Article Text

Abstract
Objective To determine the incidence of sudden cardiac arrest (SCA) and sudden cardiac death (SCD) in men and women.
Design Retrospective cohort study.
Setting Two popular urban 42 km marathons.
Participants 1982 to 2009 finishers.
Assessment of risk factors Race records were assessed for finishers, age distribution and cardiac events by sex.
Main outcome measures The SCA/SCD incidence for all (total), male and female finishers.
Results There were 548 092 finishers with women finishers increasing from 10% to 40% over the first 18 years and remaining near 40% for the last decade. There were 14 SCA events (1 woman, 13 men) with seven successful resuscitations yielding an all finishers SCA rate of 2.6 per 100 000 finishers. The SCA rates (per 100 000) for men and women were 3.4 (95% CI: 1.8 to 5.9) and 0.6 (95% CI: 0.0 to 3.3), respectively (p=0.079). The male SCA rate for the 2000–2009 decade was 4.6 per 100 000 finishers (95% CI: 1.8 to 9.5). Eleven of 13 men were >39 years old. The OR of a man experiencing SCA compared with woman was 5.7.
Conclusions As the number of women participating in these two marathons has increased, the difference between the men's and total SCA and SCD incidence has increased for men, especially >39 years old, from coronary artery disease with men's incidence for SCA of 1 in 22 000 and SCD at 1 in 50 000 finishers over past decade.
Statistics from Altmetric.com
Introduction
Cardiac arrests in long distance road racing create front page news. While the statistics are not alarming, sudden cardiac death (SCD) in road racing attracts the attention of the media and focuses the public away from the health benefits of regular exercise. Sudden cardiac arrest (SCA) due to ventricular fibrillation during a marathon was first profiled following a death of a 44-year-old veteran marathon runner in the 1973 Boston Marathon1. As the number of marathon finishers has increased to approximately 450 000 per year in the USA, the annual number of deaths has also increased. SCA incidence reported in two US marathons was 1 in 49 000 finishers from 1976 to 2004 with four successful resuscitations resulting in an SCD incidence of 1 in 88 000 finishers, and in the last decade of the study, the SCD incidence was 1 in 220 000 finishers reflecting an increase in successful resuscitations2. The incidence of SCA (all male) at the London Marathon from 1981 through 2006 was 1 in 59 000 finishers with 6 of 11 successful resuscitations resulting in a SCD incidence of 1 in 130 000 finishers3. While these statistics are comparable and useful for estimating overall risk, they do not reflect the increasing participation of women in distance racing and the changes in incidence for men running in these races.
The Twin Cities (TCM) and Marine Corps (MCM) Marathons have tracked finishers by sex since 1982. In 1982, about 10% of marathon finishers across the nation were women, and in the last decade women comprise nearly 40% of finishers. This reflects a changing runner demographic that has altered the incidence pattern for cardiac events. Although the incidence of cardiac arrest seems relatively stable or even decreasing around the world, previous studies of risk have looked at all finishers without regard to sex2,–,4. The combined TCM/MCM database of mainly non-elite runners from around the country provides a look at incidence changes by sex and age over nearly 3 decades.
The purpose of this study is to investigate the incidence of SCA/SCD for the men's cohort as the number and percentage of women participating in the marathon has increased.
Methods
This is a retrospective cohort study of overall, male and female cardiac events in MCM and TCM participants from 1982 through 2009. The finisher statistics have been documented by each race. Cardiac events were collected from race records, personal communications, and newspaper accounts from 1982 through 2009. Outcomes were gathered from the press, from family members, from race officials, and when available, from autopsy reports. The sex, age, course location and cause of each cardiac arrest were recorded.
The incidence of SCA and SCD was calculated for total, male and female finisher cohorts based on respective cardiac events (numerators) and finisher numbers (denominators). The incidence for each cohort was updated for each year using the formula: annualised incidence per 100 000 finishers = {(∑ (cardiac events 1982 to year x)/∑ (participants 1982 to year x)) X 100 000}. The total cohort was divided into two subcohorts that reflect the rising percent of women finishers from 23% (1982–1999) to 40% (2000–2009) of the total cohort.
Fisher's exact tests were used to compare the incidence of SCA and SCD between males and females for the total cohort (years 1982 through 2009) and for the subcohorts (years 1982–1999 and 2000–2009). Exact 95% CI were also calculated. A p value <0.05 was considered statistically significant. Statistical analysis was performed using SAS V9.1.3.
The current study has been classified as exempt by the University of Minnesota Investigational Review Board (0712E23241).
Results
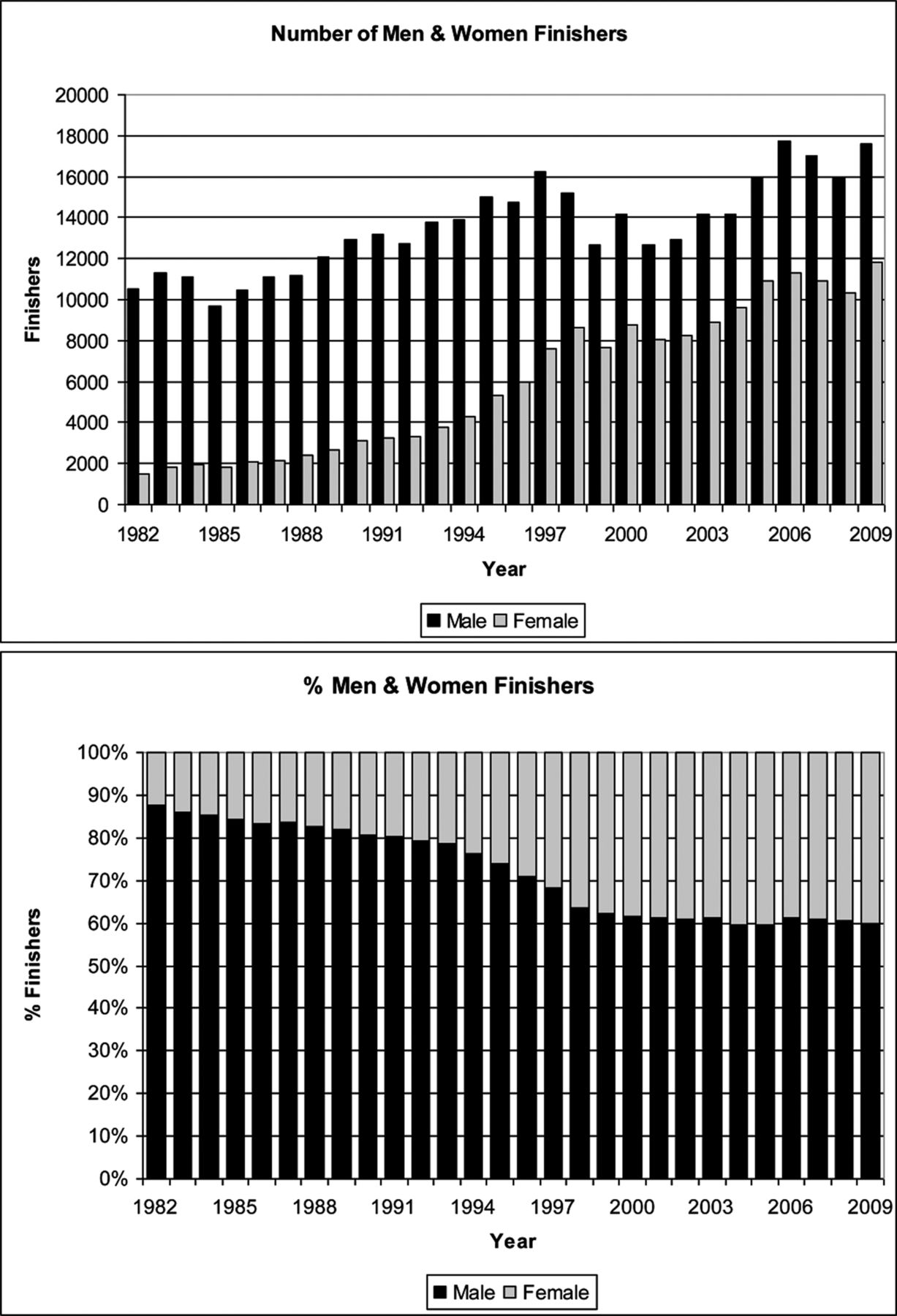
A total of 548 092 runners finished the two marathons (70% from MCM); 379 863 finishers (69%) were men and 168 227 finishers (31%) were women. In 1982, 75% of the men and 85% of the women were under age 40 years, and in 2009, 55% of the men and 71% of the women were under age 40 years in the TCM. The average ages for men and women were 35 and 32 years old in 1982 (estimated) and 39 and 34 in 2009 (actual) also at TCM. Over the first 18 years of this cohort, the annual % women finishers increased from 12 to 39 (average 23) and remained near 39% annually for the last 10 years (figure 1).
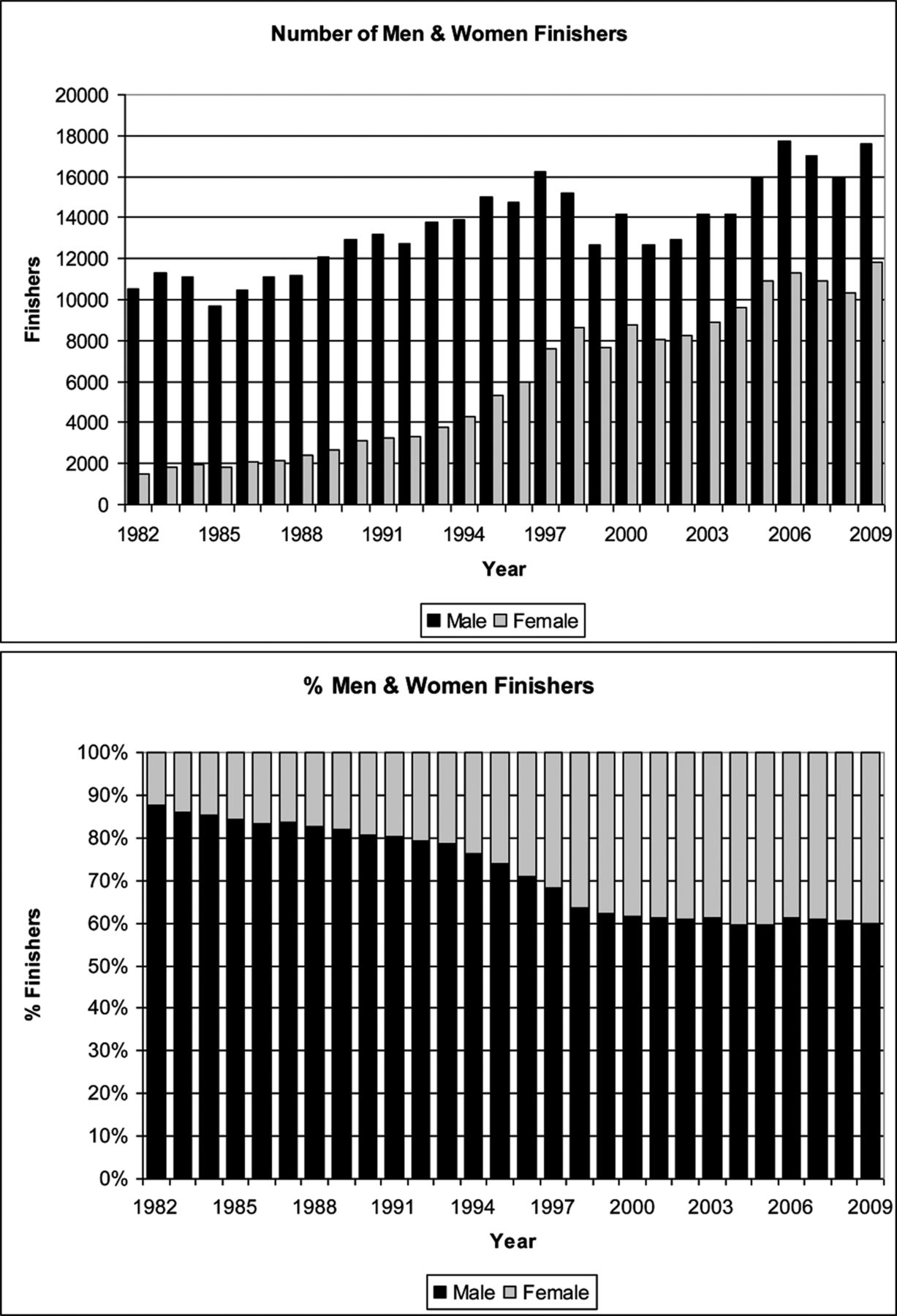
(A) The number of men and women finishers has increased steadily since 1982 with the greatest increase in the per cent of women finishers occurring between 1982 and 1999. (B) Women comprised 12% of the finisher field in 1982 and increased to approximately 38% by 1999. From 2000 to 2009, the women averaged 39% of the finishers.
Fourteen runners collapsed due to SCA in the 1982–2009 cohort with 7 successful resuscitations yielding an SCA incidence of 1 per 39 000 (2.6 per 100 000) finishers and an SCD incidence of 1 per 78 000 (1.3 per 100 000) finishers. There were 227 635 men and 69 358 (23%) women finishers from 1982 to 1999 with 7 SCA and 4 SCD, and there were 152 228 men and 98 869 (39%) women finishers from 2000 to 2009 with 7 SCA and 3 SCD.
In 1990, a 19-year-old woman collapsed at mile 24 with SCA and subsequently died; on autopsy she had an anomalous left main coronary artery. Thirteen SCA events occurred in men aged 28–60 years old and 6 did not survive (table 1). The 28-year-old male who survived SCA had a mitochondrial defect found on muscle biopsy and normal angiography5. The other male runners ages 32–60 years old had underlying coronary artery disease (CAD) of varying severity.
Clinical data for cardiac arrests occurring in 13 male marathon runners
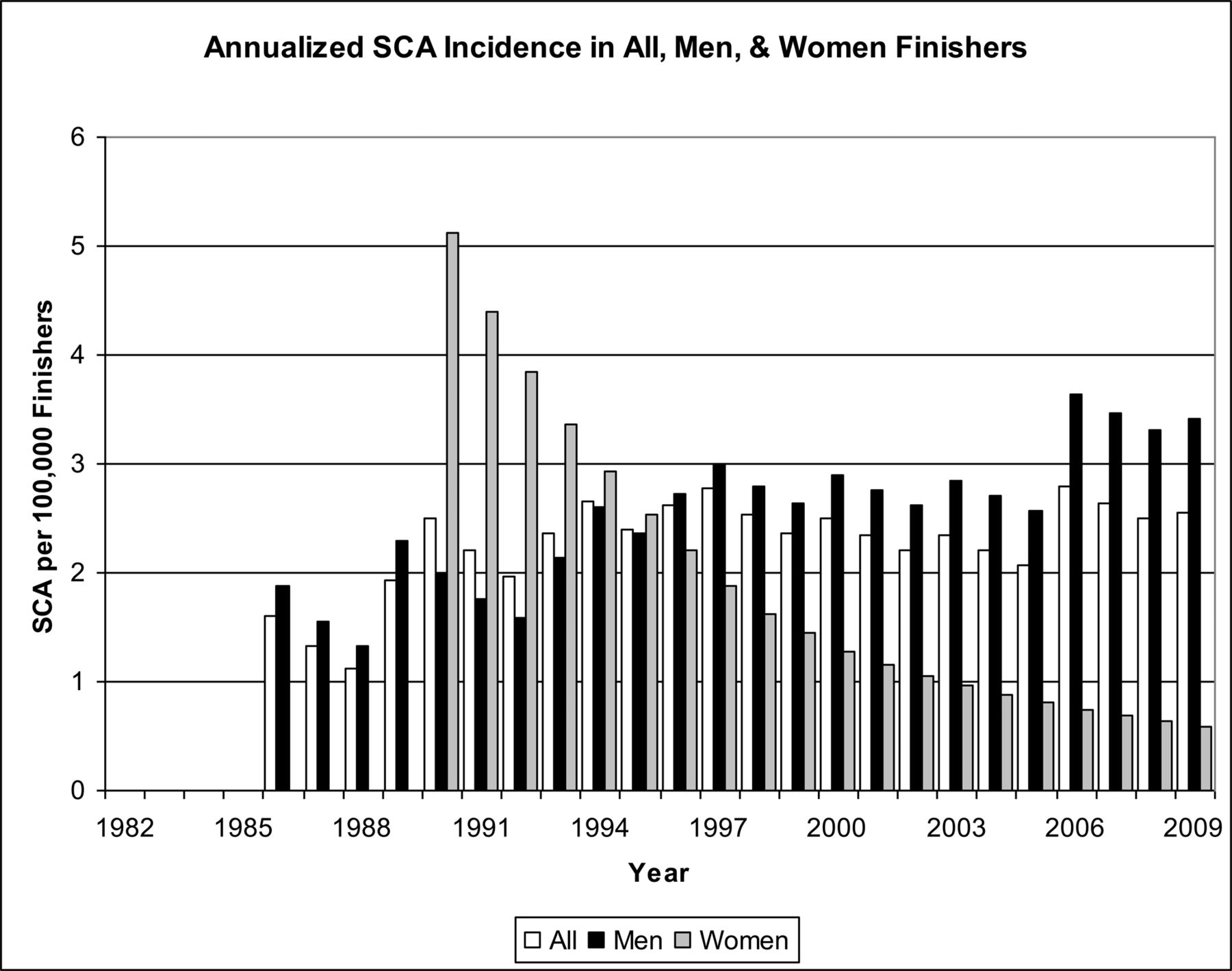
The ‘annualised’ all, male and female SCA incidence per 100 000 finishers is presented in figure 2. The SCA incidence for the 28 year cohort was 3.4 (95% CI: 1.8 to 5.9) per 100 000 men and 0.6 (95% CI: 0.0 to 3.3) per 100 000 women (p=0.079). The SCD rates during the 28 year period were 1.6 (95% CI: 0.6 to 3.4) per 100 000 and 0.6 (95% CI: 0.0 to 3.3) per 100 000 for males and females respectively (p=0.684). The RR for a man in this cohort to experience SCA compared with a woman was 5.7 and compared with all finishers was 1.3.

The solitary death of a woman runner in year 1991 produced the highest incidence of sex associated SCA risk across this 28 year study. However, the incidence for women has steadily declined as the number of women finishers has increased. In contrast, the men's incidence has increased steadily along with an increase in male finishers across the years of this study.
The 1982–1999 (23% women) and 2000–2009 (39% women) subcohorts each had seven SCA events. The male and female SCA incidence for the all finisher cohort and both subcohorts is shown in figure 3. The male SCA and SCD rates for years 2000–2009 were 4.6 (95% CI: 1.8 to 9.5) per 100 000 and 2.0 (95% CI: 0.4 to 5.8) per 100 000. In comparison (figure 3), the male SCA/SCD rates for 1982–1999 were 2.6 (95% CI: 1.0 to 5.7) and 1.3 (95% CI: 0.3 to 3.9) per 100 000. The incidence risk ratio for men experiencing SCA from 2000 to 2009 compared with 1982–1999 was 1.8.

{kind=link}
{kind=link}
{kind=link}
The men's 2000–2009 subcohort SCA risk increased in the last decade compared with the entire cohort and the 1982–1999 subcohort. The dashed line represents the combined men and women SCA incidence across the 1982–2009 cohort.
Discussion
The incidence of marathon related SCA across this cohort ranged from 1.1 to 2.8 per 100 000 finishers with a narrower range of 2.1 to 2.8 over the last decade when approximately 40% of the finishers were women. The 2000–2009 men's cohort SCA incidence was 4.6 per 100000 male finishers compared with the incidence for the 1982–2009 men's incidence of 3.6 and 1982–1999 of 2.6, implying a greater risk for men in the last decade. In contrast, the women's incidence rate across the total cohort is now at a low of 0.6 per 100 000 female finishers and was zero for the last decade. This difference in the male rates compared with the total cohort (men and women combined) was due, in part, to the increasing number of women participating in the marathon and possibly other factors like the ‘ageing’ of the men's cohort. For the SCA incidence to equalise for men and women in the next year, assuming the same field size and sex distribution for the next set of races, 8 women would have to experience an SCA. This would be unlikely given that only one woman experienced an SCA in the past 28 years.
Total, men's, and women's participation numbers increased steadily from 1982 through 2009. The changes in men's and women's participation in the US during this time period are reflected in this study cohort. Looking at national statistics for marathon participation, the number of finishers continues to rise and the % women finishers has increased in parallel with this study cohort6. The relative sex distribution of US marathon finishers in 2007 was 39.5% women and 60.5% men6. In the 28 years of this cohort study, women finishing these marathons increased from 12% to 39% by year 18, and the percentage has remained at nearly 40% over the last decade (figure 1B), reflecting national participation trends. Nationally, women tended to be younger than men with 62.5% of the women and 48.1% of men <40 years old6. Women have increased SCA risk after age 50 years old and in 2008–2009 only 7% of TCM women finishers were >50 years old, so the actual group of women at most risk for SCA was smaller than the men's cohort. As in this study, the Women's Health Study showed a very low cardiac risk during and following exercise, and women who are habitually active have the lowest risk of SCD during or following exercise and away from exercise7. It is likely that many of the women in this cohort, based on the younger age of female marathon participants, are at less cardiac risk than the older male cohort.
Over age 35 is the traditional age mark for separating CAD and other causes of cardiac collapse in men. CAD is the culprit in the vast majority over age 35 and indeed 11 of the 13 male cardiac arrests in this current study were in men over 39 years old and all were attributed to CAD. The average age of the male cohort has risen from 34 (1982) to 39 (2009).
In this study, the difference in male and female SCA incidence across 28 years is nearing significance (p=0.079). As the women's cohort has increased in number over the last 2 decades, the absolute risk has decreased to a rate of approximately 1 in 200 000 finishers. Considerably lower than the 1 in 29 000 risk for all men finishers. The rates in this study are consistent with those reported for the 2000–2009 decade by the RACER group of 1 SCA per 100 000 finishers, along with a mixed half marathon – full marathon incidence of 0.9 per 100 000 male finishers and 0.16 per 100 000 female finishers8.
This study includes all known SCA and SCD associated with these marathons since 1982, but it is possible that an event occurred after the marathon and the connection to the respective road race was not established. The number of events is very small, limiting the statistical power of the cohort. There is likely under reporting of SCA nationally as these events are not a matter of public record, unlike SCD. SCD is easier to track because it rarely escapes media coverage. The sex distribution of this cohort closely matches the changes seen at the national level, but unfortunately the age statistics are not readily available for the entire cohort.
What this study adds
-
The risk of cardiac arrest for men during marathon participation has increased across 28 years of this study compared with the women and men combined and women alone.
-
The risk for men alone is 1 in 29 000 finishers over 28 years and 1 in 22 000 finishers from 2000 to 2009.
-
Women participants are at exceedingly low risk in this cohort (1 in 200 000 finishers).
-
Participation of women in the marathon has increased from 10% to 40% from 1982 to present and the average age of women has increased from 32 to 34 while the average age of men has increased from 35 to 39 with considerably more men in the at-risk age group for cardiac arrest.
Women are at considerably less risk for cardiac events during the marathon compared to men. The overall cardiac event risk has remained relatively stable across nearly 3 decades of marathon racing; however the risk to men has increased during the same time period as the number of mainly younger women participating in the event has increased. This increase in women running the marathon has masked the rise in the men's SCA incidence when the aggregate risk is reported without segregating the men's and women's cohorts. The medical management preparations for marathon road races should continue to emphasise cardiac field care and deploy defibrillator equipped emergency cardiac response teams along the entire course to facilitate rapid response to collapsed runners.
Conclusions
The RR of SCA for this cohort, which seems to reflect national participation by age and sex, is nearly sixfold higher for men compared with women. The incidence of SCA and SCD for the entire cohort was 1 in 39 000 and 1 in 78 000 finishers, respectively. For men finishers, the SCA and SCD incidence was 1 in 29 000 and 1 in 60 000 for the 28 year cohort and has increased to 1 in 22 000 and 1 in 50 000 in the last decade. The increased incidence in men, especially over age 40 years old, has been masked by the influx of women runners and sex specific incidence should be used to report cardiac risk.
Acknowledgments
The authors thank the staff and volunteers at the Twin Cities and Marine Corps Marathons for the care of the runners and the contributions to marathon medicine.
Footnotes
-
Competing interests None.
-
Ethics approval University of Minnesota Investigational Review Board (0712E23241).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmjgroup.com