Article Text

Abstract
Objective To assess the injury incidence in elite handball, and if gender and previous injuries are risk factors for new injuries.
Methods Cohort study of 517 male and female elite handball players (age groups under (u)16, u-18 and senior). Participants completed a web survey establishing injury history, demographic information and sports experience, and provided weekly reports of time-loss injuries and handball exposure for 31 weeks by short message service text messaging (SMS). Injuries were further classified by telephone interview.
Results The weekly response rate ranged from 85% to 90% illustrating the promise of the SMS system as a tool in injury surveillance. Of 448 reported injuries, 165 injuries (37%) were overuse injuries and 283 (63%) traumatic injuries. Knee (19%) and ankle (29%) were the most common traumatic injuries. The injury incidence during match play was 23.5 (95% CI 17.8 to 30.4), 15.1 (95% CI 9.7 to 22.2), 11.1 (95% CI 7.0 to 16.6) injuries per 1000 match hours among senior, u-18 and u-16 players, respectively. U-18 male players had an overall 1.76 (95% CI 1.10 to 2.80) times higher risk of injury compared to females. Having had two or more previous injuries causing absence from handball for more than 4 weeks increased the risk of new injury in the u-16 group (IRR: 1.79 (95% CI 1.03 to 3.11)–2.23 (95% CI 1.22 to 4.10)).
Conclusion The incidence of time-loss injuries in elite handball was higher during match play than previously reported in recreational handball. Previous injuries were a risk factor for new injuries among u-16 players. Male players had a significant higher injury rate in the u-18 group.
Statistics from Altmetric.com
Background
Team handball or handball, was first played at the end of the 19th century, and introduced in the Olympics in 1936.1 Today, handball is one of the most popular sports in Europe, played by men, women and children of all ages. Playing handball is also associated with a high risk of injuries.2,–,12 Studies have shown that time-loss injury rates range between 8.3 and 14.3 injuries per 1000 match hours and 0.6–4.6 injuries per 1000 training hours among recreational handball players with slight differences between youth and senior players.4 8,–,12 Prevention of these injuries is therefore an important task for everybody around the athlete.
An important first step in developing effective injury-prevention strategies is to determine the burden of injury through injury incidence and severity.13 Variability in injury definitions, inconsistencies in injury-reporting methods, and poor study designs in previous investigations in handball may negatively impact the internal and external validity of the research available, thus making direct comparisons between studies difficult. In a recent study, Nilstad et al,14 evaluated an new method in which female soccer players employed short message service text messages (SMS messages) to record injuries rather than routine injury registration by team medical staff. The study showed that the reports from the medical staff underestimated the incidence of time-loss injuries by two-thirds, which emphasises the importance of athlete-versus medical staff-based registration to increase the accuracy of recorded injury incidence rates in team sports.
Studies investigating injuries in handball have focused on the recreational handball with limited research in the elite population and there have been no studies investigating injuries in handball by athlete-based registration. This study aimed to assess the injury incidence among both youth and adult elite handball players in Denmark by pioneering the use of the SMS system that made it possible for the athletes themselves to report injuries directly, and to examine if gender and previous injuries are risk factors for new injuries.
Material and methods
Study design
A 31-week prospective cohort study was conducted during the Danish 2010/2011 handball season (September 2010–April 2011), including elite handball players in the u-16, u-18 and senior elite age groups. Danish Data Protection Agency and The National Committee on Health Research Ethics in Denmark approved the study.
Population
First, seven out of 12–14 possible teams for each age group and each gender were randomly selected for direct invitation sent by e-mail to the club and/or coach. All the players from the accepting teams received additional written and oral information about the study, and signed a consent form including their phone number and e-mail. Second, information about the study including a direct link to a web-based questionnaire was posted on one major handball website (www.europamester.dk), on Facebook, and by e-mails routed to players by the Danish Handball Players' Association. The recruiting period started in August 2010 and the players could enter the study as late as December 2010.
Data collection
Population
All of the players were asked to complete a 15-min questionnaire via web-invitations or e-mail. This established their injury history, demographic information (eg, age, height, weight, player position), sports participation experience including hours per week spent on injury prevention and weight training, and whether the players attended the national team at study start (table 1).
Operational definitions used in the study
Prospective registration of injuries and exposure hours by SMS messages
All participants provided weekly reports of injuries, match and training exposures using the SMS system. The primary outcome was any handball-related injury (table 1). Every Sunday evening all participants received the following three SMS messages:
(1) Have you had any injury or illness that has restricted you partly or fully from participation in one or more training sessions and/or matches the last week? Answer ‘no’ (=0), or ‘yes’ (=1), or ‘yes, but due to the same reason as last week’ (=2).
Illness was originally included in the question as a secondary outcome, but this was not included in the purpose of this article.
(2) How many minutes of match play did you do the last week? Sum up all matches and report the total number of minutes played.
(3) How many hours of training did you do the last week? Sum up your total hours of handball training, rounding up to nearest full hour.
If a participant did not answer the SMS, he/she received a reminder SMS 48 h and 96 h after receiving the first SMS.
The following week, three bachelor students, with no clinical background or particular interest in handball, contacted players who had reported an injury via telephone, to complete a 5-min structured interview (table 2). To ensure the standardisation of the interview, the bachelor students were instructed how to perform the interview before study start. Players who could not be reached the following week were contacted up to 4 weeks after they have reported the injury. If still not reached by phone, the injury was categorised as ‘non-classified’.
Data collected through the standardised injury classification form
If a player sought medical attention, the club's physiotherapist was contacted to include her/his or the clinician's diagnosis of the injury in study data. Exposure hours were calculated based on the answers to questions 2 and 3. Injury severity was measured by the number of weeks the player reported having the same injury as the previous week (question 1), and was divided into two groups, total absence and partial absence from handball activities (table 1). Severity of less than 1 week in length was established through the aforementioned telephone interviews.
Data analyses
Injury incidence was calculated as the number of injuries during the study divided by the sum of exposure hours expressed in 1000 h of match, training or total exposure time (match and training). All reported illnesses and missing values in injury and exposure hours in the SMS system were excluded from the analyses. Furthermore, injuries with zero in the corresponding time of risk were excluded to be able to perform calculations of incidence rates, but included when presenting the prevalence and severity. Weekly prevalence was expressed as the sum of new injuries and the reported same injuries as last week (question 1) divided by the number of participants answering that week. These analyses were based on all participants included in the study, regardless of whether or not they had completed the baseline questionnaire.
Poisson regression using robust standard errors and taking into account the cluster nature of the study was used to estimate incidence rate ratios (IRR) with gender and previous injuries as primary risk factors. All the listed baseline co-variates (table 3) were assessed as potential confounders or effect modifier, and the analyses of risk factors were adjusted for the identified potential confounders, which was participation on the national team, body mass index (BMI) and hours per week spent on injury prevention. All analyses were based on the injuries that were successfully classified through the telephone interview. Non-classified injuries were not excluded from the analysis, but included as no injury, and therefore still contributed with exposure time. STATA Intercooled version 11.2 was used for the statistical analyses, and all statistical hypotheses were tested with a significance level of 5%.
Baseline characteristics of 342 elite handball players by age group and gender
Results
Population
Of the 530 players who accepted to participate in the study, 499 were recruited through direct invitation. A total of two women's teams in each age group declined or did not respond to the invitation. Two male senior teams, three male u-18 teams and four male u-16 teams declined or did not respond. Of the 530 players, 13 players, all from the web invitation, were excluded because they had ended their career or played at a lower level. The remaining 517 players in the age groups u-16 (n=194), u-18 (n=152) and senior (n=171) were included in calculations of incidence rates. The final study sample represented 52 clubs; with the majority of the population – 387 players – representing nine directy invited clubs from all regions in Denmark. The questionnaire on baseline characteristics was completed by 342 (66%) players (table 3), and only this part of the population was included in the analyses of the hypotheses.
Prospective registration of injuries by SMS text messaging
The weekly response rate to all three SMS messages ranged between 85% and 90% during the 31-week study period. When illnesses were weeded out, a total of 754 registrations remained in the SMS system, of which 529 were classified as injuries (70%). Of the 517 participating players, 306 (60%) sustained at least one injury.
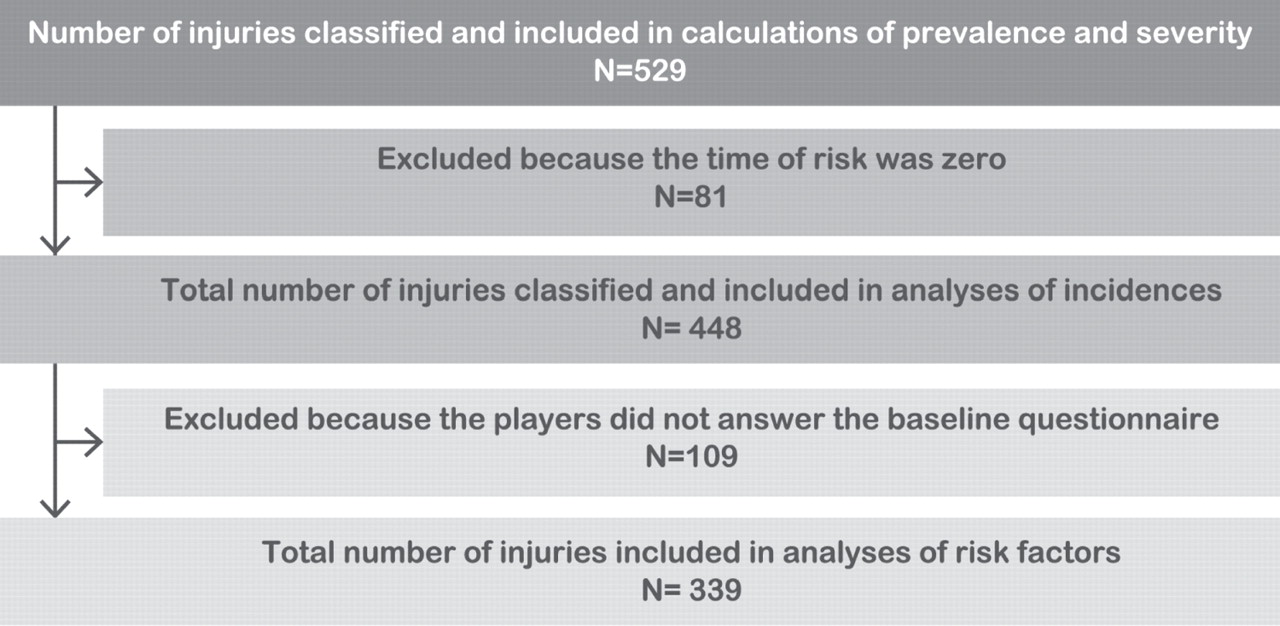
Figure 1 illustrates how injuries were included in the analyses of prevalence, severity, injury incidence and of the hypotheses.

{kind=link}
Inclusion-flow of injuries in analyses of incidence rates and of risk factors with total exposure hours (match and training) as the time of risk.
Injury incidence
Four hundred and fourty-eight injuries were sustained in 71 014 exposure hours, resulting in an overall injury incidence of 6.3 per 1000 match and training hours (95% CI 5.7 to 6.9). Overall, the study shows that reported injury incidence falls with age (table 4).
Injury incidence and unadjusted relative risk estimates in 517 elite handball players by age group and gender
Injury pattern
Of the 448 injuries, 165 injuries (37%) were classified as overuse injuries and 283 (63%) as traumatic injuries (table 5), and 366 (82%) were confirmed and diagnosed by a physiotherapist or a physician. Acute injuries ranged from sprains/distortion (46%) to muscle strains (17%) and contusions (9%). Shin splints (22%) were the most common overuse injuries, accounting for 35 of the 39 reported lower leg injuries, followed by tendinopathy (22%) and bursitis (7%).
Number of injuries and injury incidence in 517 elite handball players by age group, injury type and body region
The majority of the injuries were new injuries (65%), and 35% were recurrent injuries, of which 40% were classified as early recurrence (within 0–2 months), 29% as late recurrence (2–12 months) and 31% as delayed recurrence (>12 months). Approximately half of the injuries caused absence from handball activities more than 1 week, of these 10% caused total absence from handball activities more than one week (table 6). The weekly mean injury prevalence was 21.4% (range 17.8–25.6).
Severity of 529 classified injuries according to absence in days from matches or training sessions during the study period
The risk of injury by baseline data
There was a significant difference in the classified injury incidence between players answering the baseline questionnaire (injury incidence 7.1 (95% CI 6.4 to 7.9) based on 339 injuries during 47 693 exposure hours) and players not answering the baseline questionnaire (injury incidence 4.7 (95% CI 3.8 to 5.6) based on 109 injuries and 23 321 exposure hours). Injury rates and IRR associated with baseline characteristics are summarised in table 7.
Multivariate incidence rate ratio estimates by baseline covariates and by age group adjusted for all included covariates
Discussion
Prospective registration of injuries by SMS text messaging and injury incidence
This study is the first of its kind in elite handball to capture all injury and exposure data using a SMS system of self-report. The weekly response rate of 85%–90% illustrates the promise of the SMS system as an effective data-collection tool in injury-surveillance studies. Compared to previously used registration methods, the SMS system limits the risk of recall bias and facilitates more accurate exposure time, which allows us to obtain more accurate injury estimates. This might be the reason why, this investigation lead to a higher match injury incidence than reported in previous injury-surveillance studies focusing on time-loss injuries, but the reported incidences of training injuries and total incidence, based on both training and matches, were consistent with previously published reports in recreational handball for all age groups.
For senior players, the estimated match injury incidence was 23.5 per 1000 match hours (95% CI 17.8 to 30.4), which is more than twice that reported by Nielsen et al.4 Senior male players had an estimated incidence of 31.7 per 1000 match hours (95% CI 22.0 to 45.0), which is nearly three times greater than the rates reported in previous studies.8 9 In the u-18 group, the incidence of match injuries was 17.2 per 1000 match hours for males (95% CI 9.3 to 28.8), 13.0 per 1000 match hours for females (95% CI 6.5 to 23.3). These rates were also greater than those in the study by Olsen et al.10 For u-16 players, the estimated incidence of match injuries was 11.1 per 1000 match hours (95% CI 7.0 to 16.6). No previous studies have reported the incidence of time-loss injuries in this age group. Wedderkopp et al studies in 19976 and 19997 included all injuries, not just time-loss injuries, and have to date reported the highest match injury incidence among recreational female youth players, 41 injuries per 1000 match hours and 23 injuries per 1000 match hours. Their results indicate that the injury incidences we have reported in this study might be underestimated, because of the time-loss definition we employed. Fuller15 argues that a large percentage of elite players continue to play with modification rather than stopping; as a result, particular overuse injuries might not be captured.
Our results might be further underestimated by the fact that pool of data on reported injury rates was reduced as many injuries had to be excluded because respondents either did not report or made errors in their calculations of exposure time. While the weekly SMS response rate was high, we experienced difficulties in reaching the participants by telephone. As a result, only 70% of the injuries reported through the SMS system were classified. As the incidence of match and training injuries were based solely on traumatic injuries classified, the reported incidence in this study might be underestimated by up to 30%. This study is also limited by the difficulty we had obtaining validated injury reports from the physiotherapist, which gives a risk of information bias and in future studies, we recommend having all reported injuries evaluated and/or assessed by medical personnel assigned to the study.
Injury patterns
In this study, overuse injuries accounted for 31%, 36% and 45% of all injuries among the senior, U-18 and U-16 players, respectively. Previous studies have reported that 7%–21% of injuries to young handball players were overuse injuries.6 7 10 This indicates that the SMS method is better to capture overuse injuries than the methods used in previous studies. We divided the severity of the injuries into full absence from handball activities and partial absence: this shows that a large percentage of the players continue to play, rather than stopping completely, and that traumatic injuries are more likely to cause full absence from handball activities than overuse injuries.
The most commonly reported traumatic injury locations were the ankle and the knee, 29% and 19%, respectively. Wedderkopp et al6 presented similar findings, but Olsen et al10 and Seil et al9 reported that the number of acute knee and ankle injuries were similar.
The risk of injury
Gender was only a significant risk factor in the u-18 group, in which boys had a 1.75 (95% CI 1.10 to 2.80) times greater risk of injury than girls. Previous studies have shown that women have up to five times higher risk for an anterior cruciate ligament injury compared to men.17 We did not observe any differences in injury location between genders, but this might be due to the relatively small sample size.
Previous injuries were only a risk factor in the U-16 group in particular if the player had sustained two or more previous injuries. Wedderkopp et al6 found a much higher relationship between previous injuries and new injuries. This difference may be related to the differences in injury definition between the two studies. In this study, previous injuries were included in the analyses as one variable combining injuries of all types and locations as one, which might be ‘diluting’ the effect of previous injuries as a risk factor, for example, a shoulder injury is very rarely a risk factor of a knee injury. To perform subanalyses for each injury where the researchers has to take the type and location of previous injuries into account, a very large number of participants are needed, as there will only be enough of the most common type of injuries to perform analyses with previous injuries as a covariate.
The lack of ‘non-classified injuries’, which were included in the analyses as no injuries and therefore still contributed with exposure time, may have affected the estimated IRR. To illustrate that, we performed a sensitivity analysis in which all registrations (classified and not classified) from the SMS system were included as injuries. In this analysis, previous injuries and gender were not significant risk factors in any of the age groups. This emphasises the importance of getting all injuries classified, especially in this case where it is uncertain if the non-classified registrations might be because of illness or an injury.
All collected data on risk factors was based on self-reporting, which is limitation in this study and in all other studies assessing the association between previous injuries and new injuries, because of the risk of recall bias. In this study, a previous injury could only qualify as such if it resulted in time loss of 4 weeks or more, which is a serious injury, we believe, a player will remember. BMI and hours spent on injury prevention, which was included as confounders, may be biased, because players tend to underestimate their weight by self-report, and it is possible that the players have overestimated the hours they spent on injury prevention.
The analyses of risk factors were based only on the 66% of the population who answered the questionnaire, leading to a risk of selection bias. No difference was found in comparing responders and the non-responders with respect to gender or age group, but the questionnaire responders had a higher injury incidence than non-responders, leading us to conclude that the responders were also the ones with (more) previous injuries, which might lead to an underestimation of the IRR of the previous injuries.
The study population was invited by two approaches, invitation via clubs and through the Internet. We cannot rule out the possibility that those who signed up on the web had previously had injuries and thus were more interested in participating. However, given the limited number of participants who actually joined the study through the web, we assume that this did not affect the results.
Conclusion
The injury incidence of time-loss injuries among elite handball players is higher during match play than previously reported in recreational handball, however, it might be due to the new SMS method implied as registration method in this study. A history of more than two previous injuries is associated with an increased risk of new injuries among u-16 Danish handball players. Male players had a significant higher injury rate in the u-18 group.
Perspectives
The SMS system is a promising tool in injury surveillance, but it needs to be optimised for other large-scale studies so all of the reported injuries get classified and validated by the medical staff. Ankle and knee injuries were the most common traumatic injuries. Previous studies have shown that it is possible to prevent more than 50% of these injuries.7 11 18 This study indicates, unfortunately, that prevention programs have not yet been effectively implemented in Danish elite handball clubs. Accordingly, a future challenge is to implement prevention programs proven effective to the coaches and athletes in sports by developing and evaluating strategic implementation plans designed to address key barriers and facilitators towards intervention uptake across all levels, as argued by Finch.13
Knowledge of prevention programs is not enough; it must be used.
Acknowledgments
The authors are grateful to all the players and physiotherapists who participated in this study, without which this study would have been impossible, and thank PhD student Tracy Blake, Sport Injury Prevention Research Centre, Calgary, for her assistance editing the vocabulary.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study was approved by the Danish Data Protection Agency and The National Committee on Health Research Ethics in Denmark.
-
Provenance and peer review not commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous
- Miscellaneous