Article Text

Abstract
Tennis is a popular sport with tens of millions of players participating worldwide. This popularity was one factor leading to the reappearance of tennis as a medal sport at the 1988 Summer Olympics in Seoul, South Korea. The volume of play, combined with the physical demands of the sports, can lead to injuries of the musculoskeletal system. Overall, injury incidence and prevalence in tennis has been reported in a number of investigations. The sport creates specific demands on the musculoskeletal system, with acute injuries, such as ankle sprains, being more frequent in the lower extremity while chronic overuse injuries, such as lateral epicondylitis, are more common in the upper extremity in the recreational player and shoulder pain more common in the high-level player. This review discusses the epidemiology of injuries frequently experienced in tennis players and examines some of these injuries' correlation with the development of osteoarthritis. In addition, player-specific factors, such as age, sex, volume of play, skill level, racquet properties and grip positions as well as the effect of playing surface on the incidence and prevalence of injury is reported. Finally, recommendations on standardisation of future epidemiological studies on tennis injuries are made in order to be able to more easily compare results of future investigations.
Statistics from Altmetric.com
Introduction
Tennis is truly a global sport, with tens of millions of yearly participants worldwide and over 200 nations having an association with the International Tennis Federation.1 This worldwide popularity led tennis to be reintroduced as a full medal sport beginning with the 1988 Summer Olympic Games in Seoul, South Korea. The sports was included in the inaugural Olympic Games in 1896 and continued to have participants in the Olympics through the 1924 competition in Paris, France. From 1924 through 1988, there were two demonstration years (1968 and 1984) but it did not receive full medal status until the sport's reintroduction in 1988. Beginning in 1988, men's and women's singles and doubles have been contested, with the additional appearance of mixed doubles beginning with the 2012 Games in London.2 3
Participation in tennis, especially at elite levels, places players at risk for musculoskeletal injury. There has been a wide variation in the overall reported incidence and prevalence of injury in tennis as there have been differences in the definition of injury, study populations, methods of data collection, and duration and/or frequency of follow-up between investigations. This review seeks to provide a comprehensive review of the epidemiology of injuries in the tennis player. Topics to be reviewed include the epidemiology of tennis-specific injuries as well as risk factors for sustaining injuries such as age, sex, volume of play, skill level, racquet grip and varying court surfaces.
Overall injury epidemiology
As methodologies and populations have varied between studies, the exact incidence and prevalence of injuries caused by tennis have been difficult to determine. In high-level players under 18 years of age, injury rates have been estimated to be anywhere from 2 to 20 injuries per 1000 h of tennis played.4,–,6 Pluim et al, in a comprehensive meta-analysis across all player levels, reported tennis-injury incidence as ranging from 0.04 to 3.0 injuries per 1000 h played.7 Some of the variation in these statistics invariably are the result of different definitions of injury used in the investigations. For example, in studies which defined tennis injuries as those requiring a trip to the emergency room, the rate of injury from tennis participation was extremely low.8 Other investigations, which have had more liberal definitions of injury to include any injury for which the player seeks medical assistance or treatment, have reported higher rates of injury.4 5
Injury location and chronicity
Injury due to participation in tennis may occur at any location in the musculoskeletal system (table 1). When the studies are viewed in aggregate, however, data show that most tennis injuries occur in the lower extremity (31%–67%), followed by the upper extremity (20%–49%) and lastly, the trunk (3%–21%).4 7 9,–,11 The most frequently injured parts of the lower extremity were the ankle and thigh, with ankle sprains being the most common specific injury. Upper extremity injuries most commonly involved the elbow and shoulder, with lateral epicondylitis being prevalent.12
Investigation details, overall injury incidence and injury by location across a variety epidemiological studies
Another trend which presents itself is that acute injuries commonly occur in the lower extremity while chronic injuries most often manifest themselves in the upper extremity and trunk.7 12 13 In a 6-year injury-surveillance study performed at the United States Tennis Association Boy's National Championship, the prevalence of injury was 21.1%, with the back being the most common anatomic site of injury (3.4%), followed by the thigh, shoulder and ankle.4 The rate of acute injures to the lower extremity, however, was nearly twice that of upper extremity and trunk, with acute ankle injuries demonstrating a prevalence of 2.4%. Another investigation of Swedish junior tennis players supported the findings of the previous study and found that over a 2-year period, ankle sprains were the most common acute injury while low back pain was the most common chronic complaint.14
Prevalence of specific tennis injuries
Tennis elbow
Lateral epicondylitis, or ‘tennis elbow’, is a tendinopathy involving the extensor carpi radialis brevis (ECRB) and is one of the most common overuse injuries in tennis, particularly in the recreational player.15 A recent large epidemiological investigation of 4783 Finnish tennis players of all levels found a prevalence of 1.3%, with no difference between men and women.16 In another investigation, Gruchow et al found a prevalence of 14.1% in over 500 tennis-playing subjects aged 20–50 years old.17 The overall incidence of lateral epicondylitis has been reported to be anywhere from 35% to 51% (table 2).12 16,–,18
Descriptions of studies reporting on epidemiology of lateral epicondylitis in tennis players
Although not proven in clinical investigations, some authors believe that the rate of lateral epicondylitis is lower in those with two-handed backhands as the non-dominant arm is able to absorb some of the forces associated with the stroke and using the second arm lessens the likelihood of faulty mechanics of the trailing and flexed wrist.19 20 One investigation examining the electromyographic (EMG) profile of the ECRB between single- and two-handed backhands, however, did not show any significant differences in activity.21 The use of vibration dampeners on the strings as well as grip size have also been proposed to have an effect on the development of lateral epicondylitis.15 Studies revealed, however, that there were no significant differences in vibration amplitude22 or discomfort ratings23 between players with dampened and non-dampened strings. Similarly, there was no difference in forearm muscle firing patterns when oversizing or undersizing the recommended size of the racquet grip by 6.25 mm (1/4 inch).24 As one investigation found that more experienced players had reduced forearm vibration25 and decreased EMG firing in the wrist extensors during the backhand stroke as compared with novice players,25 the development of lateral epicondylitis is likely more related to improper technique.
Shoulder
In one investigation, shoulder pain was reported to be present in 24% of high-level tennis players from ages 12 to 19 with the prevalence increasing to 50% for middle-aged participants.26 There have been a number of investigations which have reported the incidence and/or prevalence of shoulder pain within a larger group of study participants sustaining an injury from playing tennis.4 10 11 27 The percentage of tennis players at all levels with shoulder injuries in these studies ranged from 4% to 17%. Shoulder injuries are commonly due to repetitive use and may be related to scapular dyskinesis, rotator cuff pathology or glenohumeral internal rotation deficit with its resulting internal impingement and/or labral pathology.28 29 In general, shoulder symptoms in young, high-level tennis player are related to subtle instability while the rotator cuff is more commonly involved in the older player.30
Due to the high incidence of shoulder pathology in tennis players, some have questioned whether those participating in tennis are at increased risk of primary glenohumeral arthritis as they age. One investigation studied 18 senior tennis players with no history of shoulder surgery or trauma and compared them with age-matched controls.31 Results showed that 33% of the tennis players had radiographic signs of degenerative changes in the glenohumeral joint of their dominant arm versus only 11% of matched controls.
Hip
Injuries around the hip joint have been reported to account for between 1% and 27% of injuries in tennis players.4 10 12 27 Over a 6-year period, Hutchinson et al reported an incidence of 0.8 per 1000 athletic exposures and a prevalence of 1.3 hip injuries per 100 elite junior tennis players.4 Sanchis-Moysi et al investigated the size of iliopsoas and gluteal muscles in professional tennis players as well as professional soccer players with the use of MRI.32 They found that tennis players demonstrated an asymmetric hypertrophy of the iliopsoas and reversed the normal dominant-to-non-dominant balance observed in non-active controls while gluteal muscles are asymmetrically hypertrophied. As the iliopsoas can cause groin pain from tendonitis or bursitis,33 tennis players may be more susceptible to these pathologies in their non-dominant leg.
As with other joints, a positive correlation between previous athletic participation and hip arthritis in former elite athletes who have represented their country in international competition has been reported.34 35 One of the largest studies involving female ex-elite athletes who competed in running and tennis had up to a 250% increased prevalence of osteophytes around the hip joint as compared with controls.36 Furthermore, this same investigation reported that there was double the rate of osteophyte formation around the hip in tennis players when compared with runners.
Knee
Some investigations have examined the epidemiology of knee injuries in tennis players. A large epidemiologic study documented 17 397 athletes of all skill levels and ages with 19 530 sport injuries over a 10-year period. There were nearly 300 knee injuries related to tennis and of these, 11% had a confirmed anterior cruciate ligament (ACL) injury diagnosed in follow-up rather than on the tennis court at the time of injury.37 This same investigation reported that lateral collateral ligament and medial meniscus pathology were more frequent in tennis players as compared to other sports.37 Other studies have supported these findings and found that 10%–13% of athletes with knee injuries incurred ACL damage.27 38 Because of the high rate of ACL injuries across a wide variety of sports, significant research has been conducted to identify risk factors and develop prevention programmes for ACL injury.39,–,43 In addition to ACL injury, patellofemoral pain (particularly in females) and patellar tendonitis (‘jumper’s knee') have been reported to be common in tennis players.30 44
Increased risk of knee osteoarthritis has been found in athletes across many different sports.36 45,–,47 Clinicians and researchers had previously proposed that high-level activity which puts chronic repetitive stresses on the knee leads to degenerative changes. This thinking has been overturned, however, as others have shown that physical activity at a moderate level does not increase the risk of arthritis,48 49 and may in fact even decrease the risk.50 Thelin et al investigated the association between tennis participation and knee arthritis in over 150 Swedish male tennis players as well as athletes in other sports versus matched controls.51 They found that there was no significant correlation between tennis participation and knee arthritis after adjusting for confounding variables such as prior knee injury.
Tennis leg
‘Tennis leg’ involves the medial head of the gastrocnemius muscle.52 53 A large population of 720 athletes of all skill levels with ‘calf muscle strain’ studied over a 12-year period found that 16% of cases were due to tennis-related activities.54 Separate investigations have shown that calf and Achilles tendon strains represented anywhere from 4% to 9% of all tennis injuries reported.11 12
Back
Among active athletes, the prevalence of back pain has been reported to be up to 85%.55,–,58 In a case series of 148 professional tennis players, Marks et al found that 38% reported missing a tournament because of back pain and 29% suffered from chronic back pain.59 Another study found that 50% of elite tennis players suffered from back pain of at least 1-week duration, with 20% of these subjects having what they characterised as ‘severe’ pain.60 During a player's service game, the serve is the most commonly performed stroke during tennis competition.61 Hence, some have theorised that the repeated performance of the service motion may lead to back injury.62 Our laboratory investigations have shown significantly higher forces in the back for the kick (‘topspin’) serve versus the flat or slice serves, potentially leading to greater injury risk potential.63 64 We hypothesised that teaching the topspin serve at a young age may put the young tennis player at increased risk for back pain and/or injury. This early introduction of the topspin serve may be associated with the development of spondylolysis (stress fracture of the pars interarticularis of the spine) and/or spondylolisthesis in elite-level players.65
Given the common complaint of back pain in tennis players, studies have been undertaken to determine the prevalence of radiographic abnormalities of the back in tennis players. Alyas et al performed MRI on 33 asymptomatic adolescent elite-level tennis players and found that over 80% had abnormalities on MRI.65 Although pathology in the structures of the back is known to exist in tennis players, the most common cause of back pain is related to lumbar strain rather than direct spinal pathology.30 Furthermore, tennis players have not been found to be at increased risk of back pain as compared with non athletes. From the interviews of spectators at an international tennis competition, it was inferred that there were no significant differences in the prevalence of back pain between tennis players and non-tennis players.66 67
Stress fractures
A recent study of stress fractures in tennis players carried out by Maquirriain et al followed a cohort of 139 elite tennis players over a 2-year time period.68 They found an incidence of almost 13%, with the tarsal navicular being the most commonly affected (27%), followed by the pars interarticularis (16%), the metatarsals (16%) and the tibia (11%). Those under 18 years of age were more affected as compared to adults. In the upper extremity, Balius reported a case series of seven metacarpal stress fractures in high-level junior tennis players.69 All stress fractures were located in the second metacarpal with the exception of one which was located in the third metacarpal. They found an association with playing intensity and theorised that the western or semiwestern grip may also be an additional risk factor. Less common areas of stress fractures in tennis players that have been reported in the literature, mostly as case reports, have been the ischium,70 first rib,71 humerus,72 73 sacrum,74 patella,75 hook of hamate,76 ulna77,–,80 and distal radius.81
Player-specific risk factors
Age and sex
The effect of age on injury was studied by Jayanthi et al and there was no significant correlation for tennis players across a variety of skill levels.9 When examining investigations which reported on differences in rate of injury between men and women in tennis, the literature is fairly clear that there are no significant differences. In a study of nearly 4000 collegiate athletes who sustained 1800 athletic injuries over a 15-year period, there were no significant differences in the overall injury rate between males and females.10 This finding did not change when the tennis players were broken out into a subgroup analysis. Other investigations have supported these findings.9 11
Volume of play
Current literature suggests that volume of play is positively correlated with an increased injury rate. One investigation found an overall increase in injury rate for those who participated in tennis more than 3 h per week.12 For specific tennis injuries, two separate investigations have examined the correlation between volume of play and the development of lateral epicondylitis. Kitai et al found that the average amount of play for amateur tennis players with symptoms of lateral epicondylitis was 8 h per week while those who did not have elbow pain played an average of 5.5 h per week.82 Gruchow et al reported that recreational players who participated in tennis greater than 2 h per day reported more frequent elbow pain than those playing less than 2 h per day.17
Skill level
To our knowledge, only one study published in the English literature has examined the association between risk of tennis injury and skill level. Jayanthi et al investigated the incidence and prevalence of injuries sustained during tennis and used skill level to stratify the results.9 This study did not find any significant differences in rate of injury for multiple comparisons across a variety of skill levels.
While overall incidence and prevalence of injury may not differ between skill levels, less experienced players may subject themselves to larger stresses, therefore raising their risk of injury. The influence of skill level on the magnitude of vibration at the wrist and elbow during the backhand stroke has been studied.25 The authors found that compared with more proficient players, less experienced players were subjected to higher vibration loads in the elbow and wrist during stroke production. Another investigation by Wei et al confirmed these findings by finding that experienced players were able to reduce the racquet vibration impact to the elbow joint by 89% during the backhand stroke while novice players reduced impact by only 62%.83 Reasons for this may include novice players having more variability in the contact point of the ball upon the strings84 as well as differences in grip forces between the two populations. Hennig et al has stated that reduced grip forces allow for decreased vibration translation from the racquet to the arm, potentially leading to fewer injuries to the upper extremity.25 84 Although professional tennis players have improved technique and therefore a theoretically decreased risk of injury, their increased volume of play as compared with the non-professional may account for the similarity in injury rates between the two groups.
Racquet grip position
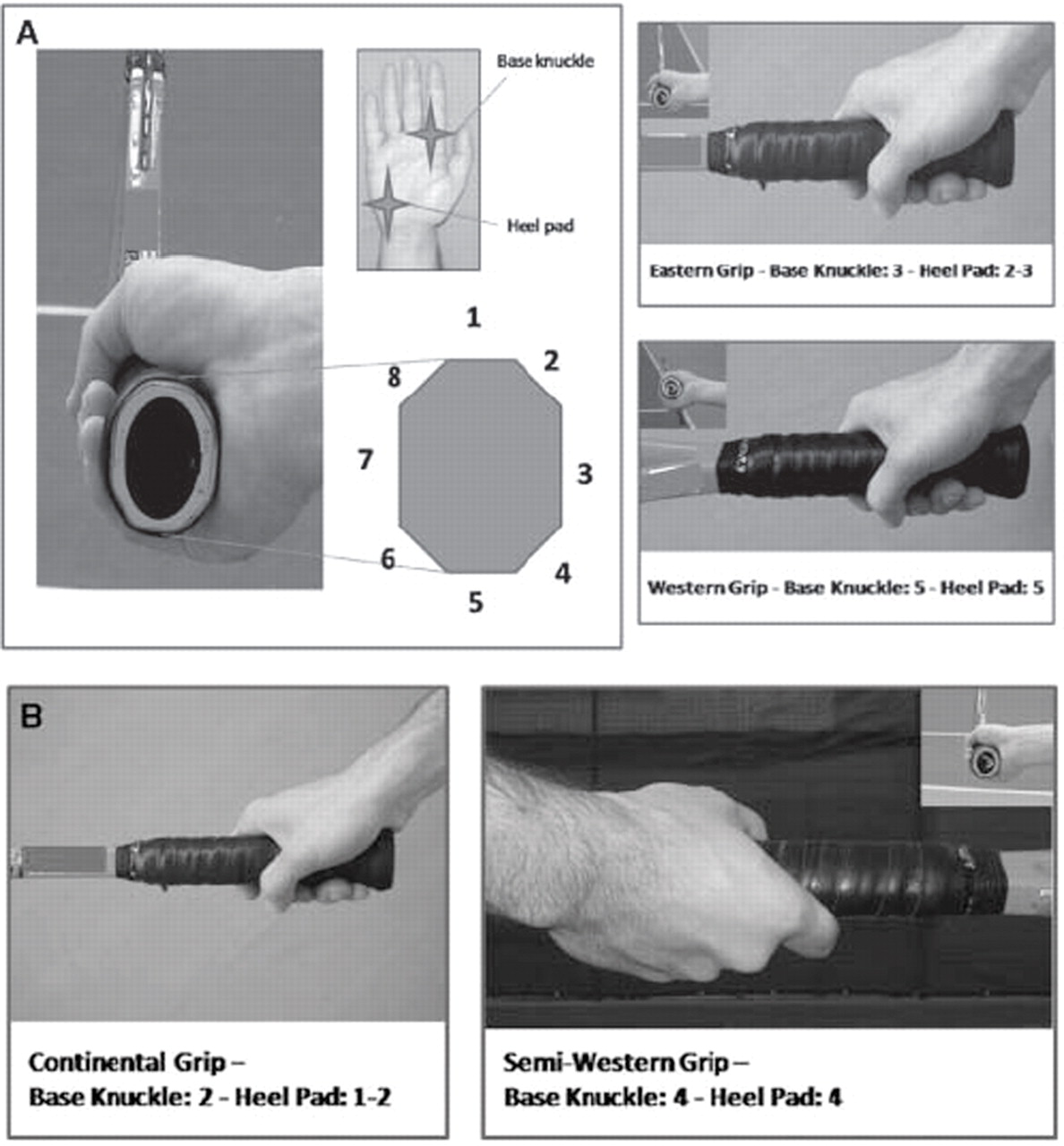
Different grip positions may affect stroke biomechanics and overall biomechanical loads transmitted to the upper extremity. Classically, there have been four different grip positions used to hit the forehand: continental, eastern, semiwestern and full western. The continental grip places the second knuckle on level 1 of the grip while a full western grip has the second knuckle placed at the bottom face of the grip (figure 1A,B).85 To investigate the effect of grip type on injury to the wrist, Tagliafico et al studied 370 non-professional tennis players.86 They found that ulnar-sided injuries (extensor carpi ulnaris tendonitis and triangular fibrocartilage complex pathology) were significantly associated with western or semiwestern grips while radial-sided injuries (flexor carpi radialis tendonitis, DeQuervian's tendinopathy and intersection syndrome) were more common in players with the eastern grip.86
{kind=link}
(A) On the left side the eight facets of the butt cap and the reference points (base knuckle of the index finger and heel pad) on the hand to identify the different grips are represented. On the right side, the eastern and western grips are shown; note that the hand of the players is in the same position while the inclination of the racket changes. (B) The continental and the semiwestern grips are illustrated (images used with permission.92)
Racquet properties
Racquet mechanical characteristics themselves also have the ability to change vibration loads transmitted to the arm during the performance of tennis strokes. Hennig et al showed that between different racket properties, increased racket head size as well as a higher resonance frequency of the racket were found to reduce arm vibration. There have been no studies, however, to determine the effect of arm vibration on injury rate or severity.25
Court surface
A number of studies have examined the relationship between court surface and injury in tennis players. A retrospective review of data from 1978 to 2005 was undertaken to identify incomplete matches in Grand Slam tournaments, indicating that one of the players was forced to retire due to injury.87 The authors found that the fewest incomplete matches occurred on grass while there was a higher number of incomplete matches for women on Australian hardcourts and on USA hardcourts for men. Bastholt recorded the number of players on the Association of Tennis Professionals (ATP) tour who sought medical treatments at various tournaments over a 3-year period.88 The RR of receiving treatment while playing on hard court as compared with grass was 0.8 (grass had a higher risk) while the RR between hard court and clay was 2.3 times (hard court had a higher risk). In contrast to the study in Grand Slam tournaments, this investigation found that playing on grass or hard court incurred a greater risk of seeking medical treatment as compared with clay. In a review of tennis injuries, Kulund et al reported fewer knee problems in senior tennis players who had spent their career on clay courts as compared with hard courts,89 with another investigation also suggesting that the risk of injury is lower on clay courts.90
Future directions
It is clear from the review of the literature that further study on the epidemiology of injuries in tennis is needed. Differences in the definition of injury, study populations, methods of data collection and duration and/or frequency of follow-up between investigations make comparisons between studies difficult. In the future, adherence to previously published guidelines on epidemiological studies of medical conditions in tennis91 may allow more indepth comparisons should a critical mass of data be collected using these standardisation guidelines. Furthermore, when looking at the epidemiological literature for tennis injuries, there are surprisingly few studies on professional tennis players. Some of the investigations which have included professionals were included in this review,32 59 87 88 but most published studies have focused on either ‘high-level’ or ‘elite’ tennis players. In the future, additional studies on professional/Olympic level players would provide better insight and knowledge on the specific types of injuries these players sustain.
Conclusion
This article has reported on the overall incidence and prevalence of injury in tennis players as well as the rates of injury for more tennis-specific pathologies. The general trends which emerge from this review are that acute injuries are more common in the lower extremity while chronic and overuse injuries are more common in the upper extremity and trunk. Furthermore, there is no association between age, sex and skill level on injury rate in tennis players. Volume of play, however, is clearly associated with an increased risk of injury. Factors for which the literature is mixed include the association between tennis participation and long-term arthritis in joints other than the knee as well as the effect of court surface, racquet grip and racquet properties on the rate of injury.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.