Article Text

Abstract
Data from the past five Olympic Games obtained from athletes seeking to inhale β2 adrenoceptor agonists (IBA) have identified those athletes with documented asthma and airway hyper-responsiveness (AHR). With a prevalence of about 8%, asthma/AHR is the commonest chronic medical condition experienced by Olympic athletes. In Summer and Winter athletes, there is a marked preponderance of asthma/AHR in endurance-trained athletes. The relatively late onset of asthma/AHR in many older athletes is suggestive that years of endurance training may be a contributory cause. Inspiring polluted or cold air is considered a significant aetiological factor in some but not all sports. During the last five Olympic Games, there has been improved management of athletes with asthma/AHR with a much higher proportion of athletes combining inhaled corticosteroids (ICS) with IBA and few using long-acting IBA as monotherapy. Athletes with asthma/AHR have consistently outperformed their peers, which research suggests is not due to their treatment enhancing sports performance. Research is necessary to determine how many athletes will continue to experience asthma/AHR in the years after they cease intensive endurance training.
Statistics from Altmetric.com
Introduction
Because of a significant increase in the number of Olympic athletes notifying the use of inhaled β2 adrenoceptor agonists (IBA) between 1996 and 2000, in 2001 the International Olympic Committee (IOC) resolved that athletes must justify their use of such drugs by demonstrating current asthma and/or airway hyper-responsiveness (AHR). This decision was not an antidoping measure but one to protect the health of athletes. Applications were reviewed by an Independent Expert Asthma Panel (IP) who had the responsibility of deciding if the athlete met the established criteria which have been published.1 Briefly, approval necessitated a positive bronchodilator or a bronchial provocation test. If the provocation test was negative, submission of the athlete's complete medical file may allow the IP to approve IBA use. Much of this information acquired between 2002 and 2006 has been published.1,–,3 In January 2008, at a Consensus Conference, the IOC reviewed this policy and resolved that it would continue.4 5 For the four Olympic Games between 2002 and 2008, a total of 1462 new applications and 201 renewals for IBA use were received and 1549 were approved. In January 2009, the World AntiDoping Agency (WADA) prohibited IBA and required athletes to obtain a therapeutic use exemption (TUE) to inhale IBA in and out of competition. WADA's criteria were identical to those of the IOC. However, in 2010, WADA partially reversed this policy, permitting salbutamol and salmeterol, although all other IBA remained prohibited.6 This policy change occurred a few weeks before the 2010 Olympic Winter Games in Vancouver, by which time virtually every athlete had obtained a TUE by 1 January 2010. Thus, this change had no significant influence on the athletes' prescribed medication,7 as confirmed by data sourced from WADA's AntiDoping Administration and Management System. The present study summarises key aspects of the information acquired from five Olympic Games between 2002 and 2010.
Outcomes
Asthma/AHR is the most common chronic medical condition encountered in Olympic athletes.
After early issues in 2002 and 2004 with doctors having difficulty with understanding the requirements, the percentage of athletes approved to inhale IBA stabilised between 7% and 8% (table 1). An additional number of athletes (0.5% to 1.3%) managed their asthma solely with ICS. This included some who failed to meet the criteria to be approved to use IBA. Thus, around 8% of Olympic athletes have asthma/AHR, the most common chronic medical condition encountered in Olympic athletes. At recent games, few athletes were noted to be using a long-acting IBA as monotherapy – only 5/186 in Vancouver and 5/781 in Beijing, all inhaling formoterol. In Vancouver 2010, no athlete was inhaling salmeterol without an inhaled corticosteroid (ICS), in contrast to Athens 2004 when more athletes inhaled salmeterol without than with an ICS.
Percentage of athletes approved to inhale β2 agonists (IBA) and percentage of athletes inhaling corticosteroids (ICS) with and without IBA in Olympic Games between 2002 and 2010
The concomitant use of inhaled glucocorticosteroids (ICS) with IBA has increased steadily, although this regressed in Vancouver 2010.
ICS is the ‘gold standard’ treatment for asthma and AHR.8 In 1996, only 46.1% of the 383 (3.6%) of athletes who notified the use of IBA were using ICS. For the Olympic Games between Atlanta 1996 and Athens 2004, ICS were permitted and no data are available. As table 1 indicates, since 2004 there was a steady increase in the percentage of athletes using ICS with IBA but the increased percentage of athletes using IBA as monotherapy in Vancouver 2010 was disappointing and evidence that education of doctors needs to continue to ensure athletes receive optimal management of their asthma/AHR.
Endurance-trained Olympic athletes – Summer and Winter – have a higher prevalence of asthma/AHR than non-endurance-trained athletes.
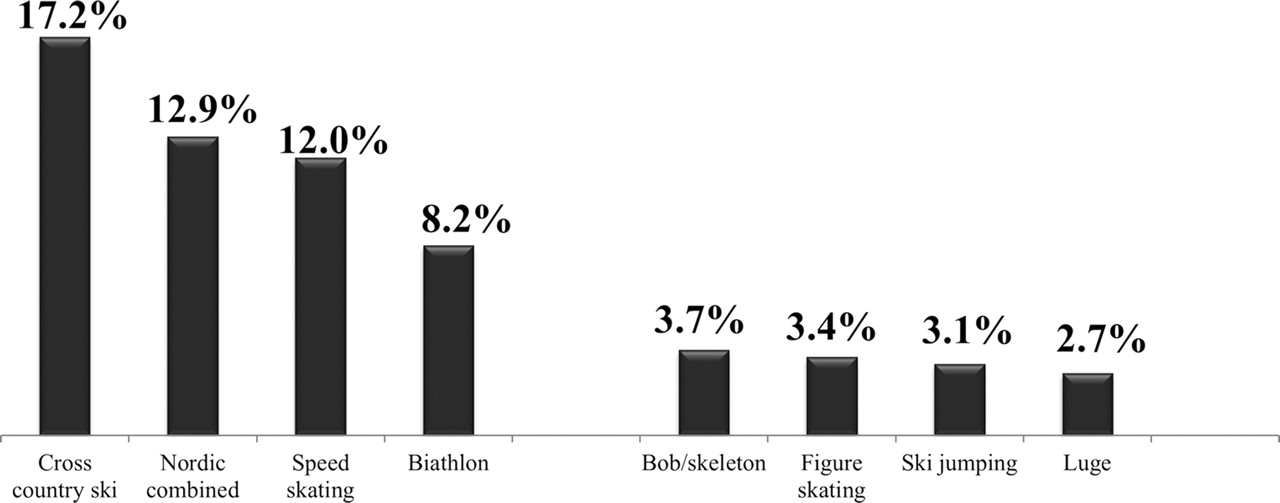
The classical discrepancy between endurance-trained and non-edurance-trained athletes is the fourfold difference in IBA approvals between Nordic-combined athletes who ski jump and then cross-country ski 15 km and ski jumpers who do not cross-country ski (figure 1).

Mean percentage of athletes approved for β2 adrenoceptor agonists use for 2002, 2006 and 2010. Winter Olympic Games – Only sports with highest and lowest percentages included.
Inspiring cold air contributes to airway injury in outdoor Winter athletes9 and to a lesser degree in indoor skating rinks, but the superimposed airway irritant of particulate matter (PM) from ice resurfacing machines may also provoke injury to the airways of athletes who train and compete in such venues.10 11
Figure 2 demonstrates that Summer Games athletes who undertake endurance training have a much higher prevalence of asthma/AHR than their counterparts in sports that have little or no endurance component in their training. The status of synchronised swimmers was surprising particularly in Beijing, when 21.2% of the 102 competitors were approved for IBA use which was higher than swimmers (19.3%). But synchronised swimmers spend as much time training in indoor pools as many swimmers and are continually filling their lungs and breathholding air which contains injurious chloramines, byproducts of the interaction of chlorine with organic matter.12 13 Yet to be determined is if their AHR and asthma will subside after they cease intense training.14 15 In addition to chloramines, the lungs of Olympic Summer athletes may be damaged by PM16 17 and ozone.18

Mean percentage of athletes approved for β2 adrenoceptor agonists use for 2004 and 2008. Summer Olympic Games – Only sports with highest and lowest percentages included.
Years of endurance training appears to be provoking airway injury and inflammation, perhaps with airway remodelling resulting in AHR and asthma.
The potential of years of endurance training contributing to asthma/AHR was suspected in Torino 2006 where of the 193 athletes approved for IBA use, 131 (67.9%) athletes stated that they had no history of childhood asthma. Of these, 85 indicated the onset of asthma/exercise-induced bronchoconstrictionwas aged 20 years or older and in 49 athletes, the onset of asthma was ≥25 years.3 As this finding indicated the likelihood that many years of intensive endurance training may have had a role in the development of AHR in some athletes, the 2008 online application form was modified to obtain improved information. In Beijing, the 781 athletes approved for IBA use were divided into those under or over 25 years of age at the start of the games.
Figure 3 is confirmation that some elite athletes are developing asthma/AHR late in their sporting careers. While for many, the quality of the inspired air may be injurious to their airways, this has not been so in all sports. A mean of 10.8% of rowers were approved for IBA use during the 2004 and 2008 Olympics and many rowers are tall with large lung volumes and thus can generate enormously high ventilation rates. For example, a 27-year 198-cm rower (forced expiratory volume in 1 s 6.9 l; forced vital capacity (FVC) 9.6 l) and gold medallist who developed asthma in his third decade had a ventilation of 1123 litre (mean 187 l/min) during his 6-min eucapnic voluntary hyperventilation test, which was positive. Clearly, if his minute ventilation approached this during the years of rowing training necessary to become an Olympic champion, his airways would have been exposed to repeated episodes of dehydration and injury increasing the likelihood of remodelling and asthma/AHR. This would have occurred despite not breathing air-containing chloramines, PM or ozone, or simply very cold air. This rower's size was not unique. Of the 23 non-weight-classified rowers from 10 National Olympic Committees who were first approved for IBA use in Beijing and whose data were available, their average height was 194 cm (184 to 200 cm) and prechallenge FVC was 116% of that predicted (range 84% to 154%). These lung volumes were measured after withholding asthma medication before bronchial provocation testing. This resulted in several rowers demonstrating significant airways obstruction in their baseline spirometry.
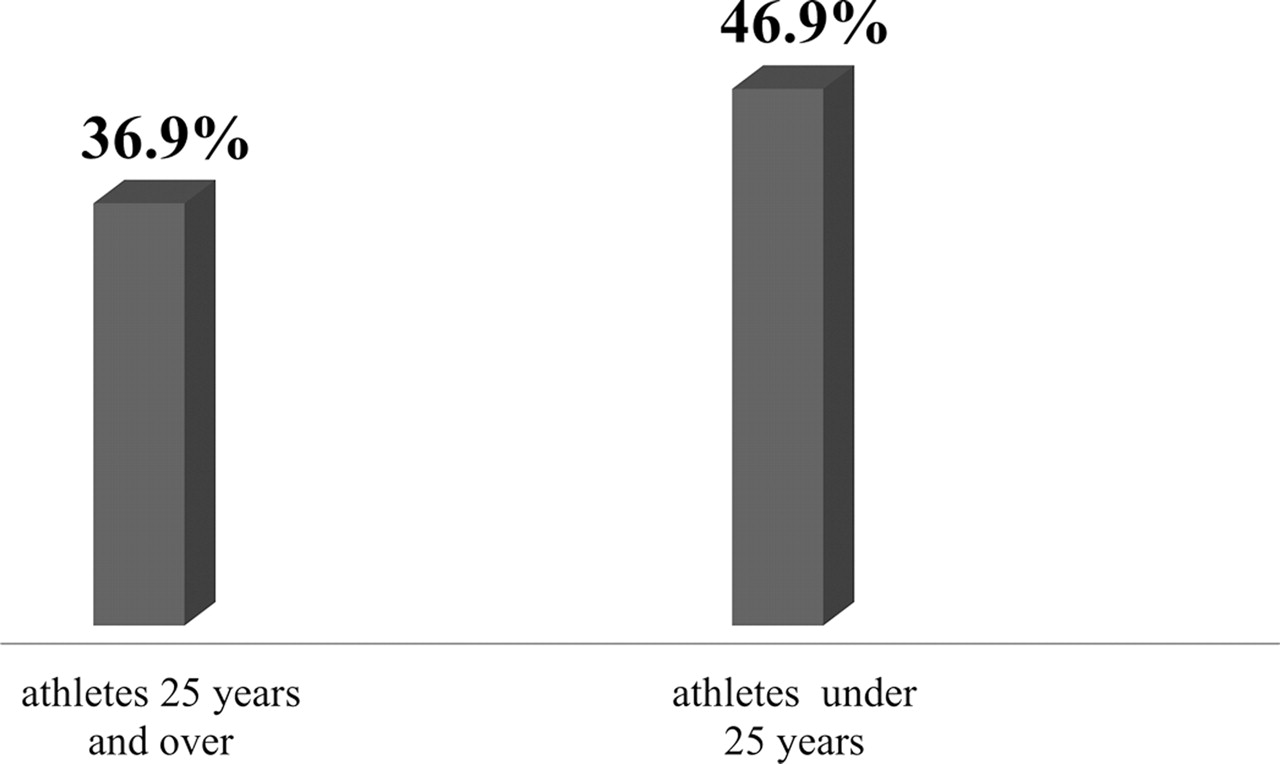
Beijing 2008 Older athletes develop asthma later – Sport induced? χ2 Significant at 0.01 level.
Olympic athletes with asthma/AHR have consistently outperformed their peers.
In Athens 2004, 4.2% of athletes were approved to use IBA and won 5.4% of the individual medals (figure 4). This unexpected outcome had been noted in Sydney 2000 when IBAs where merely notified. In Sydney, 5.7% of athletes notified IBA use but won 7.2% of the individual medals. It has been a consistent pattern over the past five Olympic Games.4 5 7

Olympic Games 2002 to 2010 – Percentage of athletes approved to use β2 adrenoceptor agonists and the percentage of individual medals won by them.
The marked dominance of asthmatic Winter athletes compared with their Summer counterparts is due predominately to the paucity of individual medals available in endurance Summer sports in contrast to Winter Games (figure 4). Six of the 22 Summer sports that award individual medals – boxing, gymnastics, weightlifting, judo, wrestling and shooting – are non-endurance sports yet provided 43% of the 679 individual medals won in Athens 2004.7 This contrasts to the Winter Games where endurance and non-endurance sports award about an equal number of individual medals. Partly because of this, for Beijing 2008, only two sports, swimming and cycling, were examined and a similar outcome was observed (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Beijing 2008 – percentage of swimmers and cyclists approved to use β2 adrenoceptor agonists and the percentage of individual medals these athletes won.
Why should athletes with asthma/AHR outperform their non-asthmatic rivals? As there is no evidence that IBA19 or ICS20 enhance performance, it is not due to treatment. Do the physiological changes associated with asthma represent a training stimulus that non-asthmatics do not experience?7 Genetic aspects may be a factor21 22 as to which athletes do or do not sustain damage to their airways by years of endurance training but research is necessary to determine if this theory is valid. Most accept the adage ‘the harder I train, the better I perform’. Is the reason that many athletes develop asthma/AHR in adult life because they train harder than many of their competitors and thus became more successful?
Finally, there is some evidence from retired Finnish swimmers that their AHR/asthma may be attenuated or disappear after ceasing years of endurance training.14 More research is necessary to determine if this is the likely outcome for many elite endurance-trained athletes.
Acknowledgments
The author thanks his colleagues on the IOC Independent Asthma Panel for their invaluable assistance; SD Anderson, DC McKenzie and M Sue-Chu since 2001, P Kippelen since 2004, R Crapo and H Magnussen (2002), C Gratziou (2004), C Gulotta (2006) and Lu Yong (2008).
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed