Article Text

Abstract
Objectives To investigate the short-term clinical efficacy of in-shoe foot orthoses over a wait-and-see policy in the treatment of anterior knee pain (AKP) and evaluate the ability of foot posture measures to predict outcome.
Design Single-blind, randomised control trial.
Participants Forty participants (18–40 years) with clinically diagnosed AKP of greater than 6-week duration, who had not been treated with orthoses in the previous 5 years.
Intervention Prefabricated orthoses perceived as most comfortable from a selection of 3 different hardness values compared with a wait-and-see control group.
Outcome measures Participant-perceived global improvement, Kujala Patellofemoral Score, usual and worst pain severity over the previous week and the Patient Specific Functional Scale measures at 6 weeks.
Results Foot orthoses produced a significant global improvement compared with the control group (p = 0.008, relative risk reduction = 8.47%, numbers needed to treat = 2). Significant differences also occurred in measures of function (standardised mean difference = 0.71). Within the intervention group, individuals who exhibited a change in midfoot width from weight bearing to non-weight bearing of >11.25 mm were more likely to report a successful outcome (correct classification 77.8%).
Conclusion This is the first study to show orthoses provide greater improvements in AKP than a wait-and-see approach. Individuals with greater midfoot mobility are more likely to experience success from treatment.
Trial Registration ACTRN12611000492954
Statistics from Altmetric.com
Introduction
Anterior knee pain (AKP) is a debilitating condition1 occurring in 25% of the active population.2 3 Conservative management is considered the principal treatment,4 and in-shoe foot orthoses are often used in conjunction with, or as alternative to, other techniques. Clinically, orthoses are normally prescribed to individuals exhibiting excessive pronation. This is despite growing evidence supporting the use of orthoses in the treatment of AKP regardless of foot posture, with improvements in pain and function being observed from immediately upon application5 to weeks and continuing after months of wear.6 Interestingly, a post hoc analysis of the latter study identified greater medio-lateral midfoot mobility (arguably a surrogate indicator of greater pronation)7 as one of four predictor variables improving the success of orthoses treatment.8 Although there is growing research evidence in support of using orthoses, no study has considered natural history as a comparator. Therefore, the clinical efficacy and amount of improvement solely attributable to an orthosis remains unknown. There is a need for a clinical trial using a wait-and-see comparator.
This study primarily investigated the short-term clinical efficacy of in-shoe foot orthoses over no orthoses and followed this up with an evaluation of the ability of foot posture measures to predict outcome.
Methodology
The study was a single-blind, randomised controlled trial. As per previous clinical trials,6 9 inclusion criteria were (1) age 18–40 years; (2) anterior or retropatellar knee pain of a non-traumatic origin with duration exceeding 6 weeks; (3) aggravated by at least two of the following activities: running, hopping, hill or stair walking, prolonged sitting or kneeling, or squatting and (4) pain of palpation of the patellar facet or double leg squat. In addition, we also included only those who demonstrated at least two of the following: a more mobile foot as defined by greater than 10.96-mm change in midfoot width from weight-bearing to non-weight-bearing position as per a previously described protocol;7 10 pain severity less than 53/100 mm on a visual analogue scale; older than 25 years; and shorter than 165 cm. These criteria were identified in a recent study as improving likelihood of success.8 Exclusion criteria were (1) concomitant pain or injury in the hip, pelvis or lumbar spine; (2) damage to any knee structures or indications of patella tendinosis; (3) chronic patella instability (4) knee effusion; (5) any foot conditions that would preclude the use of orthoses; (6) the use of physiotherapy treatment for knee pain or foot orthoses in the previous 3 years or (7) previous lower limb surgery.
The study took place at the Australian Institute of Sport (Canberra, Australia) with participants sourced locally through advertisements. On expressing interest, potential participants were interviewed to screen for major inclusion and exclusion criteria. Two physiotherapists (KM and PB) physically examined suitable participants to confirm a diagnosis of AKP. Eligible participants provided informed consent prior to inclusion into the study.
Intervention
Four prefabricated, full-length, commercially available orthoses (Vasyli International, Brisbane, Australia) constructed of ethylene-vinyl acetate with fabric covering were used. Three orthoses exhibited identical contouring and posting and intrinsic medial posting/wedging (manufacturer's specifications) and were hard (Shore A 75°), medium (Shore A 60°) and soft (Shore A 52°). The fourth orthosis featured identical Shore A value to the soft orthosis but was of uniform thickness (3 mm) along its length. The orthoses were fitted as per a modified protocol used in a previous randomised control trial (RCT),11 which involved ensuring that the medial longitudinal arch of the orthoses did not impede motion of the first metatarsal head. Varying sizes were trialled in order to optimise fit, and some trimming of the orthoses where required was done to fit into the shoe, as per manufacturer's guidelines. No heat moulding was performed and no additions applied. Either the fitted orthosis or sock liner was used for the trial period.
Primary outcome measure
Global Improvement Scale
Each participant's self-perceived level of improvement was measured at the 6-week follow-up using a 6-point Likert-type scale. The categories were completely recovered, much improved, improved, no change, worse and much worse.12 13 The categories much improved and completely recovered were regarded as indicating success.12 14
Secondary outcome measures
Pain severity
Horizontal visual analogue scales (VAS), anchored by ‘no pain’ (0 mm) and ‘worst pain imaginable’ (100 mm), were used to measure usual and worst pain over the previous week. A change in score of 20 mm was considered a clinically meaningful change.15
Kujala Patellofemoral Score
The Kujala Patellofemoral Score (KPS) is a 13-item questionnaire categorically related to symptoms and varying levels of current knee function, such as weight bearing (WB), running, jumping and prolonged sitting with knees flexed. Each response is weighted and a total summed resulting in an overall score from 0 to 100, where higher scores represent greater function and less pain.16 A change exceeding 10 points was regarded as clinically meaningful.15 17
Patient Specific Function Scale
The Patient Specific Function Scale (PSFS) involves participants listing up to five activities they perceive as important but are having difficulty completing, or are unable to complete, due to their current condition. Participants rate the difficulty associated with that task from 0 (unable to perform) to 10 (able to perform activity at the same level as before injury or problem). The sum of activity scores is divided by the number of activities to calculate a PSFS score. A change of 2 points was regarded as clinically meaningful.18
Baseline foot posture measures
To evaluate our second aim, we measured foot posture with a foot assessment platform previously described,7 which has been found to be a reliable and valid measuring tool.10 Static measures of the foot in WB and non-weight bearing (NWB) were taken for midfoot width and dorsal arch height. The difference between WB and NWB measures were used to calculate the difference in midfoot width and dorsal arch height. The composite ‘foot mobility magnitude’ was calculated using a Pythagorean-based function of the difference scores. This approach was chosen because the foot posture index and normalised navicular drop, which are other commonly used foot posture/mobility measures, have recently been shown not to improve the likelihood of orthosis success.19
Procedure
Upon enrolment into the study, participants were randomly assigned to the intervention or control group with a computer-generated randomisation method (Math.random in JavaScript).20 An automated data file was used to preserve allocation concealment.
Upon inclusion into the trial, all participants were sized for orthoses while blinded to the differences between orthoses. Baseline measures were recorded, and then participants jogged, on a treadmill, in 3-min intervals alternating between their usual jogging shoe and their shoe with an orthosis inserted until all four orthoses had been trialled. Shoes were inspected for excessive wear (KM) prior to commencement in the study. Participants were asked to self-select a speed that would not provoke knee pain and that they could maintain throughout the session. To ensure blinding, orthoses were inserted and removed out of participants' field of view.
After the session, participants were asked to rank the orthoses from most to least comfortable. A ranking scale was chosen as this has been shown to be the most reliable measure of footwear comfort.21 Participants allocated to the intervention group were then assigned their most comfortable contoured orthosis (when the flat orthosis was ranked 1, the contoured orthosis ranked 2 was assigned) (table 1) because comfort has been identified as a potential indicator of success,22 and perhaps more importantly discomfort is a primary reason for patients discontinuing use.23 Intervention group members were instructed to wear their orthoses as much as possible and to contact the investigators if they experienced any adverse reactions (eg, blistering, pain etc). Members of the control group were instructed to continue wearing their usual shoes.
Frequency each orthosis received the most comfortable ranking. For the intervention group, the orthosis perceived as most comfortable was assigned for the intervention period
Follow-up outcome measures were conducted by an assessor blinded to baseline measures.
Sample size
Sample size was calculated using an α of 0.05 and β of 0.05 and assuming 30% of the control group would report improvement. To achieve 85% success with orthoses as in the Collins et al study (ie, 55% difference from control) required 18 per group (n = 20 with 10% dropout allowance).
Statistical analysis
Statistical analyses were conducted in SPSS (version 16, SPSS Inc, Chicago, Illinois, USA) and R (version 2.12.1, R Foundation for Statistical Computing, Vienna, Austria). The two groups were compared at baseline using independent t-tests. Dichotomised global improvement was analysed using Fisher's exact test and expressed as numbers needed to treat and relative risk. Secondary, continuous outcome measures were analysed using univariate analysis of covariance with baseline as a covariate and group as a fixed factor. Duration of pain was also entered as a covariate for the KPS and PSFS as it has been identified as influencing the 6-week prognosis of these outcomes.24 Significance was set at 0.05 and change scores from baseline to follow-up were compared with previously established MCIDs to determine clinical importance. Results are reported as the mean (95% CI) and standardised mean difference (SMD = mean difference/pooled SD). SMD is referenced to Hopkins' classification of trivial (<0.2), small (0.2–0.6), medium (0.61–1.2) and large (>1.2).25
Following the main analysis, a classification tree was applied to the data in order to identify which baseline characteristics contributed towards the success of the participant on the dichotomised Global Improvement Scale. Briefly, the classification tree method grows a decision tree determined by a sequence of binary decision rules for relating an outcome variable (success) to various predictors (table 2). This is done by recursively partitioning the predictor space into rectilinear regions of increasing homogeneity as measured by a classification criterion such as entropy or sample variance.26 As this approach tends to over-fit to the data, the tree was pruned by subjecting the size of the tree to a penalty parameter that balances goodness of fit against the ability to generalise the fitted relationship to the broader population.27 The classification tree27 was then cross-validated to ensure the amount of pruning was appropriate.26
Participant demographics and baseline measures
Results
From August 2009 to May 2010, there were 126 enquiries of which 51 individuals were clinically examined resulting in 40 enrolled participants. There were no significant differences between the groups at baseline (table 2). The trial finished in June 2010 with one participant withdrawing from the study due to an acute traumatic episode of lower back pain unrelated to orthosis use (car accident) (figure 1).
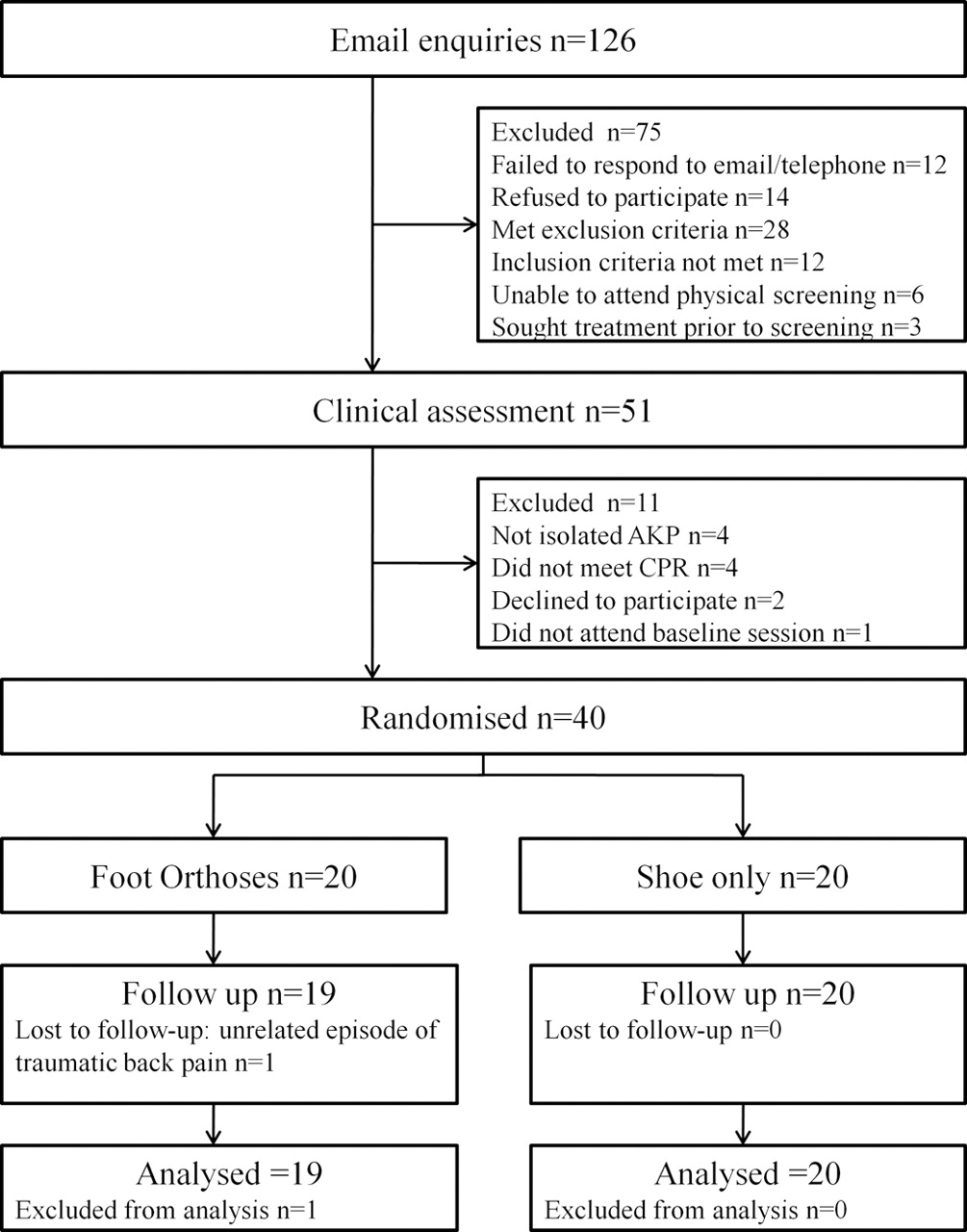
Flow of participants through study.
At follow-up, there was a significant difference in the global improvement between the orthosis and control group (χ2 = 7.086, p = 0.008). Within the orthosis group, success rate, expressed entirely by ‘marked improvement’, was 47.37% (9/19), RR reduction 8.47% (3.1 to 12.74) and numbers needed to treat (NNT) of 2 (2–7) (figure 2). A significant, moderate effect (SMD = 0.71) in favour of foot orthoses was also present on the PSFS (table 3); however, the difference between groups was below clinically meaningful levels.18 There was no difference between groups in the KPS and pain severity measures, although there was a tendency in favour of orthoses for the KPS (4.13 (−0.06 to 8.33) SMD 0.44 p = 0.053).

Percentage of participants' ratings of global improvement across different categories. Note that there were no reports of ‘completely recovered’ or ‘much worse’.
Mean (SD) and mean difference (95% CI) between groups for secondary outcome measures adjusted for baseline values
The classification tree produced two splits. The first, most important, split predicting successful outcome was the presence of orthoses. Within the orthoses group, the variable difference in midfoot width was identified as the covariate most consistently associated with low classification error rates based on cross-validated. Nine participants were deemed as successes and 10 as non-successes (figure 3). Of the 9 participants with a difference in midfoot width exceeding 11.25 mm, 7 were successes while 2 were not. These 2 are considered to be classification errors with respect to the fitted tree model. For the 10 participants in the orthoses group whose midfoot width difference fell below 11.25 mm, 8 were correctly classified as non-successes and 2 resulted in classification errors.

{kind=link}
{kind=link}
{kind=link}
Classification tree analysis showing predictor variables for treatment success.
Adverse events
Early in the study, one participant reported blistering in the medial arch of the foot after wearing orthoses. This did not prevent them from wearing their orthoses.
Discussion
We found that after 6 weeks, patients with AKP who had used foot orthoses reported greater improvements than patients in the wait-and-see group. A striking finding was that NNT = 2; only two people need to be treated with orthoses for one more person to report his or her symptoms have much improved in 6 weeks than those without an orthosis. This finding indicates a better chance of success over natural history when compared with a previous RCT that reported an NNT of four of orthoses over a flat insert.6
Interestingly, the only secondary outcome measure to demonstrate significant, though moderate improvements, was the PSFS, a measure of patient-perceived function. That is, secondary outcome measures that capture pain severity (wholly or in part) were not different in the 6-week time frame. This was not a surprise as multidimensional outcome measures may be more appropriate to measure change in AKP than one-dimensional measures as it is a syndrome marked by pain, disability and functional limitation.15 28 Arguably, the Global Improvement Scale is the sum total of a number of dimensions of a patient's AKP experience (perhaps weighted according to some internal schema of the patient), and as such the results from the Global Improvement Scale tend to support the use of multi-dimensional outcome measures. Previous examination of the sensitivity to change of common outcome measures referenced to the Global Improvement Scale found the KPS usual and worst pain VAS to be the most responsive to change.15 In the current study, these measures did not differentiate between groups in 6 weeks, though patient-nominated specific functional activities did show a difference between groups. Our results indicate that in the short term, outcome measures including pain are not as sensitive to change as those specifically targeting function as in PSFS and possibly as a large component of the Global Improvement Scale.
This study also builds on previous clinical trials, which evaluated relative efficacy of orthoses to a comparator.6 29 After 6 weeks, Collins et al6 reported significant difference in global improvement between an orthosis and flat insert group. Similarly, after 8 weeks of orthoses wear, Eng and Pierrynowski29 reported their cohort of adolescent females experienced greater reduction in pain than a matched flat insert group during specific functional activities, namely, running, stair climbing and squatting. The orthoses used in the previous and current studies were prefabricated; however, both Collins et al6 and Eng and Pierrynowski29 afforded some degree of customisation through heat moulding and individualised posting. The similar feature across all orthoses' designs was the presence of medial posting. A recent meta-analysis found orthoses that were medially posted systematically reduced tibial internal rotation by 1.66° (95% CI 0.2 to 3.13) in currently injured cohorts.30 This may be one mechanism by which orthoses exert their effect. Reducing internal tibial rotation can produce a concurrent reduction in internal femoral rotation thus decreasing lateral compressive forces on the patella and subsequently improving AKP.31
The second aim of this study was to determine the role of foot posture/mobility in predicting the success of orthosis treatment. The difference in midfoot width from WB to NWB was identified as the foot mobility measure most consistently predicting orthosis success in this cohort. When treated with orthoses, people exhibiting a midfoot width difference greater than 11.25 mm were more likely to report success than those with lower midfoot mobility. This finding supports a previous report8 and suggests that of the four variables (age, height, pain severity and midfoot mobility) identified by the preliminary prediction rule, this is the most important. The current study found a difference in midfoot width of 11.25 mm as the cut-off as opposed to 10.96 mm in the previous study,8 though both showed similar improvements in success rate (27.6%8, 30.5% current study). The difference between 11.25 and 10.96 is less than a minimal detectible difference,7 and therefore either cut-off could be used clinically. Based on normative values from that reported by McPoil et al, both indicate a more mobile midfoot.7
The foot orthoses used in this study resulted in a single incidence of a minor adverse event experienced within the 1st week of wearing the prescribed orthoses (1/19, approximately 5%). Warning patients that there is a 5% chance of blistering on the plantar surface of the foot when orthoses are prescribed in this way is advisable. Fitting orthoses based on comfort may have assisted in the low adverse event rate.
In interpreting the results of this study, the reader should be aware of three key issues. First, the follow-up period for this study was 6 weeks, chosen on the basis that a significant global improvement over flat inserts was reported in a previous study.6 In hindsight, the lack of significant change in pain severity may be due to insufficient time. Collins et al6 and Eng and Pierrynowski29 noted reductions in pain occurred after 6 weeks. It is possible that while functional and patient-perceived improvement occur quickly, pain is slower to resolve. Second, the secondary analysis (the role of foot posture and mobility) is a subanalysis for which the study was not primarily designed. Therefore, further studies designed specifically to test foot mobility measures as predictors of outcome are needed. Nevertheless, this is the second study to identify the importance of midfoot width mobility and indicate this feature as an important consideration in orthosis fitting/prescription. Last, in considering implementation of this study's findings (external validity), it is important to refer to the inclusion criteria that were used, in particular that the findings of a prior clinical prediction rule were used (ie, patients had to exhibit two of the four variables (age, height, midfoot mobility and pain severity)).8
Summary
In-shoe foot orthoses, selected on the basis of comfort, produce improvements in 6 weeks that are beyond natural history in individuals with AKP, but this was mainly in the function domain. Those with greater width at the midfoot in WB relative to the NWB position were predictably improved for the orthosis but not the control group.
Acknowledgments
Authors thank Vasyli International for supplying the orthoses.
References
Footnotes
-
Funding KM is supported by the Australian Research Council. Financial support for this research was received from the Australian Research Council (Australian Research Council Linkage Project Grant LP0668233).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.