Article Text

Statistics from Altmetric.com
Introduction
Catastrophic neck injuries in rugby are rare1 but devastating, and they continue to occur in a sporadic fashion with cohorts of cases reported by clinicians confronted by a peak in presentation.2,–,5 This pattern has been repeated since the 1970s when the problem first became evident.
This review was prompted by a recent increase in schoolboy admissions to the Scottish national spinal injuries unit in Glasgow.6 The aim of this study was to obtain comparative data for players aged under 19 years in Great Britain and Ireland, an exercise which has not previously been undertaken. The intention was to include cases since 1996 which was possible in Scotland and Ireland, but was not possible for England and Wales where records could be traced only from 2000.
The lack of a complete data set for spinal cord injuries in rugby, despite repeated calls over the past 20 years, was highlighted by Noakes and Draper7 in 2007. This survey provided an opportunity to appraise the current state of data collection on catastrophic injuries in the schoolboy game in Great Britain and Ireland.
Methods
The aim was to obtain as complete a dataset on the epidemiology of these injuries as possible. An initial attempt to identify injuries through audit records within the NHS proved difficult. Although detailed information services division discharge summary coding is available in each region, accessing it is fraught with obstacles and no detail can be reliably attached to the figures due to issues of data protection and patient confidentiality. Data recording systems in Accident and Emergency Departments differ throughout the countries, with no opportunity to identify those patients injured playing rugby. The only reliable data source proved to be the 12 spinal injuries units in Great Britain and Ireland which over the past 2 years were approached on a number of occasions with requests to identify rugby-related admissions in patients aged under 19 years.
Finally approaches were made to representatives from the four home rugby football unions to confirm that cases reported to the unions reflected those admitted to the spinal injury units.
Limited statistical analysis was performed applying the χ2 test.
Results
Two of the 12 spinal injury units collated data prospectively, while two further units were able to provide figures with ease. However, in most data retrieval was difficult and time consuming. Datasets from Ireland and Scotland were reasonably complete due to the limited number of units involved and admissions since 1996 were traceable. The nine units with a wide geographical spread in England proved more challenging and as a consequence records were only traced back to year 2000, following which rearrangement of official records made it more possible to cross-check catastrophic cases.
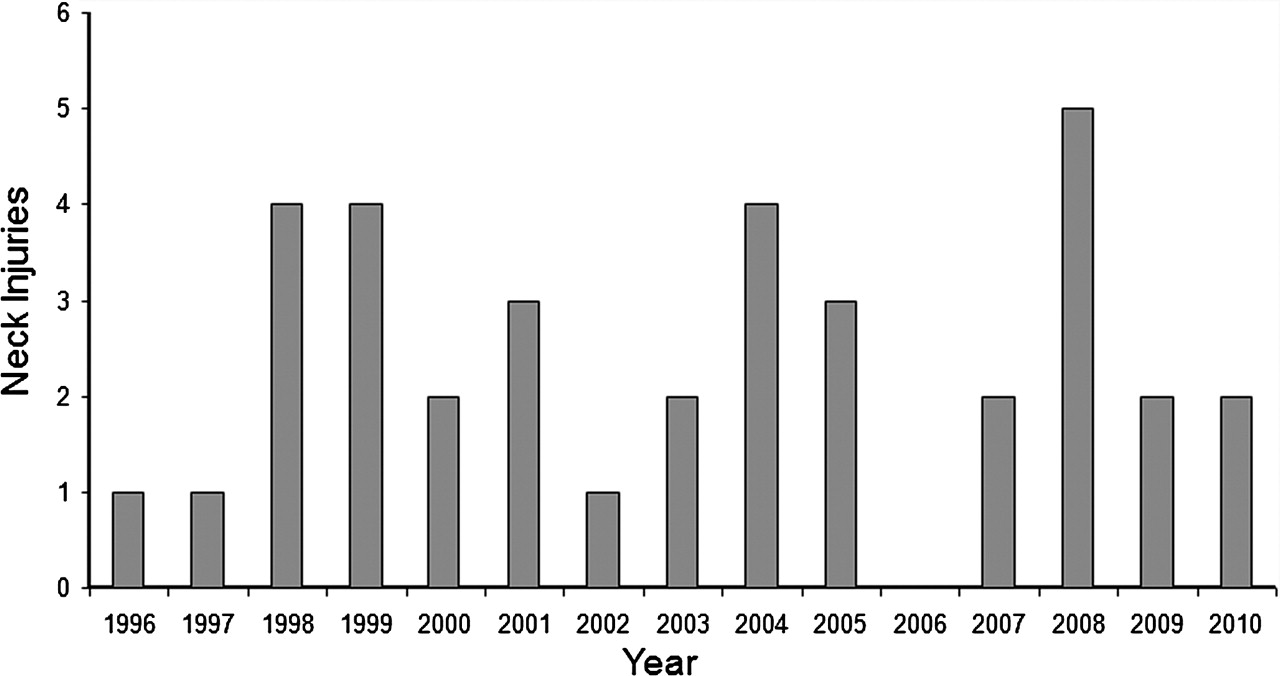
Table 1 lists those admissions for which there was confirmed record of admissions. Between years 1996 and 2000 eight admissions were recorded in Ireland, of which four occurred in 1998. During the same period there were two admissions in Scotland. Since 2000, eight cases were admitted in Scotland, of which five were in years 2007 and 2008, six cases in Ireland and 11 in England and Wales. The annual variation of admissions is illustrated in figure 1.The age at time of injury ranged between 14 and 18 years (mean 16.2 years, median 17 years). This represented 54% of all ages admitted to the national spinal injuries unit in Glasgow6 with rugby injuries in Scotland over the same period and 45% of those in Eire.5

Annual variation in admissions to spinal injury units with serious neck injuries from schoolboy rugby
Admissions to spinal injury units
The mechanism of injury was scrum in 13 (36%), tackle in 17 (47%), two due to mauls, two due to collisions, one due to a kick and one due to a ruck. With regard to neurological deficit, 16 (44%) were complete at presentation (ASIA/Frankel A), 9 (25%) had incomplete neurological deficit (partial spinal cord injury assessed as 1 Frankel B, 8 ASIA/Frankel D) and 11 (31%) had no neurological deficit. Of the 16 with complete neurological deficit, eight were injured in the scrum, five in the tackle, two in collisions and one in a maul. Of the nine with incomplete neurological deficit, four were injured in the tackle, four in the scrum and one in a ruck. Of the 11 with no neurological deficit, 8 were injured in the tackle, one in the scrum and one due to a kick and one due to a maul.
Injury in the tackle resulted in eight (47%) with no neurological deficit, four (23%) with incomplete neurological deficit and five (29%) with complete neurological deficit. Injury in the scrum resulted in one player (8%) with no neurological deficit, four (31%) with incomplete neurological deficit and eight (61%) with complete neurological deficit.
The statistical significance was calculated for: (i) the association between complete neurological deficit (ASIA/Frankel A) in scrum injuries (61%) compared with tackle (29%) (p<0.001); (ii) the association between any neurological deficit (ASIA A-D) sustained in the scrum (92%) compared with any neurological deficit sustained in the tackle (53%) (p=0.001) and (iii) for serious neck injury without neurological deficit following a tackle injury (47%) compared with a scrum injury (8%) (p<0.001).
Discussion
Despite repeated recommendations in the literature8 9 no register of catastrophic injury in rugby exists within the home unions. Additionally, there is inconsistency between official records within the unions and those recorded in this study, which were obtained through direct liaison with the hospital units treating these seriously injured patients.
The IRB (International Rugby Board) launched an online reporting system for catastrophic injuries in rugby in January 2011. While this is an important development, it will require resource and effort if the difficulties encountered in this audit are to be overcome. Early collection of data with analysis is crucial, with feedback at the earliest opportunity. Comparison of data internationally will be of interest. However, of more relevance locally is aggregation and evaluation of data within Great Britain and Ireland, hopefully resulting in collaboration and sharing of experience and knowledge.
The IRB definition of a catastrophic neck injury is one in which a spinal cord injury ASIA grades A–D is present at 48 h.10 By this definition, only 24 of the 36 injuries reported in this series would have been classified as catastrophic. Consequently, a third of admissions to spinal injury units with serious neck injuries in the study period would have remained unrecorded and therefore unavailable for analysis. In this series that would have included three vertebral burst fractures, seven facet dislocations or subluxations, one rotatory subluxation and one spinous process fracture. The last of these injuries is the only one of limited significance, while the remaining 11 represent potentially catastrophic injuries or ‘near misses’ (figure 2). Previous authors have recognised the significance of near misses11 suggesting they can provide ‘collateral evidence of trends in frequency of serious injury’.4 Williams and McKibbin12 proposed that a serious neck injury is one showing sufficient instability to damage the spinal cord or requires surgical stabilisation. Such a definition of serious neck injury should be recorded in registers rather than restricting it to catastrophic injury involving spinal cord damage. Failing to do so would prevent a significant proportion of serious neck injuries from being recorded or analysed.

{kind=link}
{kind=link}
A “near miss” injury—C4/5 bifacet dislocation with no spinal cord injury.
In the light of recent injuries in Scotland, this survey focused on schoolboys—a group recognised as being at increased risk by a number of previous authors.2 3 13 14 A recent review from South Africa15 has observed that players aged 17 years had the highest number of spinal cord injuries, although other reviews have suggested that the peak age is slightly older at 22–25 years.8 11 16
In the absence of any previous comparable nationwide survey it is not possible to comment whether serious neck injuries are occurring more or less frequently than in earlier decades. However, it is clear that in this era of professional rugby, this survey does confirm that such injuries continue to occur in schoolboys with a low but persistent frequency. No attempt has been made to compare incidence within the four home unions for a number of reasons. While every effort has been made to confirm reliability of those cases included, it is, of course impossible to know whether cases have been missed. The absence of a reliable denominator, that is, the respective playing numbers at various ages, has long been recognised as an issue.17 The four home unions provided estimates for their current playing populations (table 2), but how these have varied over the study period is not known. In addition, one important potential source of error was that the majority of youth players who were registered with clubs were assumed also to be registered with their schools. Despite these shortcomings and the fact that the Scottish dataset is probably the most complete, the high number of injuries for a comparatively small playing population in Scotland is evident and a cause for concern. Confirmation of this fact was one of the primary objectives of this study and justifies the measures that have been undertaken by the Scottish Rugby Union in revising regulations regarding under 16-year players playing in the under 18-year age group. This prevents anyone in the younger age group playing in the front row and physical maturity testing for players under 16 years wishing to play in any other position in the under 18-year age group. A group of senior orthopaedic surgeons and research physiotherapists in Scotland are currently involved in research related to serious neck injures in schoolboy rugby players and the situation remains under close scrutiny.
Registered players aged 12–18 years
More injuries occurred in the tackle (47%) than the scrum (35%) and this is in keeping with reported trends in the adult literature,8 16 17 although there does appear to be significant variation with scrum injuries still predominant in some countries.18 19 One of the few studies to concentrate on schoolboys reported an overall reduction of injuries subsequent to law changes in the schoolboy game in South Africa.20 However, the reduction occurred due to a decreased incidence in high tackles while the scrum injuries were unchanged despite some of the law changes affecting the scrum. Additionally, law changes failed to reduce scrum injuries in Argentina.21 Tackle injuries have increased proportionately over the past decade. This is likely to be due to the large impact forces consequent on the increased mass and velocity of players in the modern game. Modern tackling techniques further contribute to increased risk, in particular tackles above the waist and the involvement of multiple tacklers.
It would appear from this series that, while less frequent, neck injuries in the scrum are more serious and are associated with a statistically significantly increased risk of spinal cord injury, at least in schoolboys. Injury at the point of scrum engagement has been identified by a number of authors19 22,–,24 and indicted in more than two-thirds of cases of catastrophic spinal injury in scrum collapse. Separate engagement of the front rows has been suggested previously;22,–,24 although there is limited evidence to suggest that this has been tried in practice, mechanical testing in schoolboys has demonstrated significant reduction in the forces on the front rows when the front rows engage separately followed by the rest of the scrum.25
‘Winning the hit’ is commonly discussed by rugby commentators referring to gaining an advantage at scrum engagement. Competition at such a stage of the scrum risks destabilising it. While such practice may be an option in adult players who are likely to be matched for strength, conditioning and experience, there is no place for this in schoolboy rugby where mismatch in any of these three may well occur. The scrum is an integral part of rugby union. However if it is to be maintained, coaches and referees need to work with medical professionals to scrutinise this phase of the game in the light of all recorded serious neck injuries.
From this study, it would seem that a proper appraisal of separate engagement in schoolboy rugby should be a consideration, while a review of current tackling methods in relation to the injuries caused should also be regularly undertaken.
In conclusion, it will be clear that, while this study is not reporting an increase in serious neck injuries in schoolboy rugby that would suggest the game has become less safe, it highlights the ongoing deficiency in data collection. All contact sports carry an inherent risk of injury, and it is incumbent on the rugby authorities, the IRB in association with the home unions, to minimise this risk wherever possible. This must begin with improved data collection and analysis, without which it is not possible either to identify what needs changing or to assess the effect of any changes introduced.
Acknowledgments
The authors thank the senior medical and secretarial staff at all 12 spinal injury units approached over the past 2 years. The authors also thank the medical officers at the home unions including Dr J Robson (SRU), Dr M England (RFU), Dr C McCarthy (IRFU) and Dr R Evans (WRU).
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed