Article Text

Abstract
Objective To examine whether people with recurrent ankle sprain, have specific physical and sensorimotor deficits.
Design A systematic review of journal articles in English using electronic databases to September 2009. Included articles compared physical or sensorimotor measures in people with recurrent (≥2) ankle sprains and uninjured controls.
Main outcome groups Outcome measures were grouped into: physical characteristics, strength, postural stability, proprioception, response to perturbation, biomechanics and functional tests. A meta-analysis was undertaken where comparable results within an outcome group were inconsistent.
Results Fifty-five articles met the inclusion criteria. Compared with healthy controls, people with recurrent sprains demonstrated radiographic changes in the talus, changes in foot position during gait and prolonged time to stabilisation after a jump. There were no differences in ankle range of motion or functional test performance. Pooled results showed greater postural sway when standing with eyes closed (SMD=0.9, 95% CI 0.4 to 1.4) or on unstable surfaces (0.5, 0.1 to 1.0) and decreased concentric inversion strength (1.1, 0.2 to 2.1) but no difference in evertor strength, inversion joint position sense or peroneal latency in response to a perturbation.
Conclusion There are specific impairments in people with recurrent ankle sprain but not necessarily in areas commonly investigated.
Statistics from Altmetric.com
Introduction
Chronic ankle instability (CAI) is a problem for many people with a history of acute ankle sprain, with reports indicating that up to 34% of people incur a residual problem within 3 years following their first ankle-sprain incident.1 Characteristics of CAI include recurrent sprain, mechanical instability, ‘giving way’ of the ankle, functional instability, pain and swelling.2 Mechanical instability is defined as joint range of motion that is beyond the normal expected physiological or accessory range of motion. Around the ankle, this is usually considered excessive inversion laxity of the rear foot or excessive anterior laxity of the talocrural joint. Functional instability is defined as frequent episodes of ‘giving way’ of the ankle joint and/or feelings of ankle joint instability.2 The cause of CAI is unknown, but it is thought that sensorimotor deficits resulting from the original ankle injury may play a role.3
Sensorimotor variables that have been studied in participants with CAI include proprioception, strength, and neuromuscular and postural control. Results from these studies are equivocal.4,–,11 Recent systematic reviews have further examined postural stability,12,–,15 proprioception, muscle reaction times14 and strength.16 Three reviews of postural stability, with meta-analyses, concluded that there are deficits in postural stability in unstable ankles compared with ankles without instability.12 14 15 A contrasting finding was reported in another review which concluded that using force-plate measures in single-leg stance on a stable surface did not discriminate between participants with CAI and those without.13 A deficit in frontal plane joint position sense may be present in participants with functional ankle instability, but not in measures of peroneal reaction time.14 A recent meta-analysis of ankle evertor strength found a decrease in strength in participants with ankle instability, but the authors stated that the difference may be too small to be clinically significant.16
These systematic reviews and other studies in the area4,–,11 encompassed a broad spectrum of inclusion criteria for participants with CAI and may explain conflicting results with similar tests. The reviews included participants with ‘giving way’, ankle instability, recurrent injury, functional instability (however defined) or any combination of these. This reflects a recent systematic investigation of definitions and inclusion criteria used in ankle research studies2 which demonstrated the wide variety of characteristics of participants in CAI research and recommended the tightening of inclusion criteria.17 Preliminary evidence18 19 suggests that using more homogenous groups of participants with CAI could demonstrate deficits more clearly, and that these deficits may differ among subgroups.20 A way forward would be to undertake a review based on a homogenous cohort of participants and determine if deficits in outcomes were more clearly defined. The aim of this review was to determine whether people with recurrent ankle sprain exhibited differences in physical findings, strength, postural stability, proprioception, response to a perturbation, biomechanics or functional tests compared with healthy controls.
Methods
We conducted a literature search using the AMED, CINAHL, PEDro, PubMed and SportDiscus databases, from inception to 30 September 2009. In Pubmed, the following participant-specific strategy was developed, and modified for use in the other databases: (1) ankle injuries or ankle joint or ligaments, (2) ankle.tw, (3) sprain or strain or rupture or instability or unstable or repeated or recurrent or multiple or functional or functionally or chronic or chronically, (4) 2 AND 3, (5) 1 AND 4. The search was limited to papers published in the English language.
Inclusion criteria
Articles were included if they satisfied the following criteria: all participants in the recurrent ankle sprain group had sustained two or more ankle sprains, all participants in the healthy control group were independent non-injured participants, and at least one outcome of interest was measured. The extracted data were grouped into: bone and joint characteristics, strength, postural stability, proprioception, response to perturbation, biomechanics and functional tests. Bone and joint characteristics included any measures of anatomical features and ankle joint mechanics, such as joint laxity and joint motion. Strength measures included strength in any plane around the ankle joint axis of motion. Postural stability included single or bilateral standing measures that did not involve moving the standing limb/s. Proprioception included any proprioceptive measure of ankle movement, whether active or passive. Response to a perturbation included any measurement that occurred during or after a perturbation of any degree. Biomechanics measures were usually laboratory-based, and involved active movements such as gait, jumping or cutting manoeuvres. Functional tests, in contrast, were tests of active movement used in clinical settings with minimal equipment. These included tests such as hopping or running around a set course.
Data extraction and analysis
Search result screening and data extraction were conducted by two independent reviewers. Where consensus was not reached, a third person adjudicated. The data extracted were participant sample size and characteristics, the tests used and results. For randomised controlled trials, only baseline data were extracted. Where groups of studies provided inconsistent findings, and if studies were considered homogeneous with regard to participant characteristics and outcomes, data were pooled using the random-effects model. The random-effects model was chosen to incorporate heterogeneity among studies.21 The effect size was calculated using the standardised difference of the mean (Hedges' adjusted g) when comparing studies with different outcome measures, and as the difference in group means for studies with the same measure. Where the outcome of interest was considered to be more desirable when larger, for example, strength, the outcomes were multiplied by −1 to convert all effect sizes to the same direction. All meta-analysis was undertaken using Review Manager Version 5.0 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2008.).
Results
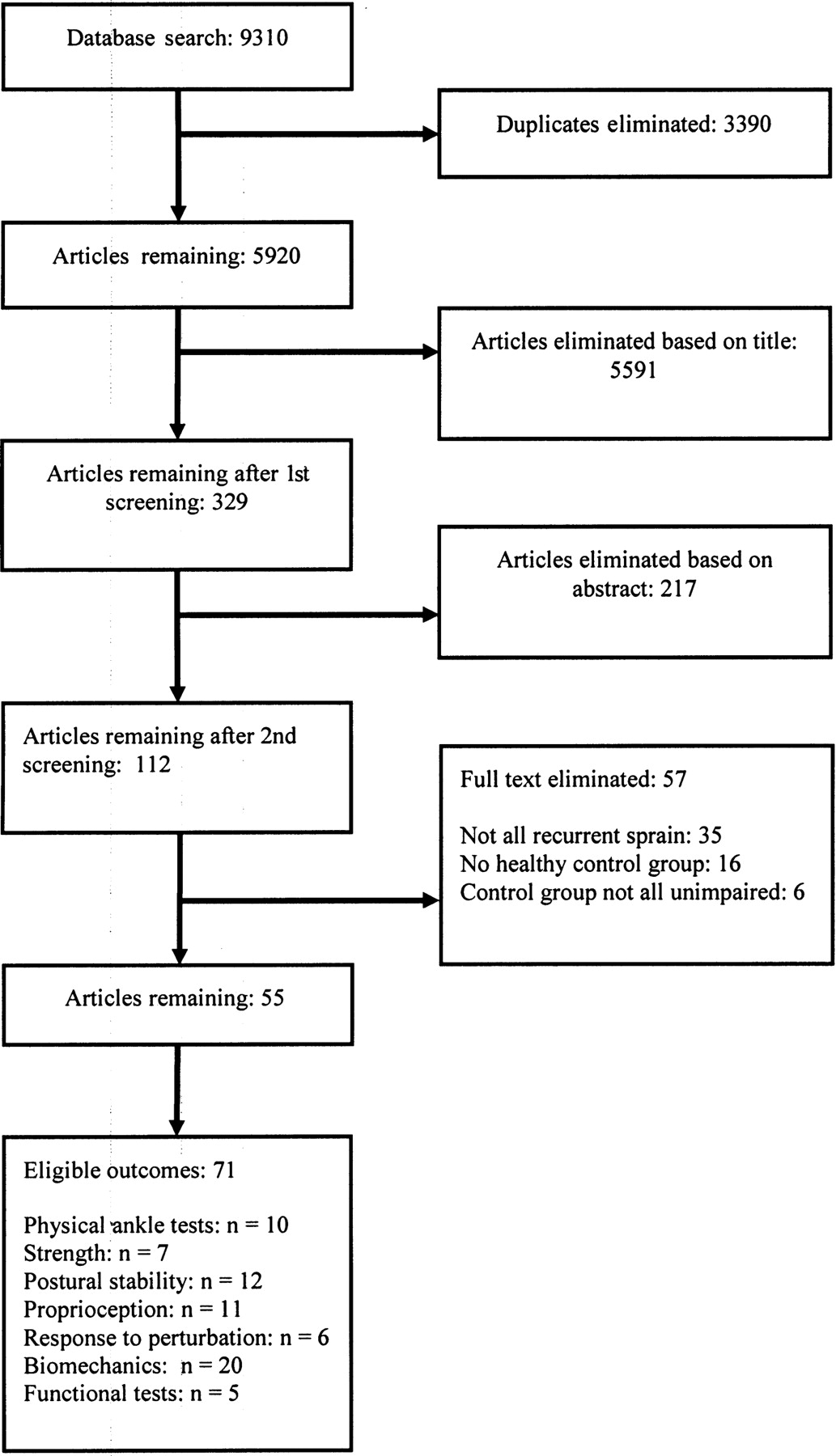
A total of 55 papers were retrieved for data extraction from an initial titles search of 9310 (figure 1). A range of physical and sensorimotor deficits were examined; the most common outcome group was biomechanics measures (20 studies, figure 1). The age range of participants in 52 of the papers was 18–30 years. The remaining three papers recruited participants with an average age in the thirties.22,–,24 Papers were skewed towards the male population with 26 studies including solely, or a majority of, male participants. Only one paper had a solely female cohort,25 and seven papers had a majority of female participants.24 26,–,31 The sample size of the included papers ranged from 1530 to 10422 23 with a mean of 42±21.2 (mean±SD) participants.
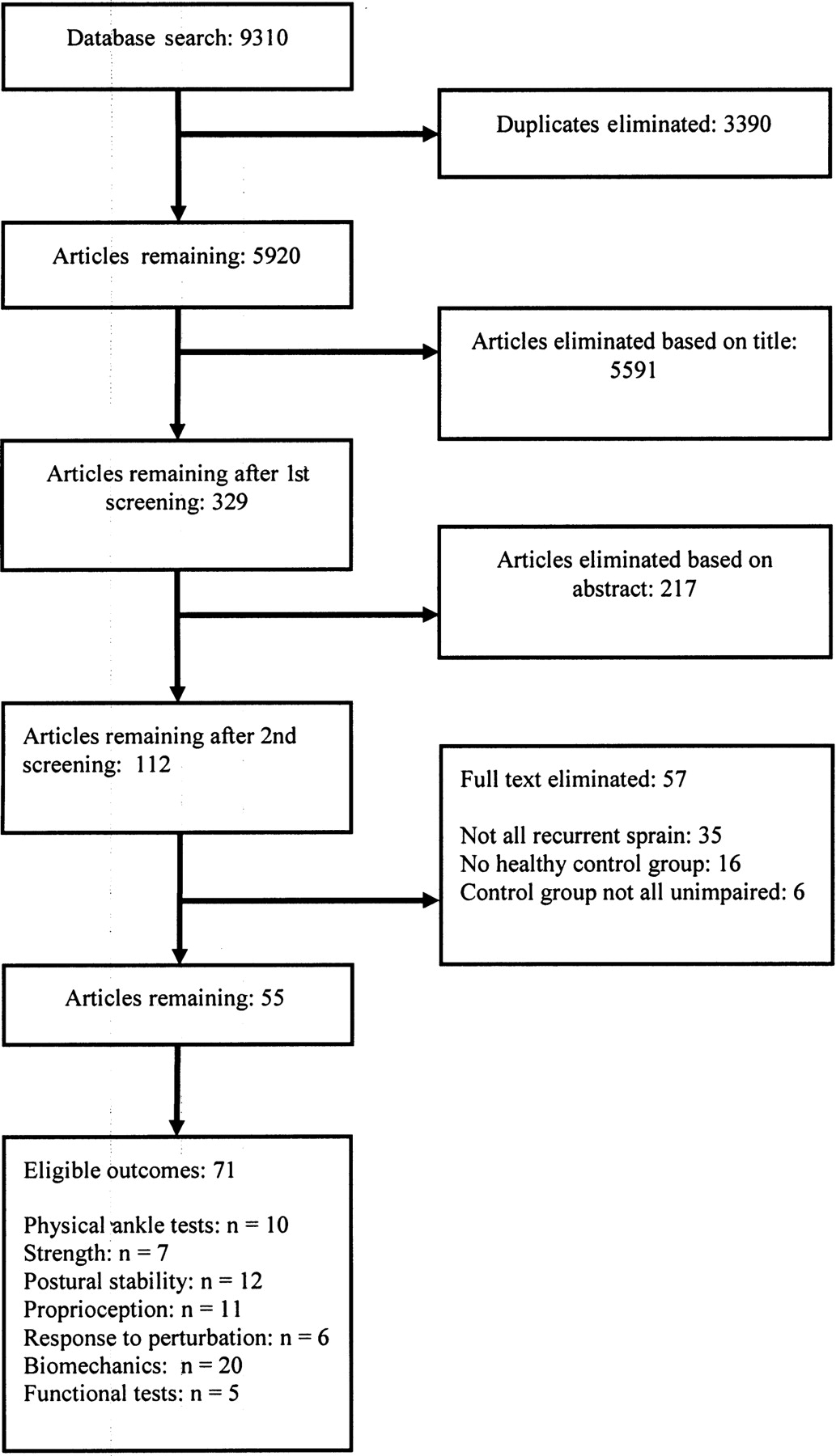
Flow chart for included papers.
Bone and joint characteristics
Papers considering the bone and joint characteristics of participants with recurrent ankle sprain (table 1) investigated a range of variables including ankle anatomical features, range of motion, and ankle joint laxity or stiffness. A broad spectrum of methodologies were utilised.
Bone and joint outcomes
Anatomical features were investigated using x-rays or fluoroscopy, with some measuring the position of the fibula relative to the tibia at the distal tibiofibular joint23 32 33 and others measuring the shape of the talus.22 23 The fibular position was found to be more anterior in two of three papers,23 32 33 and the two papers investigating the shape of the talus found the radius of the curve to be larger22 23 The small number of papers and the heterogeneity in the measurement methods used meant that it was not possible to conduct a meta-analysis.
Range of motion (active and passive) was investigated in five studies, with none finding a significant difference in any direction between participants with recurrent ankle sprain and a control group.26 34,–,37 Joint laxity and stiffness were measured in four studies. Laxity was measured using manual testing of talar tilt and anterior drawer37 and an instrumented anterior drawer test.33 Joint stiffness into inversion has been assessed using instrumented methods to obtain torque angle curves.24 38 Only the instrumented anterior drawer test found significantly more movement in the group of participants with recurrent ankle sprain.33
Strength
Strength of the ankle musculature in participants with recurrent ankle sprain was predominantly investigated for inversion and eversion movements (table 2). Outcome measures derived from isokinetic dynamometry included peak torque, peak torque normalised for body weight and ratios of inversion to eversion strength using isometric, concentric and eccentric contractions. Of the three papers using normalised torque values,37 39 40 only one found significant differences, and this was only in the eversion direction with faster speeds increasing the likelihood of differences.39 Other strength papers found either no significant differences36 37 40 41 or differences which could be linked to group weight differences.5 Pooling of the concentric and eccentric invertor and evertor peak torque data demonstrated a significant large effect for concentric inversion only (standardised mean difference (SMD)=1.1, 95% CI 0.2 to 2.1; figure 2). Overall, strength differences did not appear to be a strongly distinguishing feature of participants with recurrent ankle sprain.

Forest plot of the standard mean differences, effect size and 95% CI for inversion and eversion peak torque measures. C, total number of control participants; RS, total number of participants with recurrent sprain.
Strength outcomes
Postural stability
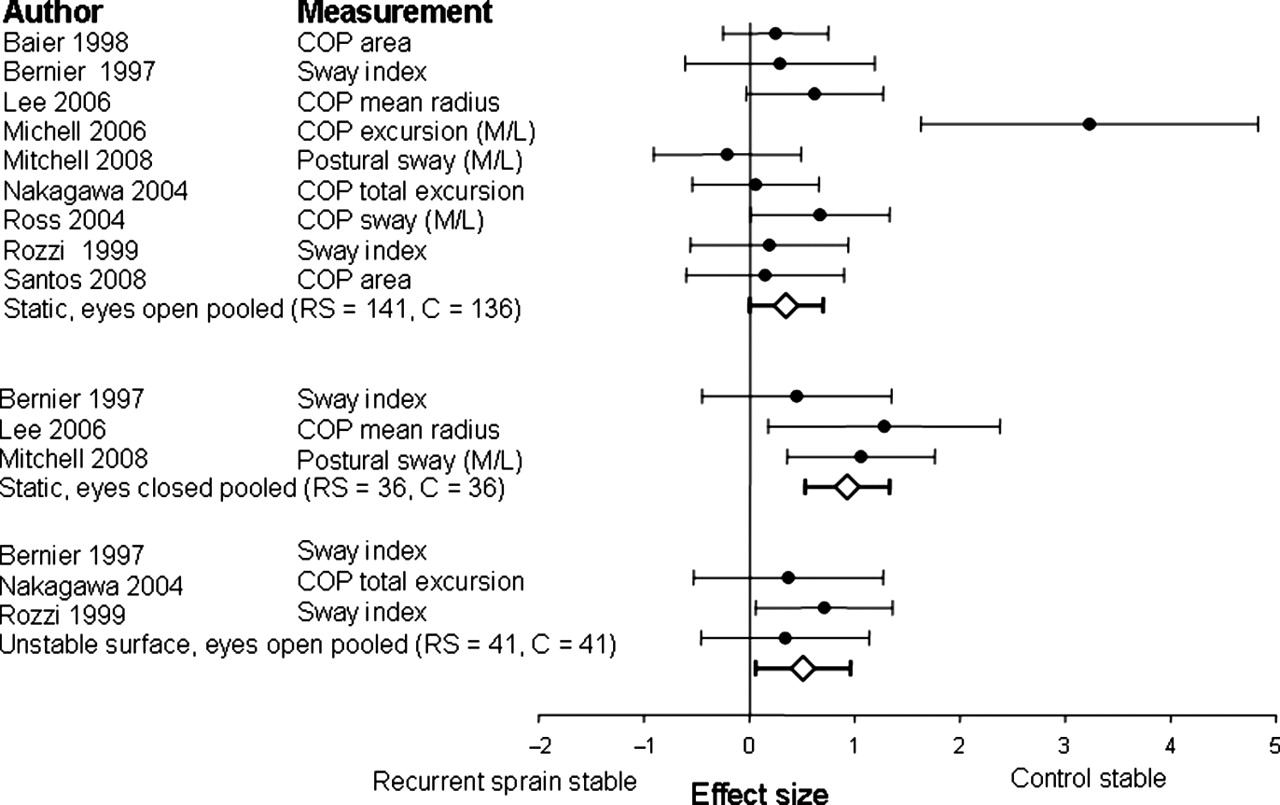
Investigations of postural stability used a variety of measures including centre of pressure velocity, centre of pressure excursion or sway index (table 3). Balance has predominantly been studied on static surfaces6 24 25 31 41,–,48 with some studies using unstable surfaces.25 31 41 43 48 Pooling of data was undertaken if outcomes were reported in units of distance or area, but not in time-to-boundary,45 strategy25 or angular measures (figure 3)43 With a stable surface and the eyes open, the pooled results showed there was no statistically significant difference between the groups (SMD=0.4, 95% CI 0.0 to 0.7). However, a large effect was demonstrated with tests on a stable surface with the eyes closed (SMD=0.9, 95% CI 0.4 to 1.4), and a moderate effect with tests on an unstable surface with the eyes open or closed (SMD=0.5, 95% CI 0.1 to 1.0) for increased postural sway in participants with recurrent sprains compared with controls.

Forest plot of the standard mean differences, effect size and 95% CI for single leg balance with the eyes open and closed on a stable surface, and an unstable surface. C, total number of control participants; CoP, centre of pressure; M/L, mediolateral; RS, total number of participants with recurrent sprain.
Postural stability outcomes
Proprioception
Investigations of proprioception most commonly studied inversion and eversion directions using active and passive joint position sense (table 4). These studies used different foot positions, speed and application of movement, yielding inconsistent findings. Four of six studies found deficits in participants with recurrent ankle sprain in active repositioning26 38 39 49 and two of five found deficits in passive repositioning.26 44 Pooling of data for active (SMD=1.2, 95% CI −0.3 to 2.6) and passive (SMD=0.2, 95% CI −0.3 to 0.8) inversion joint position sense and passive mixed inversion/eversion (SMD=0.7, 95% CI −0.2 to 1.6) joint position sense showed no difference between groups (figure 4). Studies which examined active mixed joint position sense were consistent in their findings, showing no difference between groups.4 44 There was only one study of passive inversion and eversion movement detection which found impaired movement detection in the recurrent ankle sprain group at all three velocities tested.50 Only three studies investigated the dorsiflexion–plantarflexion plane.34 43 51 There were conflicting results for passive joint position sense34 43 and no difference between groups for passive movement detection.51

Forest plot of the standard mean differences, effect size and 95% CI for joint position sense in inversion and mixed inversion and eversion. C, total number of control participants; RS, total number of participants with recurrent sprain.
Proprioception outcomes
Response to perturbation
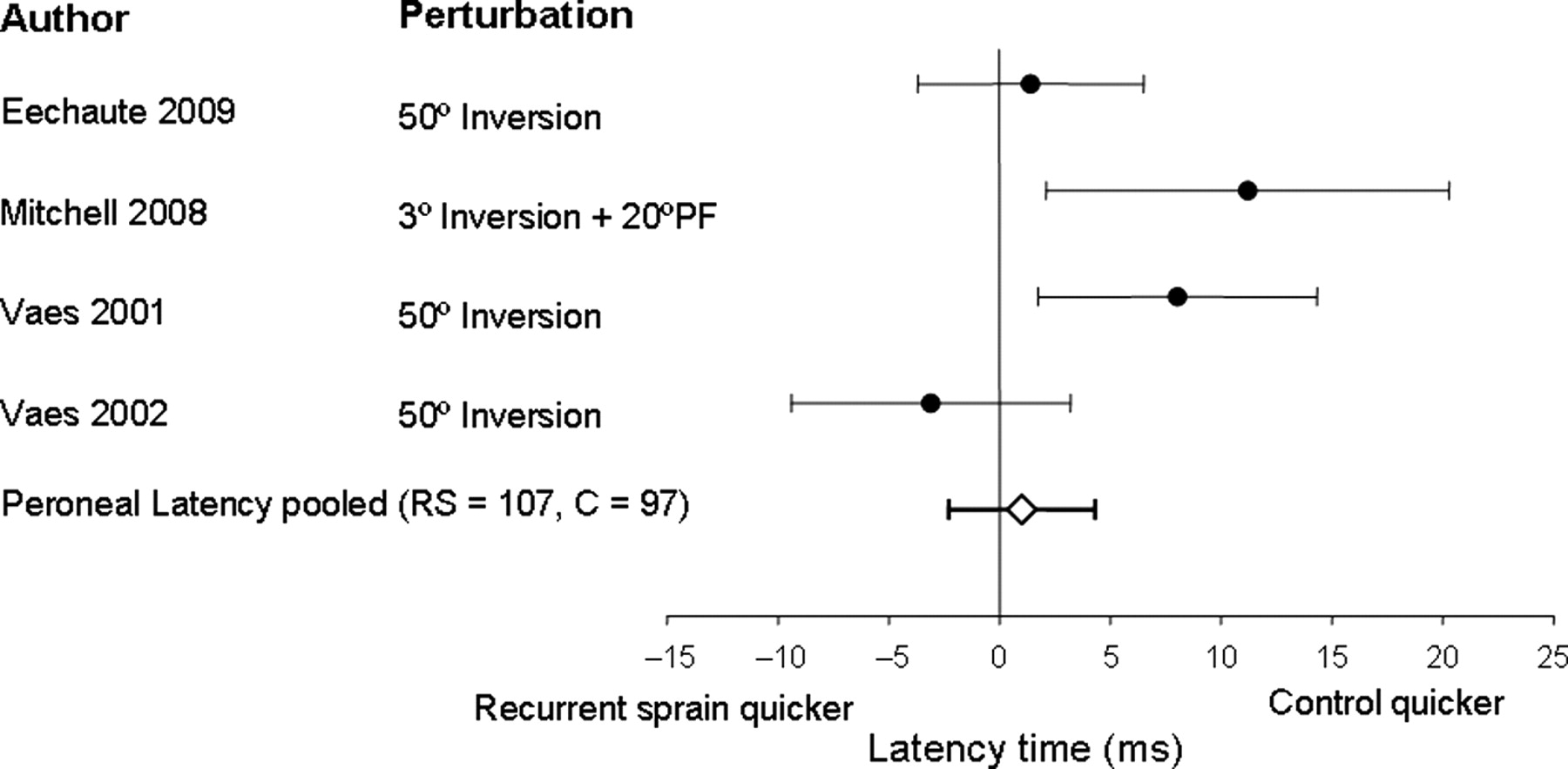
Investigations of response to perturbation (table 5) differ widely in methods used, including: dual and single leg stance, varying methods of applying perturbation with nociceptive28 52 and mechanical stimuli,29 30 53 54 and varying magnitude of perturbation. Three papers used the same positioning and degree of perturbation29 30 53 but, despite measuring similar outcomes, had no significant results in common. Overall, the most commonly investigated outcome was peroneal reaction time, but the pooled results showed that there was no difference between groups (mean difference=3.3 ms, 95% CI −2.3 to 8.9, figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of the standardised mean differences, effect size and 95% CI for peroneal latency following an inversion pertubation. C, total number of control participants; PF, plantarflexion; RS, total number of participants with recurrent sprain.
Perturbation outcomes
Biomechanics
The most common activities studied in terms of biomechanical variables were gait and landing from a jump (table 6). Gait studies investigated walking27 55,–,59 either on a treadmill or overground, and a variety of outcomes were measured. Participants with recurrent ankle sprain demonstrated a more inverted ankle position55 57 and decreased foot clearance. No significant differences between groups were noted for knee or hip variables, in either kinetic or kinematic analyses.55 57 Gait electromyography (EMG) results were contradictory in the two papers which evaluated gait on a treadmill,27 55 as were ground reaction force findings.56 58
Biomechanical outcomes
The jump landing studies all investigated tests in which participants jumped down from a height (jump down test) or performed a vertical jump from the floor, landing on one leg. Main outcomes studied were force plate measures, EMG and joint kinematics or kinetics. Findings from studies using force plate measures were inconsistent and depended on method of testing and variables measured.6 33 34 60,–,63 Studies using a time-to-stabilisation method all used the vertical jump, consistently finding that participants with recurrent ankle sprain took longer than controls to stabilise after landing in the anteroposterior direction and in combined directional measures.6 52 61 63 64 Inconsistent results were recorded for peak ground reaction force and timing, although it appears that an increased peak vertical ground reaction force and earlier timing of the peak force are present in participants with recurrent ankle sprain.60 65 These findings were consistent with the one study that investigated a V-cut movement.66 Muscle activity, measured pre- and postimpact, showed various conflicting differences between groups34 65 67 68 except for a decrease in peroneus longus activity preimpact in two studies investigating the jump down test,65 67 whereas these findings were not evident in a study of vertical jump.34 Investigation of joint kinetics and kinematics found that the ankle appears more inverted65 69 and the hip less externally rotated prior to landing65 in participants with recurrent sprains than in controls. Changes in knee joint angular displacement after landing are conflicting.65 69
Individual studies investigated a variety of other tests, including dropping from a height,68 various movements onto or off a force plate,66 67 70 wobble board movement71 and unloading reactions28 with no consistent results.
Functional tests
Few functional tests have been investigated. Those that have been investigated include jump height, running and hopping (table 7). There was no difference between groups for vertical jump6 63 and running tests.72 73 Three studies investigated hopping utilising different methodology.6 63 72,–,74 Only one study found a significant deficit in the time taken by the recurrent ankle sprain group to complete the test.74
Functional tests
Discussion
This systematic review extracted data from 55 studies that compared outcomes between people with recurrent ankle sprains and healthy controls. Our selection of a more homogenous participant group than that used in prior reviews, which used broad umbrella definitions of CAI, enabled identification of areas that were consistently impaired and those that were not. Compared with healthy controls, participants with recurrent ankle sprains had a larger talar curve, reduced concentric inversion strength, greater sway when standing on stable surfaces with eyes closed, a more inverted ankle position and decreased foot clearance during gait, and prolonged time to stabilisation after a jump. There is little evidence supporting some of the deficits commonly believed to be associated with CAI such as increased peroneal latency, decreased evertor strength and impaired proprioception.
One area in which this review has provided improved clarity was postural stability. Recent systematic reviews12 14 15 concluded that static measures of postural stability were significantly different between CAI and healthy controls when tests were not categorised by visual condition. When analysed according to specific test conditions, differences were found in measures of single-leg stance with the eyes closed or on an unstable surface, but no differences were found in tests using a stable surface with the eyes open. This interpretation is supported by the review by McKeon and Hertel13 who also failed to find any differences in static tests on a stable surface. Their review predominantly included participants with unilateral CAI, and the testing method was most commonly with the eyes open. Taken together, these findings suggest that challenging tests of postural stability are required to identify deficits.
Deficits were also found in performance of more strenuous stability challenges, such as jump tests, in people with recurrent ankle sprain. Time-to-stabilisation measures were all significantly longer in participants with recurrent ankle sprain compared with uninjured controls. This concurs with the review by Arnold et al,12 who used a broader definition of CAI, and therefore more dynamic stability tests may differentiate participants with CAI, however defined, from healthy controls.
The findings of this review suggest some bone and joint differences around the ankle. The talus had an increased radius and increased depth in the frontal plane in participants with recurrent ankle sprain. It has been suggested that these changes may predispose the ankle to reinjury due to the deeper curve increasing the bending amplitiude which limits the osteochondral restraint or the foot being placed in a more inverted position.23 Gait studies appear to demonstrate a change in ankle position, into an inverted position, and decreased foot clearance during walking, which may be linked to the anatomical differences. These differences appear to be local and not to affect the more proximal joints. This evidence is limited due to the small number of studies, but it warrants further validation.
Participants with recurrent ankle sprain do not appear to have some of the deficits commonly believed to be associated with CAI. The meta-analysis did not demonstrate a deficit in the latency and motor response time for the peroneal muscles, consistent with the finding by Munn et al.14 In our review, only one of four studies found a delay in both the peroneals and tibialis anterior.54 However, this study used a different protocol to the other three, and it may be that delays are position-specific.
In this review, only concentric invertor weakness was demonstrated in participants with recurrent sprain, and this weakness is not in the direction or manner that would have been expected. Invertor weakness could be explained by the theory that an injured joint triggers an inhibitory reflex to muscles that are capable of increasing tensile stress on damaged ligaments.75 It has also been demonstrated that in comparison with controls, participants with CAI have a concentric evertor moment at heel-strike and during the loading response, and no invertor moment, which could result in an invertor/evertor imbalance.57 65 This result conflicts with Arnold et al's meta-analysis16 in which they found a small loss of concentric evertor strength in participants with ankle instability. Ankle instability was defined as the presence of functional ankle instability or ‘giving way’ or frequent sprains. However, Arnold et al comments that the size of the difference was small and may not be clinically relevant, similar to our findings for concentric inversion strength. It may also be that participants with other characteristics of CAI such as perceived instability or ‘giving way’, but not recurrent ankle sprain, have deficits in evertor strength.
Our recommendations are that further research is required in areas with ambivalent results. For example, it is expected that a deficit in proprioception would be present, particularly in the inversion direction, and this was the finding of Munn et al14 in their systematic review. A reason for the ambivalence may be that most papers did not adhere to psychophysical principles for measuring proprioception, which encourage many movements in a number of directions and varying speeds. This ensures consistent results are obtained in a system where thresholds vary with time.76 Only three papers in this review strictly used these principles,49,–,51 with the remainder only using two to three trials, often at one stimulus velocity. Two papers examined passive movement detection at three velocities and demonstrated that the inversion and eversion detection was worse50 in participants with recurrent ankle sprain but not dorsiflexion and plantarflexion.51 The study of active joint position matching in inversion movements found greater absolute error in participants with recurrent ankle sprain.49 Thus, more rigorous methods may reflect deficits in proprioception in the inversion and eversion directions, but future studies should consider adhering more strictly to psychophysical principles to clarify the findings. It is of interest that a study of passive movement detection in the inversion and eversion directions, which used the same protocol as the study in this review but different participant selection criteria, had contradictory results. De Noronha et al77 selected participants with functional ankle instability as measured by the Cumberland Ankle Instability Tool, and not by recurrent ankle sprain. Therefore, the different results may reflect different subgroups of CAI and provide a distinguishing feature for the groups.17
Another example of an area where further research would be of benefit is strength testing. Pure strength measures, in peak torque or concentric strength, have not yielded clinically significant differences. Testing to date, however, has not routinely used normalised strength measures, which may be one cause of inconsistency, or it may be that muscle strength is not what is required to effectively counteract excessive inversion forces, but the ability to rapidly generate force or to continually generate force effectively. In the quadriceps, it has been demonstrated that proprioception deteriorates when the muscles fatigue.78 These are areas that could usefully be further explored rather than the traditional strength measures.
Ambivalent results are also present in biomechanical studies, but the wide variety of tests and measures used make comparisons difficult. Certainly differences in magnitude and timing of ground reaction forces during gait were found in some research to date,56 60 and this would correspond to differences in time to stabilisation that have been consistently found. However, stabilisation differences have been found after jumping, a more challenging activity than gait, so changes in ground reaction force measures may require a more strenuous test (eg, running or jumping) to elicit definitive differences. Consistency in measures may also influence the results, and force measures being normalised for body weight would allow direct comparison of results.
In this review, there were few outcomes investigated that used measures easily implemented in the clinic. Ankle range of motion may be useful to monitor rehabilitation progress, but not as a distinguishing feature of recurrent sprain. Static balance testing should utilise more challenging tasks such as single-leg balance with the eyes closed, or standing on a movable surface, rather than with the eyes open on a stable surface. The star excursion balance test (SEBT) has been shown to be a useful dynamic balance measure in participants with a broader definition of CAI79 but the one paper considering recurrent sprain did not find any significant differences between groups.31 It may be that the SEBT distinguishes participants with other characteristics of CAI such as ‘giving way’. Stabilisation time is the other feature, which typically is not easily measured in the clinic, but the significant differences found on Eechaute et al's74 hop test requiring balancing between hops may be a successful measure that reflects stabilisation time.
There are limitations to the findings of this review, most notably that the populations studied were overwhelmingly young and male. Whether older less active people have similar characteristics is unknown. While the pooled effects indicated point estimates of both moderate and large effects,80 the large CIs resulted in only three outcomes being significant. The large variability could reflect the small number of studies and participants, or that despite limiting homogeneity, there may still be further subgroups within recurrent sprain. Further categorising CAI into groups such as recurrent sprain and mechanical instability, or recurrent sprain with perceived instability,17 may clarify which outcomes are important. The scope of the review limited the papers retrieved to those written in English, which may have biased the findings. Similarly, the breadth of research covered using different methodologies and measures made quality assessment difficult but may well be warranted in the future.
This review attempted to address inclusion criteria within the context of the detail provided in each study. We reviewed evidence relating to sensorimotor deficits in studies that involved participants with two or more sprains, as this was the greatest level of detail available. However, our inability to make a definitive statement on many of the sensorimotor deficits, for example, kinematics during gait, may be related to the fact that differences still existed between study populations, notwithstanding the common history of recurrent sprains. This highlights the need for greater clarity in description of study populations and contributes to the limitations of reviews in this area.
From this review, a number of directions for future research are apparent. Examining more homogenous subgroups of participants with CAI may clarify which tests and measures distinguish the subgroups, and which tests may need discarding. Our results differ from other reviews of CAI12,–,14 16 and suggest that the anatomy of the ankle and ankle positioning during movement, stabilisation time and challenging postural sway tests are likely to be impaired in participants with recurrent sprain. In addition, generalisation of results requires more gender equal and older study populations. Further research in these areas should also assist in translating laboratory-based tests into clinically applicable tests and measures.
What is already known
Studies of sensorimotor deficits in people with chronic ankle instability have been equivocal, which may be due to the heterogeneity of the populations studied; we aimed to clarifiy deficits in a more defined population with CAI, those with recurrent ankle sprains.
What this study adds
People with recurrent ankle sprains demonstrate greater postural sway when standing with the eyes closed or on unstable surfaces, and decreased concentric inversion strength; differences in evertor strength, inversion joint position sense, and peroneal latency in response to a perturbation were not found.
In conclusion, participants with recurrent sprain exhibit talar differences, decreased concentric invertor strength, increased postural sway when standing on a single-leg with the eyes closed, changed foot positioning during gait and an increased time to stabilise after a jump, compared with uninjured controls. We did not find any deficits in evertor ankle strength, ankle range of motion, joint position sense and peroneal latency.
References
Footnotes
-
Funding CEH was funded by a University of Sydney Postdoctoral Scholarship. C-WL was funded by the National Health and Medical Research Council.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.