Article Text

Abstract
Athletes such as skaters and skiers inhale large volumes of cold air during exercise and shift from nasal to mouth breathing. Endurance athletes, like cross-country skiers, perform at 80% or more of their maximal oxygen consumption and have minute ventilations in excess of 100 l/min. Cold air is always dry, and endurance exercise results in loss of water and heat from the lower respiratory tract. In addition, athletes can be exposed to indoor and outdoor pollutants during the competitive season and during all-year training. Hyperpnoea with cold dry air represents a significant environmental stress to the airways. Winter athletes have a high prevalence of respiratory symptoms and airway hyper-responsiveness to methacholine and hyperpnoea. The acute effects of exercise in cold air are neutrophil influx as demonstrated in lavage fluid and airway epithelial damage as demonstrated by bronchoscopy. Upregulation of pro-inflammatory cytokines has been observed in horses. Chronic endurance training damages the epithelium of the small airways in mice. Airway inflammation has been observed on bronchoscopy of cross-country skiers and in dogs after a 1100-mile endurance race in Alaska. Neutrophilic and lymphocytic inflammation with remodelling is present in bronchial biopsies from skiers. Repeated peripheral airway hyperpnoea with dry air causes inflammation and remodelling in dogs. As it is currently unknown if these airway changes are reversible upon cessation of exposure, preventive measures to diminish exposure of the lower airways to cold air should be instituted by all winter sports athletes.
Statistics from Altmetric.com
Introduction
Air is inhaled primarily through the nose under sedentary conditions and is almost fully conditioned to body temperature and 100% relative humidity before it reaches the lower airways. During exercise, minute ventilation increases up to 30-fold from a resting level of 5 l/min, initially to meet the oxygen demands of the muscles and subsequently in response to the metabolic acidosis that develops during prolonged exercise. This is achieved through consecutive increases in tidal volume and respiratory frequency. When the minute ventilation exceeds 35 to 40 l/min, a shift from nasal to mouth breathing occurs,1 2 leading to incomplete conditioning and filtration of the inspired air. The task of conditioning the inspired air to body temperature and 100% relative humidity is completed by the lower airways.
Exposure
Winter sports athletes train on an all-year basis and are exposed to outdoor pollutants. Indoor athletes, such as figure and speed skaters and ice-hockey players, can also be exposed to pollutants from fossil-fuelled ice-resurfacing machines. They compete at temperatures between 4°C and 10°C. Outdoor athletes in endurance sports like cross-country and biathlon skiing are repeatedly exposed to subfreezing conditions on a daily basis during the competitive season. These athletes usually exercise twice daily for prolonged periods at 80% or more of their maximal oxygen consumption and have a minute ventilation in excess of 100 l/min.
Intra-airway temperature during exercise has not been measured in cold weather in human athletes. However, the effect of oral hyperventilation of 60 l air/min for 4 min has been investigated in healthy volunteers by McFadden, et al.3 Inhalation of air at −17°C and at room temperature reduces the intra-airway temperature in the anterior basal segment of the right lower lobe at end inspiration to 27.3°C and 31.3°C, respectively. A similar degree of airway cooling has been demonstrated in the sublobar bronchus of horses exposed to air at 5°C during treadmill exercise at intensities eliciting a cardiopulmonary response similar to that in human athletes.4
Cold air is always dry air
The relationship between the amount of water vapour in air at a given relative humidity and temperature is curvilinear. Air at 100% relative humidity and an ambient temperature of −10, 0 and +10°C has a water content of 3, 5 and 9 mg/l, respectively. In comparison, the water content at 100% humidity is 18 mg/ml at 20°C, and is 44 mg/l at 37°C, as in the alveoli. As cold air is always dry, the burden on the lower airways of conditioning the inspired air is greater for the winter than for the summer sports athlete. For example, in order to maintain 100% relative humidity, 34.6 mg water needs to be added per litre of air as it is warmed from 10°C to 37°C, compared with 26.7 mg/litre of air at an ambient temperature of 20°C. In addition, loss of heat and water during expiration is also greater in winter sports athletes. Water loss is proportional to the minute ventilation and has been estimated to be 32 mg/litre when exercising at temperatures below −16°C.5
Long-term effects
Knowledge about the long-term effects of cooling and drying of the lower airways following repeated and prolonged exposure to cold air in winter sports athletes is based primarily on cross-sectional studies. The prevalence of respiratory symptoms and airway hyper-responsiveness, together with the decline of lung function, has been investigated in human athletes. The effect of endurance training on the airways of the tracheobronchial tree has been investigated in human and animal athletes by bronchoscopy, endobronchial biopsy, induced sputum and bronchoalveolar lavage (BAL), and on the small airways has been limited to experimental animal studies. It is currently unknown whether the effects found in cross-sectional studies and described in this review are persistent. There are a few longitudinal studies in winter sports athletes, but these have been retrospective in nature and limited to studies of respiratory symptoms, airway responsiveness and pulmonary function.
Respiratory symptoms
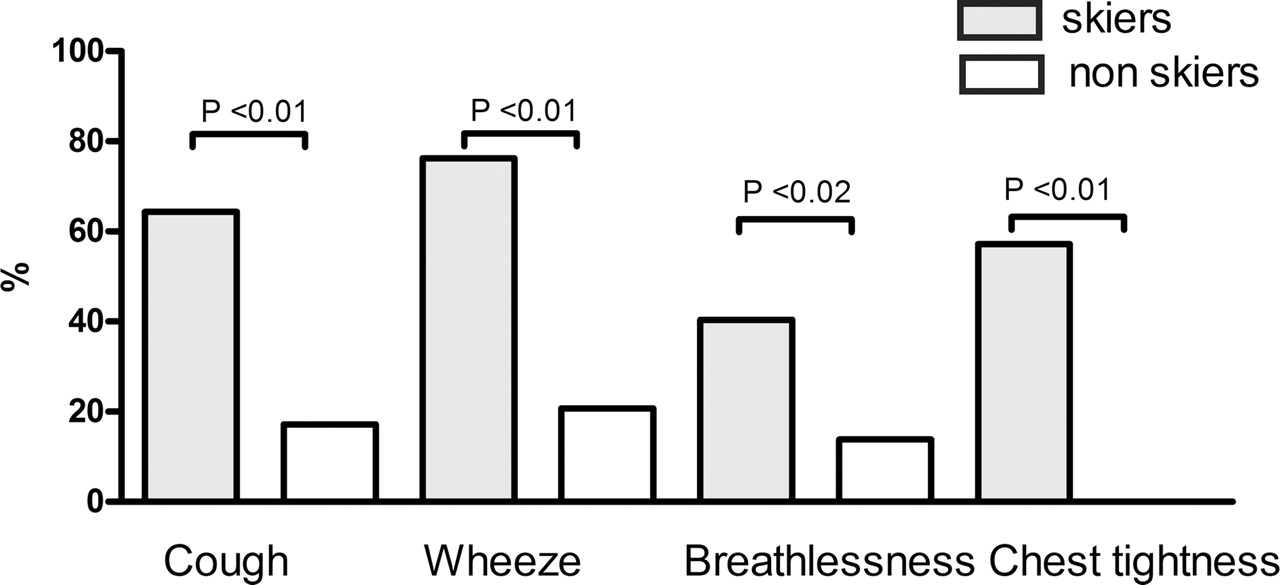
Widespread use of anti-asthmatic medication was observed at the 1991 world skiing championship. Cross-sectional studies subsequent to this observation6,–,8 reported a higher prevalence of cough, wheeze, breathlessness and chest tightness on exercise in cross-country skiers than in non-athletic controls (figure 1). Importantly, the onset of symptoms is primarily in late adolescence and early adulthood8 and the prevalence of respiratory symptoms is higher in the adult than in the adolescent skier,6 7 In one study by Larsson, et al6 50% of adult skiers had respiratory symptoms and airway hyper-responsiveness to methacholine and/or physician-diagnosed asthma. As airway hyper-responsiveness is also present in the winter and summer months, they suggested that strenuous training at low temperatures with the repeated inhalation of large amounts of cold air may be pathogenic factors for the development of asthma in athletes.
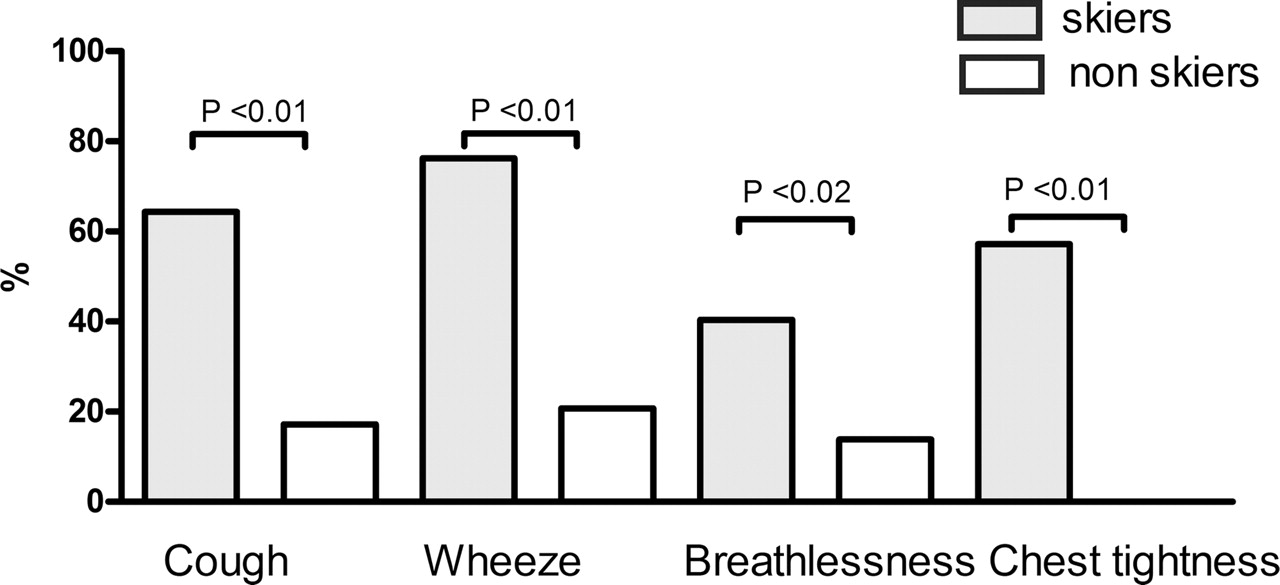
High prevalence of respiratory symptoms in elite adult cross-country skiers. Adapted from Larsson, et al.6
Airway hyper-responsiveness
In other cross-sectional studies, a lower prevalence of 18% to 35% of airway hyper-responsiveness to methacholine has been reported in skiers and other winter sports athletes, such as ice-hockey players and speed skaters.9,–,11 A similar prevalence of airway hyper-responsiveness to histamine has been reported in ice-hockey players.12 However, the prevalence of hyper-responsiveness to indirect stimuli, such as exercise challenge in the laboratory and in the field, eucapnic voluntary hyperventilation, dry powder mannitol and adenosine-5 monophosphate AMP, is even lower.10 11 13 Of these, the most sensitive stimuli are eucapnic voluntary hyperventilation and a sport-specific exercise test,13 14 with 21% to 35% of athletes testing positive to the latter stimulus in several studies.15,–,19
Airway hyper-responsiveness to any stimulus is, however, not always associated with respiratory symptoms in athletes. Airway hyper-responsiveness may be asymptomatic, and can be more prevalent to methacholine in asymptomatic than in symptomatic skiers.13 In another study, respiratory symptoms had a sensitivity of 50% for a positive sport-specific exercise challenge, which is no better than the result of tossing a coin.20
Lung function
There are only two studies of longitudinal changes in lung function in cold weather athletes. However, both studies had a retrospective design. In the first study, a decline in lung function over a 4-year period was observed in female elite ice hockey players, compared with a control group of female Nordic skiers.21 Lung function did not decline in the first 2 years of the study when training was on rinks resurfaced by electric-powered machines. The decline in lung function occurred in the third and fourth year while training on rinks resurfaced by fossil-fuelled machines. This was attributed to poorer air quality rather than to exposure to cold air.
The second study is a case report of three elite cross-country skiers with an accelerated decline in lung function, symptoms and objective evidence of airflow limitation during exercise at the end of an observation period of 9 to 12 years.22 Interestingly, airway responsiveness to methacholine improved in two skiers during the observation period.
Airway injury and inflammation
Studies in human elite athletes, as well as canine and equine athletes, suggest that repeated exposure to cold air may cause epithelial injury and mucosal inflammation in the proximal and distal airways. The proximal airways have been investigated by bronchoscopy with endobronchial biopsy and inducing and analysing sputum. The distal airways in human athletes have been investigated by BAL and experimentally at the sublobar level by dry air challenge in dogs and at the bronchiolar level by prolonged endurance training in mice.
Proximal airways
Inflammatory changes are seen on bronchoscopy of adolescent cross-country skiers who had a mean of 7 years of competitive skiing experience.23 There is an increase in vascularity and friability, defined as susceptibility to bleeding on contact with the tip of the bronchoscope, together with oedema and increased secretions (see commentary on the Blog, http://www.blogs.bmj.com/). The macroscopic inflammatory index compiled from these variables is significantly increased in skiers with respiratory symptoms and airway hyper-responsiveness to methacholine, compared with skiers without symptoms or hyper-responsiveness and healthy non-athletic controls.
Mucosal oedema is also evident on bronchoscopy of elite racing sled dogs performed at 24 to 48 h after completion of the Iditarod, a 1150-mile race in Alaska.24 These canine athletes are exposed to subfreezing conditions over 9 to 14 days. In addition, the endoscopic score, based on the degree of accumulation of intraluminal material, is significantly greater compared with control sled dogs that had trained throughout the winter but who were not exercised within the previous 2 weeks.
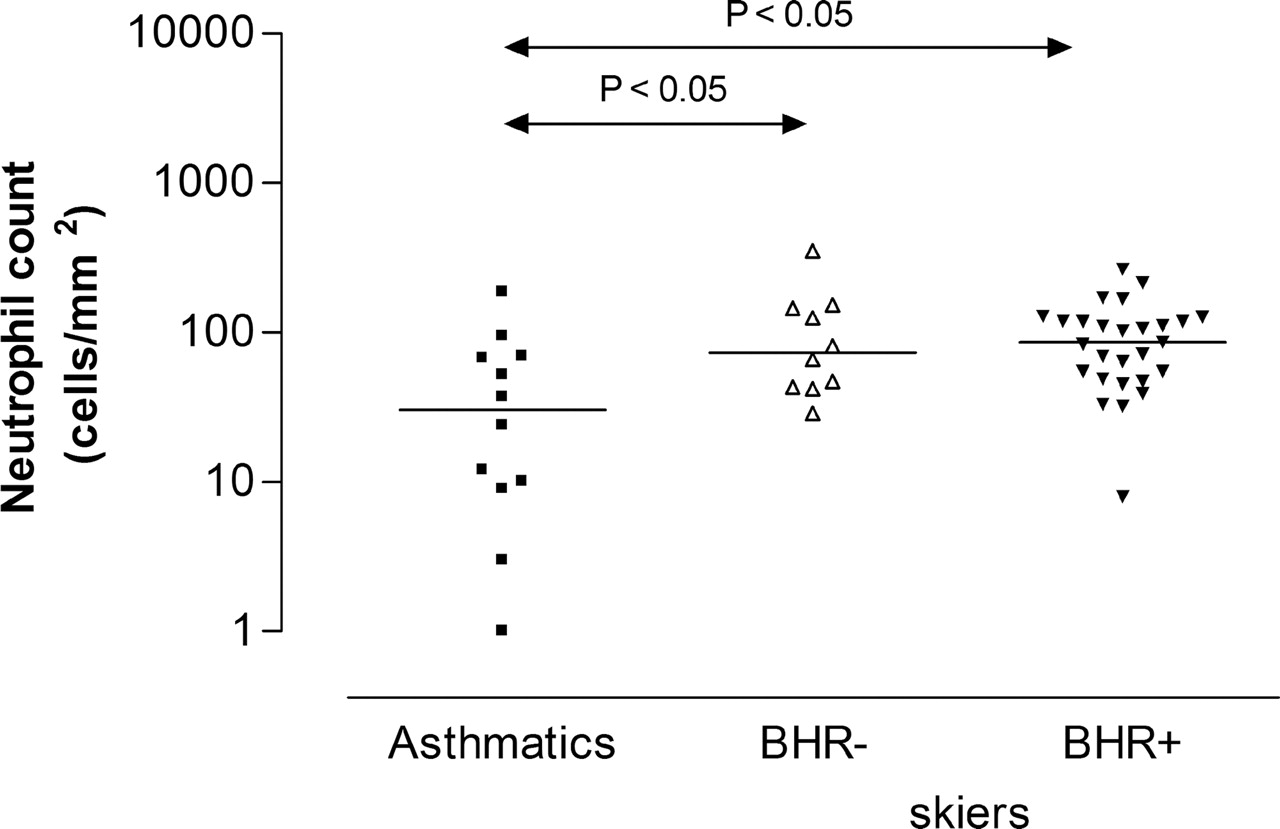
Inflammatory changes are also seen at a microscopic level. An inflammatory cellular infiltrate is present in endobronchial biopsies of the second-generation and third-generation carinae in adolescent cross-country skiers.25 Compared with non-asthmatic healthy controls, the submucosal infiltrate of Tlymphocytes, neutrophils, macrophages and eosinophils is significantly greater in skiers, with no significant difference in mast cell numbers. Lymphoid aggregates consisting of more than 50 cells are more than 2.5-fold greater in skiers.26 When compared with steroid naive mild asthmatic subjects, there are significant differences in the nature of the inflammatory infiltrate in these skiers. Neutrophil infiltration of the submucosa is more than twofold greater (figure 2), while eosinophil and mast cell infiltration are, respectively, fourfold and over twofold less in skiers. Moreover, inflammatory changes are present in skiers without respiratory symptoms or airway hyper-responsiveness to methacholine and are not associated with atopy. The nature of the inflammatory reaction in these athletes appears to differ from that in asthmatics.
{kind=link}
{kind=link}
Neutrophilic inflammation in submucosa of endobronchial biopsies of cross-country skiers and steroid -naive mild asthmatics. Higher median (horizontal bar) density of neutrophils in skiers with and without airway hyper-responsiveness to methacholine, compared to asthmatics. Reprinted with permission of the American Thoracic Society. Copyright 2011 American Thoracic Society. Karjalainen, et al25 Official Journal of the American Thoracic Society.
The inflammatory cell profile in induced sputum from adolescent ice-hockey players is similar to that observed in biopsy studies in skiers.12 It is predominantly neutrophilic in nature, but eosinophilic inflammation is present in 10% of these athletes. Like the skiers, neutrophil and eosinophil counts are not associated with either atopy or airway hyper-responsiveness to histamine.
In addition to an inflammatory infiltrate, there is evidence suggestive of remodelling.25 Expression of tenascin in the epithelial basement membrane is increased in skiers, compared with healthy controls. However, tenascin expression is not correlated with the inflammatory cell counts and is lower than that seen in mild asthmatics. The presence of tenascin is indicative of injury to the airways, as expression of this extracellular matrix protein after early childhood is associated with healing, repair and remodelling processes after injury.
Distal airways
An increase in minute ventilation leads to loss of heat and water from the small airways. The extent of involvement of these airways appears to be dependent on the temperature and water content of the inspired air. Mathematical modelling of heat and water flux at the end of 4 min of hyperventilation at 60 l/min under ambient conditions of 26.7°C and a water content of 8.8 mg/l has suggested that conditioning is complete by the 12th airway generation.27 However, Gilbert et al measured the intra-airway temperature after 4 min of exercise with inhalation of air at −17°C and at a lower minute ventilation of 42to 45 l/min and suggested that these conditions are present further down the airways at the 17th generation.28 Water loss leads to airway dehydration with an increase in the osmolarity of the airway lining fluid. In addition, non-laminar airflow due to the increased minute ventilation may also increase the shear stress to the distal airways, which together with dehydration may contribute to airway injury.
Airway injury, influx of inflammatory cells and remodelling occur after acute and chronic hyperpnoea. This has been documented by morphological and lavage studies in animal studies. In dogs, mucosal injury, bronchovascular leakage and infiltration of inflammatory cells occurs within 2 h of insufflation with dry air at 2 l/min for 5 min. A predominantly neutrophilic inflammatory cellular response is seen in the lavage fluid at 5 h after challenge, and repair of the damaged epithelium is evident at 24 h after exposure.29 30 In horses, exercise at 4°C results in an increased number of ciliated epithelial cells in the BAL fluid at 30 min after exposure.4 The effects on the distal airway appear to be influenced by the temperature of the inspired air. Compared with exercise at 25°C, the inflammatory response is greater after exercise at −5°C, with significant increases in the influx of neutrophils at 24 h and expression in pro-inflammatory cytokines, such as IL-1, IL-6 and IL-8 and tumour necrosis factor-α, and other cytokines such as IL-5 and IL-10 at 24 to 48 h in the BAL fluid.31
The effect of repeated exposure over a short time period has been investigated in dogs. Daily dry air insufflation of sublobar airways for 4 days causes epithelial injury and oedema of the submucosa, as well as influx of neutrophils and eosinophils and airway remodelling. Interestingly, the damaged epithelium is completely repaired with a return to normal airway morphology within 1 week after cessation of exposure. However, there is incomplete resolution of the inflammatory cell influx.32
The effect of repeated exposure over a longer period has been investigated in cross-country skiers and mice. In skiers, the inflammatory profile in the BAL fluid is different from that of healthy non-athletic controls. There are significant increases in total cell count and percentage counts of lymphocytes and mast cells. However, in contrast to findings in studies of acute exposure, neutrophil and eosinophil counts are not significantly increased. Inflammation in the distal airways may be present, as tumour necrosis factor-α and myeloperoxidase, a marker of neutrophil activation, are detectable in 40% and 20% of skiers, respectively.23 In mice, progressive damage to the bronchiolar epithelium is reported after 45 days of endurance training at low to moderate intensity at room temperature. The changes in mucosal morphology include a loss of ciliated cells and an increase in the thickness of the epithelium and apoptosis of epithelial cells. In addition, there is epithelial remodelling and infiltration of the airway walls and lumen with inflammatory cells without evidence of activation.33
At present, there are no studies in winter sports athletes that have investigated the effect of cessation of exposure on the kinetics of injury, repair, inflammation and resolution, as well as the cellular nature of the inflammatory response. However, a prospective longitudinal study in swimmers over 5 years suggests that cessation of swimming exercise of at least 3 months leads to a decrease in bronchial responsiveness, while eosinophilic inflammation in induced sputum increases in those swimmers who were still in active training.34
Conclusion
Winter sports athletes are repeatedly exposed to cold air. In addition to the low temperature, cold air is low in water content even when it is fully saturated with water vapour. Repeated, prolonged and chronic hyperpnoea with cold dry air represents a significant environmental stress to the proximal and distal airways, leading to the development of respiratory symptoms, airway hyper-responsiveness and injury, and inflammation and remodelling of the airway. Neutrophils and lymphocytes are the predominant inflammatory cells. As it is currently not known if these changes are reversible upon cessation of exposure, preventive measures to diminish the exposure of the lower airways to cold and dry air should be instituted by all winter sports athletes.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed.