Article Text

Abstract
Objectives This meta-analysis investigated the efficacies of foot orthoses, motion control footwear and therapeutic adhesive taping in controlling foot pronation as compared with no-intervention conditions.
Data sources Electronic searches on four electronic databases were performed and the reference lists of the screened articles were also scrutinised.
Review methods Two reviewers screened the quasi-randomised or clinical controlled trials that examined the efficacy of the selected interventions in controlling calcaneal eversion. Heterogeneity and publication bias were assessed by I2 index and Egger's regression intercept, respectively. Trial quality was rated by the Physiotherapy Evidence Database scale.
Results 29 studies were selected. The I2 indices revealed large heterogeneity which supported the use of a random effect model of meta-analysis. The Egger's regression intercepts suggested that publication bias of the included studies was marginally present in the motion control footwear and the therapeutic adhesive taping groups (p=0.06–0.07). All three interventions were effective in reducing calcaneal eversion (p<0.001) with therapeutic adhesive taping being most effective whereas Low-dye taping was less effective than the other taping techniques, such as high-dye and stirrups taping. Custom-made foot orthoses were more effective than prefabricated orthoses. Motion control footwear with heel flare or wedge design was less effective than those with dual midsole materials.
Conclusions Foot orthoses, motion control footwear and therapeutic adhesive taping were able to control rearfoot eversion with therapeutic adhesive taping being the most effective. In the clinical practice, selection of an antipronation intervention should be based on patient characteristics, type of activity and personal preference.
Statistics from Altmetric.com
Introduction
Foot pronation involves multiple joint movements at the rearfoot and midfoot1 and is a natural movement for shock absorption during the early to midstance phase of a gait cycle.2 However, people with excessive foot pronation are vulnerable to injuries such as metatarsal stress fracture,3,–,6 plantar fasciitis7 and Achilles tendonitis.8 9 Also, with the potential movement coupling between internal tibial rotation,10 excessive foot pronation may lead to problems in more proximal body parts, including medial tibial stress syndrome11 12 and patellofemoral pain.13,–,15
Even though there is no consensus on the definition of foot overpronation, much emphasis has been placed in controlling abnormal foot motion in the clinical situation. Different intervention strategies have been developed for controlling foot pronation and among them, foot orthoses, motion control footwear and therapeutic adhesive taping are the most commonly used interventions by clinicians.
The rationales of these three approaches are different. Foot orthoses, be they custom-made or prefabricated, are intended to align the foot by providing extra external support on different foot structures, for example, foot arch support.16 Motion control footwear allows deceleration of foot pronation during the touch-down phase of running and limits pronation in the midstance phase,17 18 by either heel flare/wedge design or midsole modification. Therapeutic adhesive taping controls the joint movements by applying external tension over the skin19 and among the different types of taping, ‘Low-dye taping’ is one of the most popular techniques used by the clinicians.
Although the above interventions for controlling foot pronation have been practiced for a long time and there is a growing pool of literature reporting their effects, the conflicting findings among studies had made it difficult for clinicians to decide on the efficacies of these techniques. Moreover, the small sample sizes typically reported in the clinical studies would often result in underpowered findings. To date, there has been no study comparing the efficacy of the antipronation interventions. Better understanding on their efficacies may improve the clinical outcome and cost-effectiveness of the clinical service.
Therefore, the purpose of this systemic review with meta-analysis was to investigate the efficacy of different antipronation interventions in reducing calcaneal eversion during gait.
Methods
Search strategy
An extensive literature search for all quasi-randomised and clinical controlled trials examining efficacy of foot orthoses, motion control footwear and therapeutic adhesive taping was conducted using the MEDLINE (PubMed), EMBASE, CINAHL and AMED databases (updated to November 2010). The keywords and phrases used in the online search included ‘foot’, ‘rearfoot’, ‘pronation’, ‘calcaneal eversion’, ‘kinematics’, ‘motion’, ‘foot orthoses’, ‘taping’ and ‘motion control footwear’. The detailed electronic search strategies are shown in the appendix. Reference lists from published papers were also reviewed in order to identify any other relevant studies not cited in the online databases.
Selection
Articles were included in the systematic review if they fulfilled the following criteria: (1) quasi-randomised controlled trials or clinical controlled trials published in peer-reviewed journals; (2) subjects being tested were diagnosed as having musculoskeletal conditions potentially related to excessive foot pronation3,–,9 11,–,15 and otherwise healthy; (3) comparing the antipronation interventions, namely, foot orthoses, motion control footwear and therapeutic adhesive taping with a no-intervention control group; (4) calcaneal eversion was used as the outcome measure of foot pronation; (5) measuring the foot pronation during activities of standing, walking or running and (6) the full text was written in English. The exclusion criteria were (1) studies not meeting the minimum requirements of an experimental study design (ie, case report or review article); (2) studies on subjects with any neurological pathology and (3) studies that did not compare the selected interventions in a weight-bearing condition.
Two independent reviewers screened the title and abstract of each article to decide whether it should be selected based on the preset criteria. For the actual review, two criteria were used to determine whether the article should be included in the analysis: (1) tabular means and SD were available for the control and intervention groups. In articles wherein data reporting was incomplete, the authors of the articles would be contacted for clarifications and (2) the quality of the study was satisfactory according to the Physiotherapy Evidence Database (PEDro) scale.20
In order to accommodate studies with different methodologies, the outcome used in this study was restricted to the change in calcaneal eversion. Calcaneal eversion was one of the most common dynamic outcome measurements for foot pronation. Even though other outcome variables such as change in pronation velocity and pronation angle during initial heel contact were clinically important, in the absence of a common definition of these variables among studies, extraction of these data for this meta-analysis was not done.
Quality assessment
The quality of the studies included in this analysis was evaluated by the PEDro scale20 by two independent reviewers. This quality assessment tool rates the methodology of an experiment based on subject allocation and randomisation, treatment randomisation, level of blinding, ‘intention-to–treat’ approach as well as the reporting of the results. This instrument had demonstrated good reliability (intraclass correlation coefficient = 0.68; 95% CI 0.57 to 0.76), especially for consensus rating.20 Disagreements about the PEDro criterion score were resolved by a third reviewer. Using this criterion-based evaluation tool, any study scoring eight or above would be classified as a high-quality clinical trial.21 However, the median PEDro scores for sports physiotherapy trials and overall randomised controlled trials were only 4 and 5, respectively.21 Selection of this original cut-off value could filter the majority of studies that presented the best evidence in the current literature. Therefore, the cut-off value for this meta-analysis was adjusted and those studies scoring 5 and above were included.
Statistical methods
All the data from each of the studies included were entered as the mean differences between the experimental and no-intervention control group and their corresponding SDs. The pooled mean difference of treatment effects was calculated and illustrated by forest plots with Review Manager (RevMan) version 5.0 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). The heterogeneity of the included studies was tested by I2 index. The I2 index was selected instead of the Q statistics because the latter only provided information regarding the existence of heterogeneity, but it did not quantify the extent of such heterogeneity.22 I2 index of ≤50% demonstrated low heterogeneity and supported a fixed-effect model in the meta-analysis. On the other hand, random effect model in the meta-analysis should be used when the I2 index was >50%,22 which was suggestive of a moderate to high heterogeneity of the studies.
Bias funnel plots were used to illustrate the relationship between intervention effect and SE in each intervention. Publication bias assessment was tested by the Egger's regression intercept23 using Comprehensive Meta Analysis version 2 (Biostat, Englewood, New Jersey, USA). A p value of <0.1 (two-tailed) in the test indicated the presence of publication bias.
Results
After completing the initial electronic search, 59 articles were identified (figure 1). Among the 59 studies, 19 had not examined the target outcome measurements in this meta-analysis and were excluded. One had not evaluated the intervention for foot pronation control and it was also excluded. Of the remaining 39 reports, 1 was excluded because that manuscript was not written in English. Two case studies and two review articles were also excluded. Another study was rejected due to incomplete results reported (by graphical presentation) and the authors of that study did not reply to our inquiry. Four others did not meet the inclusion criteria due to duplication of data with another study, subjects demonstrating different landing patterns and the study design was not experimental in nature. The remaining 29 reports were included in this meta-analysis (tables 1–3). Among these 29 reports, 13 had studied foot orthoses, 10 had studied motion control footwear and 10 had studied therapeutic adhesive taping. Some studies had examined more than one antipronation intervention; thus, the total number exceeded 29.
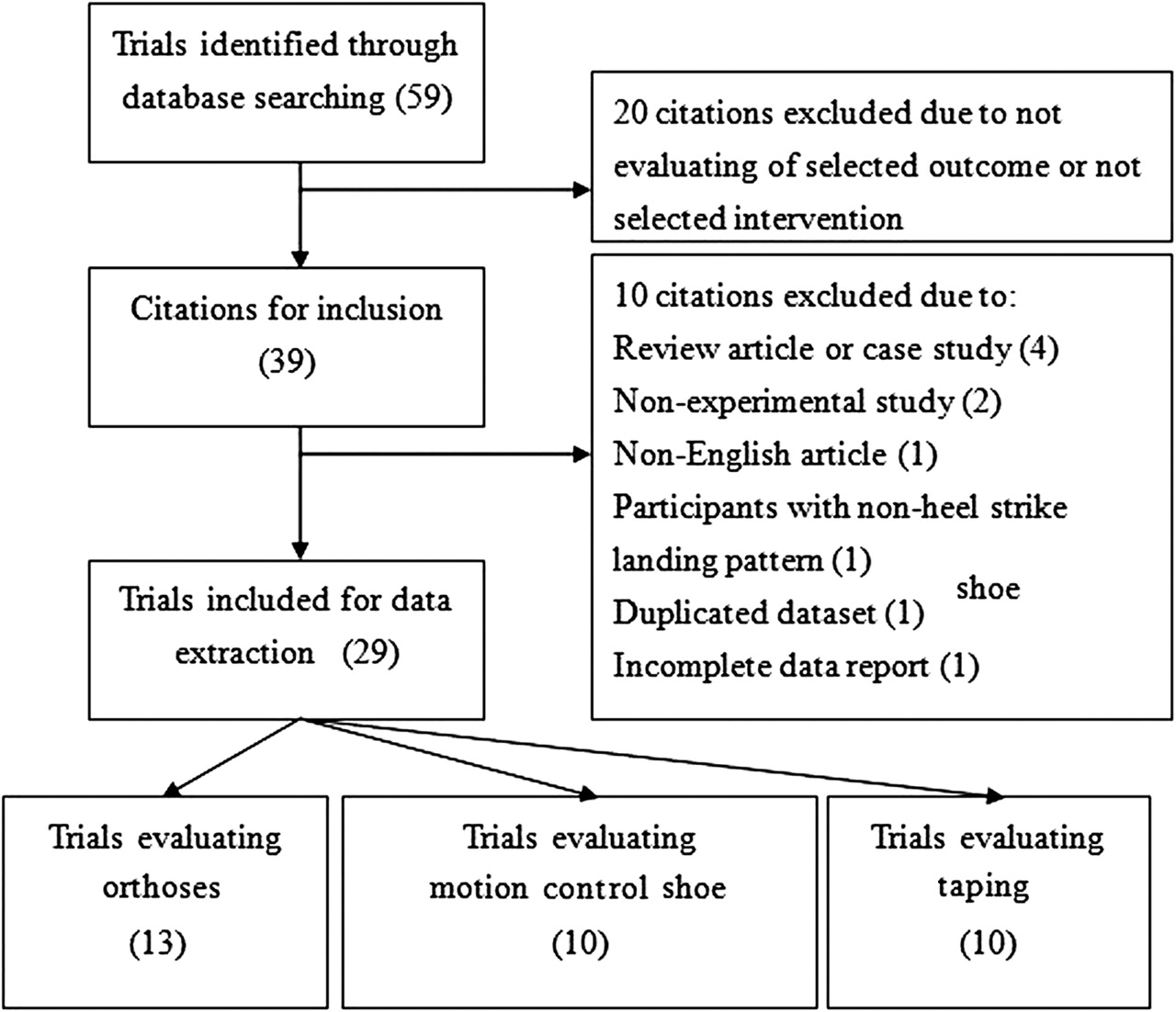
Flowchart of trial selection process.
The summary of included studies examining the efficacy of orthoses
The summary of included studies examining the efficacy of motion control shoe
The summary of included studies examining the efficacy of therapeutic taping
The total number of subjects involved in these studies was 486. The characteristics of the subjects were presented in table 4. The PEDro scores of the selected studies were listed in table 5. The average ratings for the research related to foot orthoses, motion control footwear and therapeutic adhesive taping were 5.38, 5.56 and 5.43, respectively.
Characteristics of participants in the included studies
PEDro criterion score of included studies
High heterogeneity between data sets was found in studies with different interventions and the I2 was 65% in the foot orthoses group, 92% in the motion control footwear group and 92% in the therapeutic adhesive taping group. In other words, variability in treatment effect estimates was not only due to sampling error within studies; thus, the use of a random effect model in the meta-analysis was deemed appropriate.22
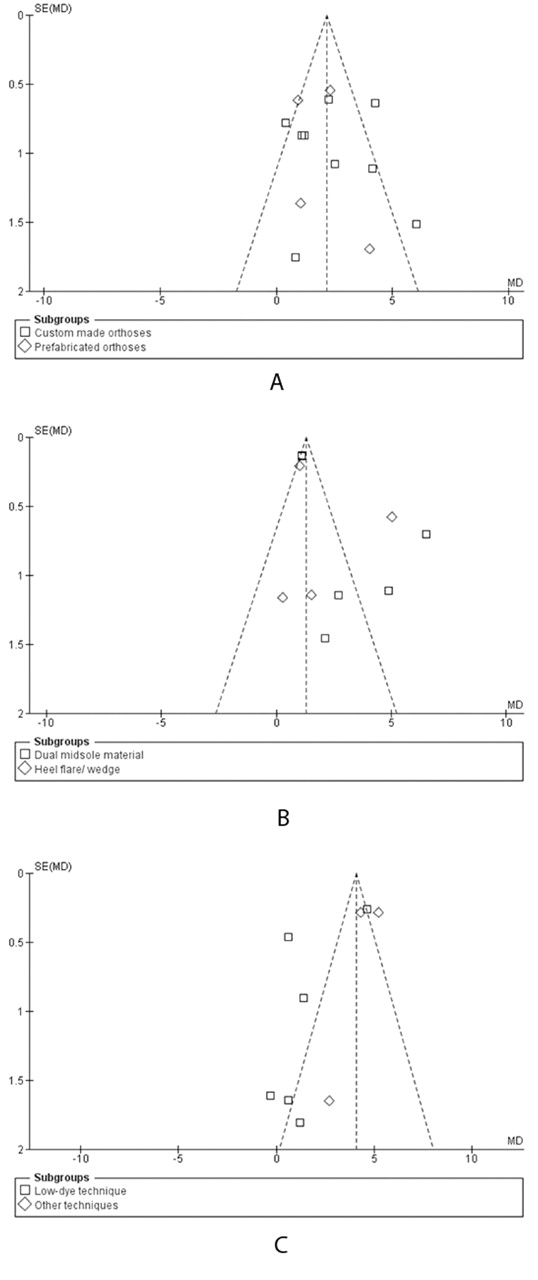
The bias funnel plots of these studies were shown in figure 2. Egger's regression intercepts were 0.67 (p=0.64, two-tailed) for the foot orthoses group, 2.95 (p=0.06, two-tailed) for the motion control footwear group and −3.52 (p=0.07, two-tailed) for the therapeutic adhesive taping group. These results suggested that publication bias was not present in the foot orthoses group but marginal publication bias existed for both motion control footwear and therapeutic adhesive taping groups.

(A) Funnel plot of included studies (orthoses). (B) Funnel plot of included studies (motion control shoe). (C) Funnel plot of included studies (therapeutic adhesive taping).
The weighted mean reduction in calcaneal eversion and pooled variance data for individual antipronation interventions were represented by forest plots (figure 3). The reduction in calcaneal eversion for three antipronation devices was significant when compared with no-intervention control (p<0.001). The reduction with therapeutic adhesive taping was the highest (mean difference=2.64°; 95% CI=1.39 to 3.90; Z=4.13), followed by the motion control footwear (mean difference=2.52°; 95% CI=1.71 to 3.33; Z=6.10). The reduction in calcaneal eversion for foot orthoses was the least (mean difference=2.24°; 95% CI=1.42 to 3.07; Z=5.30), although the overall difference between the most effective and least effective interventions was less than 0.5°.

{kind=link}
{kind=link}
{kind=link}
(A) Forrest plot for efficacy of custom and prefabricated orthoses. (B) Forrest plot for efficacy of motion control shoe with duo midsole material and heel flare or wedge modification. (C) Forrest plot for efficacy of motion control shoe with Low-dye taping and other taping techniques. Squares represent the mean difference presented by an individual study. Diamonds represent overall effects of a group of studies.
When comparing within the intervention category, custom-made orthoses (group defined by presence of description of molding procedures for each participant) had demonstrated a higher weighted mean change in calcaneal eversion reduction (mean change=2.35°; 95% CI=1.24 to 3.45; Z=4.17; p<0.001) than prefabricated orthoses (group defined by the absence of description of molding procedures for each participant or statements to claim the use of prefabricated orthoses) (mean change=2.08°; 95% CI=0.66 to 3.51; Z=2.87; p=0.004).
On the design of motion control footwear, the footwear with dual materials in the midsole (mean change=2.77°; 95% CI=1.74 to 3.81; Z=5.26; p<0.001) had produced a reduction in calcaneal eversion. Conversely, the effects of motion control footwear with heel flare or wedge modification were not significant (mean change=2.02°; 95% CI=−0.34 to 4.38; Z=1.67; p=0.09).
Results of the therapeutic adhesive taping techniques revealed that Low-dye taping had a non-significant weighted mean change in the reduction of foot pronation (mean change=1.50°; 95% CI=−0.73 to 3.73; Z=1.32; p=0.19). Interestingly, other taping techniques, including high-dye and stirrups taping techniques, were found to be effective in controlling foot pronation (mean change=4.62°; 95% CI=3.73 to 5.50; Z=10.26; p<0.001).
Discussions
This meta-analysis attempted to compare the efficacy of three different antipronation interventions for controlling foot pronation and the different application methods within each intervention. The findings revealed that foot orthoses were the least effective for controlling foot pronation as compared with motion control footwear and therapeutic adhesive taping. However, the overall difference in foot pronation among the three interventions was less than 0.5°. Such a small difference may not be clinically meaningful and it could be due to measurement error. Apart from the work by Stacoff et al,24 25 all the studies in this meta-analysis had used skin markers for capturing motion. Although a few studies had applied the markers on the shoes while others had the markers on the skin, the data collected from either skin markers or shoe markers tended to overestimate the true skeletal movement due to relative movement between the skin and underlying bony structures.26
The subcategory comparisons suggested that custom-made orthoses were more effective than prefabricated orthoses. A likely reason was that the custom-made orthoses involved more professional input such that individual foot postures could be better assessed and managed by the therapists. Besides, as there were only five studies investigating the prefabricated orthoses, the analysis based on those few studies might not be conclusive.
The technology of motion control footwear was developed approximately three decades ago and it had been shown to be effective in checking excessive foot pronation. Compared with the other two interventions, motion control footwear is less dependent on the application technique than foot orthoses and therapeutic adhesive taping. This makes it to be more convenient for the users. In addition, it is a good alternative management for patients in the stage of weaning off from direct clinical consultation after initial prescription of motion control footwear.
There were two design theories for motion control footwear.13 The older design was the use of heel flare or wedge modification whereas the more modern design consisted of dual materials in the midsole. The functioning mechanism of the dual-material midsole was based on the fact that a softer lateral midsole would provide better cushioning during initial contact and a firmer medial midsole would limit the foot pronation by additional support.17 The pooled results in this study suggested that the new design was more effective for controlling calcaneal eversion. In addition, the heel flare or wedge design would increase the lever arm of the landing moment thus leading to higher risk of ankle sprain.17
The therapeutic adhesive taping was found to be the most effective in reducing calcaneal eversion. Therapeutic adhesive taping, often applied by a therapist, could have an additional advantage over the motion control footwear and foot orthoses because the subjects would be assessed every time before taping. The change in foot condition could be assessed and managed more effectively by the therapist. However, therapeutic adhesive taping would become less effective some time after application and it is therefore not suitable as a long term intervention.
Regarding the different taping techniques, ‘Low-dye taping’ is one of the most popular techniques among clinicians. Low-dye taping consisted of an anchor strip and a series of transverse strips. The anchor strip, starting from the fifth metatarsal head to the back of the heel and mounting to the first metatarsal head, provided the base for attachment of the transverse strips. The transverse strips running from lateral to medial of the anchor strip under the plantar surface of the foot would counteract the pronation movement.27 However, it was not shown to be effective in checking excessive foot pronation. The low effectiveness demonstrated could be due to the testing condition of the experimental setup in the studies. Among the five studies involving this taping technique, none had adopted a running test. The lesser amount of foot pronation in normal walking or static standing position might underestimate the treatment effects in this group thus leading to the findings being insignificant.
Results of this meta-analysis indicated that other taping techniques were more effective for controlling foot pronation than the Low-dye taping. It could be because its longer anchor onto the skin had provided more leverage to control foot pronation. However, such findings should be interpreted with caution because there was little information on other taping techniques and only three studies could be identified for this analysis.
On the basis of Egger's regression intercepts, the studies on foot orthoses group did not demonstrate publication bias but marginal publication bias did exist in both the motion control footwear and therapeutic adhesive taping groups. This implied that the papers were true representatives of all the valid studies in the foot orthoses group only. This finding also supported the view that studies in the foot orthoses group with larger sample size would demonstrate larger treatment effects and vice versa. On the other hand, the overall treatment effect of motion control footwear and therapeutic adhesive taping might have been overestimated thus the data should be interpreted with caution.
The reason for choosing 5 out of 11 as the quality threshold for the papers in this meta-analysis was based on the fact that the median score in PEDro scale among sports physiotherapy trials and overall randomised controlled trials were only 4 and 5 out of 11, respectively.21 Although the quality of all the studies included in this meta-analysis was above the 50th percentile in the literature, the mean PEDro scores in three intervention groups were only marginally above the selected cut-off point. In most of the studies included, the subject allocation and treatment sequence were not randomised. To improve the quality of future research, this issue should be addressed. The other common criterion that most studies had failed to score was on subject blinding. Placebo taping (tape applied on the skin without application of force) and flat shoe insert had been used as controls for therapeutic taping and orthoses. In addition, subject blinding is possible when studying motion control footwear, as the subjects may not be able to differentiate the type of footwear according to their sensation and proprioceptive feedback.17 High-quality randomised controlled trials in this area are feasible and warranted.
Conclusion
We concluded that foot orthoses, motion control footwear and therapeutic adhesive taping were effective in controlling foot pronation compared with no-intervention control. Among these interventions, therapeutic adhesive taping was more effective than the other two interventions and foot orthoses was shown to be the least effective. However, the difference in calcaneal eversion reduction between therapeutic adhesive taping and foot orthoses was less than 0.5°. In clinical practice, the selection of antipronation intervention should be based on patient characteristics, type of activity and personal preference.
Acknowledgments
The authors thank Professor Thomas McPoil of Regis University for his comments and technical advice on this manuscript.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous