Article Text

Abstract
Background The London 2012 Summer Olympic Games involved 10 568 elite athletes representing 204 competing nations. To manage the varied healthcare needs of this diverse population, a Polyclinic was constructed in the athletes’ village.
Aim This work aims to summarise the usage of the Polyclinic by competing athletes and the facilities available to them.
Methods All Polyclinic encounters were entered into a database from which data were exported for the time frame 28 July–12 August 2012, inclusive to cover the first to last full day of competition. Only Polyclinic data involving accredited athletes were analysed. All types of encounters were collected for analysis, not just sports-related issues.
Results There were a total of 3220 encounters within the Polyclinic. This figure combines medical consultations, radiology/pathology investigations and prescriptions dispensed. Of these 3220 encounters, there were 2105 medical consultations; musculoskeletal comprised the greatest number (52%), followed by dental (30%) and ophthalmic (9%). The most frequently used imaging modality was MRI and diagnostic CT was used the least. After correction for multiple entries, Africa provided the largest proportion of athletes attending the Polyclinic (44%) and Europe the least (9%). Peak usage of all facilities was seen around days 9 and 10 of competition, reflecting the busiest time of the competition and the largest number of athletes in the village.
Conclusions The Polyclinic managed a wide variety of both sports-related and non-sports-related injuries and illnesses. The breadth of specialists available for consultation was appropriate as was the ease of access to them. The radiology department was able to satisfy the demand, as were the pharmacy and pathology services. We would recommend a similar structure of facilities and available expertise in one clinic when planning future mass participation sporting events.
- Olympics
Statistics from Altmetric.com
Background
The London 2012 Summer Olympic Games involved 10 568 elite athletes competing for 204 separate National Olympic Committees (NOC's). It was of comparable size to that of previous Summer Games1 ,2 but over twice the size of either the 2002 Manchester Commonwealth Games (3679 participants)3 or 1948 Summer Olympics (4104 participants) previously held in London.4 To manage the varied healthcare needs of those involved, a polyclinic was constructed on the athletes’ village site in Stratford, East London. The London Olympic Games Organising Committee (LOCOG) aimed to provide a dedicated on-site medical facility to be staffed by volunteer experts across multiple sports-related specialties similar to that of previous Games.2 ,5 Their aim was to manage the majority of Games-related healthcare issues internally in an attempt to provide an optimal level of care and avoid pressure on local hospitals and other healthcare providers.
Protection of the health of competing athletes remains a key objective during Olympic Games and forms an important part of the International Olympic Committee's (IOC) agenda.6 ,7 One of the main aims of the IOC is to provide freely available healthcare to all athletes during Games as well as institute safeguarding measures to protect athletes during competition. It is accepted that the healthcare needs of elite athletes is complex and extends beyond the immediate injuries sustained in competition. Furthermore, the incidence of injuries and illnesses is known to vary according to individual sports and by the athlete's country of origin.8 ,9
This paper aims to summarise the utilisation of resources within the clinic as well as comment more generally on patterns of usage by different nations. In presenting data on only those competing, it will provide a novel insight into the health-seeking behaviours of a diverse population of elite athletes. The scale of the facility is detailed as well as the equipment and personnel needed to service such a large event involving worldwide participants from varied domestic healthcare systems.
Methods
The Polyclinic was situated within the Athletes’ village in Stratford, East London and was in proximity to the main Olympic Park. It functioned as a small hospital and was arranged over five fully integrated floors. In the basement a small pool, zero gravity treadmills and massage tables provided rehabilitation and recovery facilities. The ground floor was the administrative centre with a reception, pharmacy and offices. There was also an acute care department including three beds for overnight admission. The first floor was the main treatment hub and included consultation rooms (sports medicine, general medicine, therapeutic radiology), a physiotherapy department and a research centre. The second floor was used for sports medicine and podiatry, and the top floor contained large dental and optometry departments as well as meeting rooms.
The Polyclinic was staffed entirely by volunteers and included general physicians, sports medicine doctors, dentists, ophthalmologists, optometrists, physiotherapists, podiatrists and sports massage therapists. Other services included a dispensing pharmacy and fully functioning radiology department staffed by musculoskeletal radiologists. In addition, specialists could be called upon to visit athletes in the Polyclinic, and there was ready access to extensive services in the nearby Homerton and Royal London hospitals.
All medical encounters were entered into a specially designed database (Atos IT Services Limited, London, UK), which was available to all staff working in the Polyclinic. The data inputted included general athlete demographic information, history of presenting complaint, past medical conditions, examination findings and investigations requested. The pharmacy and medical departments both used the same system and therefore allowed for accurate continuity of care and confidential data collation. The database was password protected and any paperwork containing athlete information (requests or results) was destroyed after the Games to ensure that confidentiality was maintained.
Comprehensive blood analysis services were provided at the Polyclinic throughout the Games period. This testing was separate from the doping blood analysis, which was performed independently by the World Anti-Doping Agency in a separate facility. The pharmacy department was only able to dispense medication prescribed by a doctor within the Polyclinic. Private prescriptions from outside were not dispensed. It was stocked with a wide range of drugs in line with current antidoping policy.
The radiology department was equipped with 1.5 and 3 Tesla wide bore MRI scanners, Discovery 750 HD 64 slice CT scanner, 2 Logic E9 ultrasound units and an XR656 wireless digital x-ray system. Integrated radiology information system (RIS) and Picture Archiving and Communication System were set up with facilities for voice recognition to generate and store dictated reports. Referrals for radiological investigations were accepted directly from both team doctors and LOCOG doctors based at the polyclinic and at the event venues. Radiology requests were entered into the RIS system and this dataset was used to obtain imaging statistics.
Experienced musculoskeletal (MSK) radiologists reported all radiological investigations apart from general ultrasound examinations that were carried out by trained sonographers. Interventional procedures were performed both under CT and ultrasound guidance by MSK radiologists. During the Games, the majority of investigations were performed on athletes, followed by team officials and then the work force. Athletes still competing were given preference over athletes who had finished their events. Requests for MRI and ultrasound were still being received on the closing day of the Polyclinic.
Data were exported from Atos and RIS for the time frame 28 July–12 August 2012, both days inclusive. Although the football competition started prior to this date, the opening ceremony was held on 27 July and the first full day of the competition started on 28 July.
We defined ‘Polyclinic encounters’ as any accredited athlete seeking medical attention for injuries and illnesses sustained in both competition and training during the London Olympic Games. This included all medical consultations, pharmacy, pathology and radiology investigations/procedures. Non-athletes such as coaches, officials and other NOC staff seeking medical attention were excluded from the analysis. Encounters taking place in any medical facility other than the Polyclinic, including in the field of play venues, were excluded as this work relates only to usage of the Polyclinic.
Data analysis and correction for duplicate data were performed using Excel, version Mac OS X (Microsoft, Redmond, Washington). Countries have been grouped into their respective continent based on the United Nations Statistics Division classification.10 The proportion of attendances for individual athletes was calculated by dividing the number of individuals who were seen in the polyclinic by the total number of individual attendances. We present radiology data with means and SD.
Results
Usage of polyclinic departments
Medical consultations
General
Medical consultations included interactions with any of the healthcare specialists, that is, general physicians, sports medicine doctors, dentists, ophthalmologists, optometrists, physiotherapists, podiatrists and sports massage therapists. In total, 2105 medical consultations took place over the 16-day period. These data are summarised in figure 1 and illustrate a peak attendance around days 9 and 10 of the competition when over 250 consultations took place each day (mean 201 daily consultations).

Summary of all medical consultations, which occurred in the Polyclinic during the Games period.
Musculoskeletal (52% of all encounters) and dental care (30%) were the most common categories under which encounters were logged. Consultations covered a wide range of medical specialties and were not limited to only exercise-related complaints (table 1).
Summary of all medical encounters
Musculoskeletal encounters
The subdivision of complaints within the category is illustrated in table 2. On a review of the clinical records, the 31% who were logged as involving ‘multiple locations’ most commonly related to athletes seeking physiotherapy or sports massage with multiple muscle tension points.
Summary of musculoskeletal encounters seen in the Polyclinic during the Games period
Radiology
A wide range of diagnostic investigations and imaging-guided interventional procedures were performed on athletes during the games (figure 2), with MRI constituting the greatest component of daily workload (mean 34, SD 9). MRI showed a generally upward trend, peaking on day 9, with 50 MRIs before steadily declining to 25 MRIs on day 16. Diagnostic ultrasounds peaked on the 10th day with 18 examinations, before coming down to 8 examinations on day 16. Compared with MRI and ultrasound, the number of plain x-rays performed had a slightly delayed peak, on day 13 with 24 examinations. A total of 36 diagnostic CT scans were performed.

Line graph of the daily number of procedures performed by the radiology department in the Polyclinic.
In contrast to the trends observed for MRI, ultrasound and plain films, the demand for interventional procedures was steady throughout the Games. Imaging-guided interventional procedures on peripheral extremities such as corticosteroid and local anaesthetic injections for indications such as tenosynovitis and bursitis were performed under ultrasound guidance. Spinal interventions, for example, selective nerve root blocks, facet joint and epidural injections were performed under CT fluoroscopy.
The maximum number of interventional procedures in a day was 6 on days 1 and 7 (figure 2). Although diagnostic CT was a less utilised resource, the use of CT fluoroscopy for spinal interventional procedures and in evaluating possible bony stress fractures was thought to be invaluable. In this application, CT fluoroscopy had a major influence on future participation and performance outcome during the competition.
Pathology and pharmacy
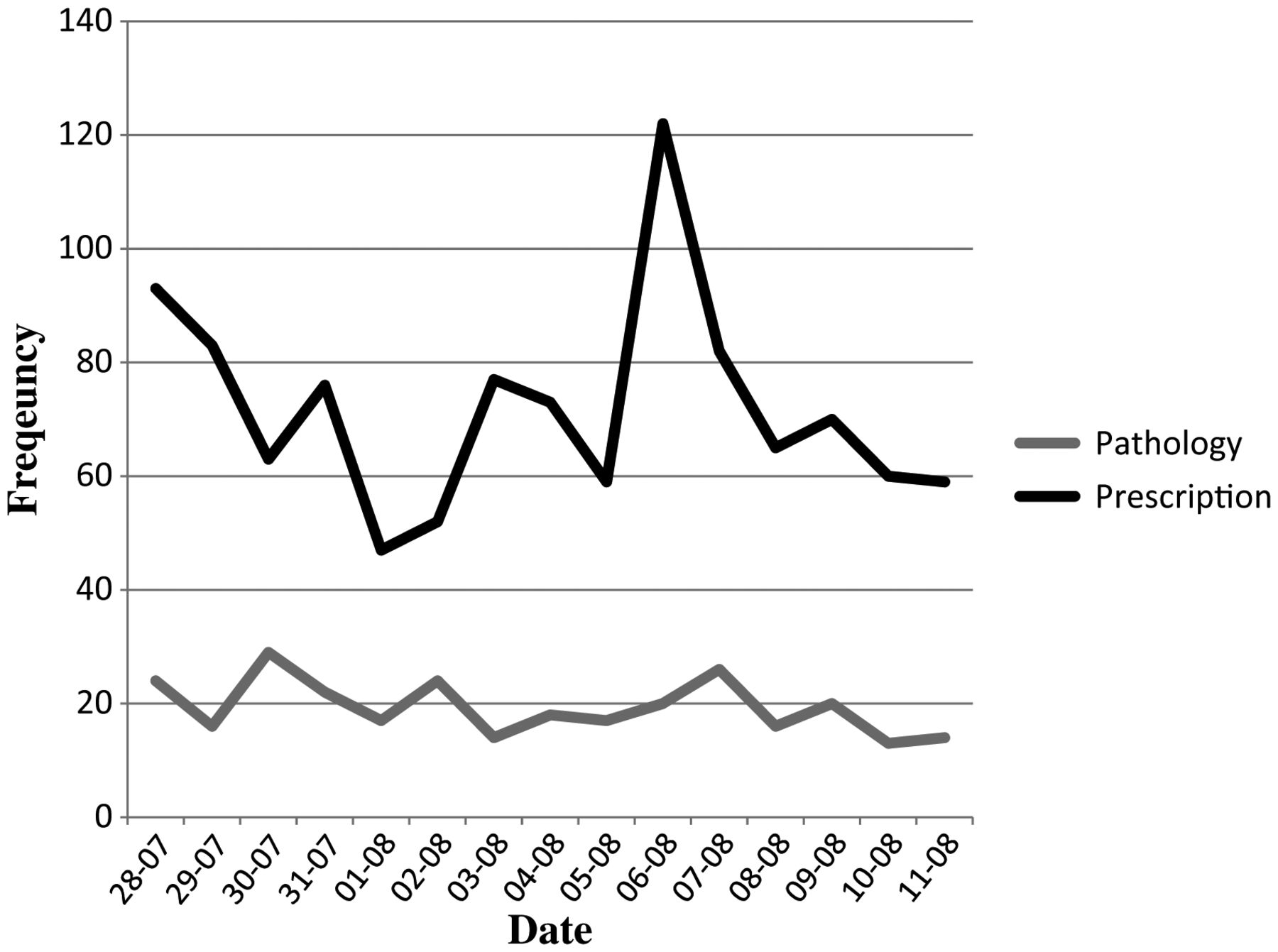
A total of 290 pathology tests were performed. These were performed at a steady rate throughout the Games with an average of 19 pathology tests performed daily (figure 3). In total, 930 prescriptions were dispensed with a mean of 62 prescriptions each day. In a similar pattern to the peak in demand for other services, a rise in prescriptions was seen on day 10 when 122 prescriptions were processed.
{kind=link}
{kind=link}
{kind=link}
Line graph of the daily number of prescriptions and pathology requests performed in the Polyclinic.
Distribution of encounters by continent
Over the 16-day period under scrutiny, there was a total of 3220 encounters within the Polyclinic (table 3). This table combines usage of all services within the facility such as medical consultations, radiology/pathology investigations and prescriptions dispensed. Each encounter has been further analysed to establish the continent of origin of the athlete.
Distribution of Polyclinic encounters by athlete continent of origin with correction for duplicate attendances
The greatest proportion of total encounters was from athletes competing for African nations (28%) followed by athletes from America (26%). Once corrected for duplicate encounters from the same athlete, Africa had the highest proportion of athletes seen at the Polyclinic (44%), and Europe the least (9%).
Discussion
This work highlights the broad range of diagnostic and therapeutic services available to athletes during the London 2012 Olympic Games. Peak usage of many of the facilities was seen around days 9 and 10 of the competition (5 and 6 August 2012). This is when there was the greatest number of event finals occurring11 and the athletes’ village was at its busiest. As expected, most consultations were musculoskeletal in origin but a sizeable proportion also related to dental and ophthalmic complaints. The demand for MRI was significant, reflecting the fact that this resource is considered not as freely available otherwise as it is during Games time. Pathology investigations were performed steadily throughout the period of competition, but the demand for pharmacy services did spike considerably.
It is interesting to note from the continent subanalysis that the greatest proportion of attendances was from athletes from African nations. This was for the gross number of overall attendances and also when corrected for multiple attendances by individual athletes. It is also interesting that although Oceania provided the smallest proportion of overall attendances (7%), this constituted the second largest fraction of visits by individual team members (30%). This reflects the fact that Oceania fielded the smallest number of athletes (670); therefore, individual attendances would constitute a greater proportion of the small Oceania cohort.
Athletes were able to self-present to the Polyclinic and would often be accompanied by their NOC's medical or administrative staff. On arriving at the Polyclinic, they were quickly triaged to the appropriate department and rarely had a significant delay in being seen. Staffing levels appeared to meet the demands effectively; however, minimal waiting time was seen for some of the busier services such as physiotherapy, sports massage and radiology. Despite being serviced entirely by volunteers, staff had undergone a comprehensive recruitment and selection process involving an induction and orientation to the building and working environment prior to the start of the Games. This enabled an efficient working environment right from the start of the Games and limited any start-up issues. Daily work force meetings at the start and end of each shift further reinforced good communication and working relations among staff from different departments in the Polyclinic.
Efficient assimilation and storage of medical encounter data were crucial throughout the Games. Workstations connected to the Games network were available in all medical venues including all fields of play to allow timely data input. This meant that records were kept contemporaneously and could be referred to during successive visits for the same individual. The Atos database provided an effective platform for these data to be securely stored and contained relevant data fields to be comprehensive and appropriate.
Practical implications and further research
The Polyclinic provided an appropriate breadth and accessibility of expertise and facilities to safeguard athlete health at the Games. Although staffed entirely by volunteers, a high level of care was delivered and the aims of LOCOG and the IOC were achieved. The healthcare of elite athletes remains a key priority in the organisation of major sporting events, although the specific impact of this can be hard to predict. The work here provides clear details of what to expect and what is required for those planning similar future endeavours.
There are several other methods for estimating healthcare needs of such a population, for example, the WHO health impact assessment (HIA).12 The HIA was found to be a useful tool in planning the public health agenda for the 2014 Commonwealth Games13 but is generally considered to lack robust evidence to consider it reliable in predicting impact accurately.14
Alternative strategies to monitor an athlete's health include the collation of epidemiological data on injuries and illnesses sustained during major championships. There are many examples of this in the literature to include youth and adult cohorts participating in a wide range of sporting pursuits.15–29 The longitudinal evidence acquired from successive championships has increased the scientific strength of these studies, making them of vital importance in the monitoring of athlete health and well-being. Work by the IOC has emphasised the importance of injury surveillance1 and has since 2008 monitored athlete's injury (and later illness) risk in each Summer and Winter Games.8 ,9 ,30
The work presented highlights those health issues which could not be managed internally by the NOC's own medical staff. Examples include: access to pharmacy medication, use of specialist rehabilitation equipment, diagnostic imaging or obtaining specialist medical opinion. This may be due to a lack of medical personnel travelling with the team or the resources available to them domestically or at the Games. Teams with a small number of athletes are limited in additional personnel travelling with the team and will often choose coaching staff over a team doctor or physiotherapist.
It is acknowledged, however, that long distance travel is an independent risk factor for illness risk among elite athletes in competition.31 In contrast, several of the larger teams choose to travel with extensive medical support diminishing the need to utilise Polyclinic services. These support staff are often present at pre-Games training camps and their own medical facilities could be seen throughout the athletes’ village. It is noted, however, that America still comprised 26% of all Polyclinic encounters despite their large number of support staff.
In summary, this work provides details of the patterns of daily usage and the facilities required by elite athletes attending the London 2012 Olympic Games. Planning and provision of healthcare at an Olympic Games is a complex task which we feel was adequately achieved at these Games. The pattern of healthcare demands at this event will provide invaluable information for planning future mass participation sporting events. It is important to remember that this is only one facet of healthcare provision at an Olympic Games. It must be combined with field of play data as well as ‘illness and injury’ data such as that collected by the IOC to produce a more complete picture of all medical needs during these events.
Conclusion
The London 2012 Summer Olympic Games was the largest mass participation sporting event to be held in the UK. It saw over 10 000 competing athletes from 204 separate nations. Much of these athletes’ healthcare needs were provided by the Polyclinic located in the athletes’ village. A wide range of diagnostic and therapeutic services were provided by the Polyclinic and these met the demands of this unique population of elite athletes. Provision and safeguarding athlete health is of paramount importance to the IOC and this was achieved through the role of the Polyclinic.
What are the new findings?
-
The London 2012 Olympic Games was the largest sporting event in the UK to date and was over 2.5 times the 1948 London Games.
-
In total, 10 568 elite athletes participated from 204 separate nations.
-
This is the first paper to categorise attendance by continent of origin and analyse Polyclinic usage using this method.
-
Peak usage is expected by days 9 and 10 of the competition, coinciding with the greatest number of event finals and number of athletes resident in the village.
References
Footnotes
-
Correction notice This article has been corrected since it was published Online First. The affiliation address for DPG has been corrected.
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com