have occurred, and health pathological conditions regarding the nervous system, eye and ear, nose and throat are quite similar in prevalence and incidence to what observed in general non-athletic young population and/or in male boxers. Moreover, the rate of medical problems in the after-match examination and in the longitudinal phase of our study has appeared lower than what we reported in a previous research with fewer athletes evaluated and with a shorter follow-up.
For these reasons, we believe that female boxing, as well as male boxing, is nowadays granted satisfactory medical assistance in Italy, due to a great extent to the close attention by the Italian Ministry of Health and by a steadfast control by the Italian Boxing Federation.
Finally, this analysis strongly confirms what we observed in our previous report that female boxing brings about the same health risks to the women athlete, as any other sport in which opposite players share the field and may possibly come to an impact (either willingly or accidentally). Moreover, we hope that this close and reassuring analysis of health conditions of female boxers could contribute to a quiet and conscious inclusion of women's boxing among other contact sports and martial arts that are well accepted by public opinion and the medical personnel all over the world.
What is already known on this topic
Women's boxing is a recent sport with a prevalence and incidence of injuries, respectively, of 2.86% and 1.56% per year, similar to what observed in male boxing and in other contact sports.
What this study adds
This new study shows that women's boxing is safer than previous observed, with an overall prevalence and incidence of injuries, respectively, of 1.82% and 0.30% per year. No lesions, particularly to the breast and reproductive system, seem to be related to boxing.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Italian Boxing Federation.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Corrections