Article Text

Abstract
Background The characteristics and incidence of injuries at the Summer Paralympic Games have not previously been reported. A better understanding of injuries improves the medical care of athletes and informs future injury prevention strategies.
Objective The objective of this prospective cohort study was to characterise the incidence and nature of injuries during the London 2012 Summer Paralympic Games.
Methods Injury information was obtained from two databases. One database was populated from medical encounter forms completed by providers at the time of assessment in one of the medical stations operated by the Organising Committee. The second database was populated daily with information provided by team medical personnel who completed a comprehensive, web-based injury survey.
Results The overall injury incidence rate was 12.7 injuries/1000 athlete-days. Injury rates were similar in male and female athletes. The precompetition injury rates in women were higher than those in the competition period. Higher injury rates were found in older athletes and certain sports such as football 5-a-side (22.4 injuries/1000 athlete-days). Overall, 51.5% of injuries were new onset acute traumatic injuries. The most commonly injured region (percentage of all injuries) was the shoulder (17.7%), followed by the wrist/hand (11.4%), elbow (8.8%) and knee (7.9%).
Conclusions This is the largest and most comprehensive epidemiological report examining injuries in Paralympic athletes. Injury rates differ according to age and sport. Upper limb injuries are common. The knowledge gained from this study will inform future injury surveillance studies and the development of prevention strategies in Paralympic sport. The Epidemiology of Injuries at the London 2012 Paralympic Games.
- Disabled
- Epidemiology
- Injury Prevention
- Sporting injuries
Statistics from Altmetric.com
Introduction
Injury surveillance has become increasingly recognised as an important component of sports medicine.1 ,2 A detailed understanding of the characteristics of injuries improves the ability of medical providers to treat different athlete populations. More importantly, by identifying mechanisms of injury and associated risk factors, injury surveillance studies can assist in the development, implementation and assessment of injury prevention strategies.3 In recent years, there have been a growing number of randomised controlled trials that have demonstrated the benefits of injury prevention programmes.4–6
Interest and participation in the Paralympic Games have grown substantially.7 ,8 In 2012, 4176 athletes from 164 delegations competed in 20 sports at the London Paralympic Games. Athletes competing in Paralympic sports may have one or more types of impairment, including limb deficiency, spinal cord injury, visual impairment, cerebral palsy and other significant neurological and musculoskeletal conditions.
Despite the growth of Paralympic sport, relatively few studies have evaluated the incidence of injury among athletes with impairments. Prior studies have been limited by the lack of standardised accepted definitions of injury, small sample sizes, absent or limited athlete exposure data and the use of retrospective surveys assessing athletes’ self-report of injury.9
The overall percentage of injured athletes within the summer Paralympic Games has been reported in the range 17–90% across all sports.10 ,11 Only one study in summer adaptive sports has included exposure, and found an overall injury rate of 9.3/1000 athlete exposure hours in 319 athletes competing at the national level.12 Injury rates by individual sport or impairment type were not reported. In another national-level study examining wheelchair disciplines, basketball accounted for 30.9% of all injuries followed by track racing (30.6%) and road racing (12.1%).13
The anatomical location of injury has been previously reported by sport and impairment. The percentage of wheelchair athletes with a shoulder injury in international competition has been reported in the range 26–57%.,10 ,14 ,15 In women's wheelchair basketball, 72% of players reported experiencing shoulder pain during their careers.16 Among athletes with visual impairment, lower limb injuries are particularly common.,10 ,14 ,15 ,17 ,18 Athletes with cerebral palsy sustain injuries in a larger variety of anatomical regions, and frequently experience soft tissue injury which may be secondary to muscle imbalance caused by spasticity.,10 ,14
In summer Paralympic sports, the ratio of acute to chronic injuries is approximately 60:40 across studies.9 The most commonly recorded injuries are strains and sprains.10 ,19–21 Among chronic injuries, risk factors for injury have been identified, including returning to play prior to resolution of symptoms in wheelchair racing 22 and a high weekly training load in wheelchair basketball.23 In the limited number of studies available that examine gender-specific injury patterns, men and women have been shown to have a similar prevalence of injury.24–27
The main objective of this prospective cohort study was to determine the incidence rate (IR) and characteristics of injuries sustained by athletes competing at the London 2012 Paralympic Games. Additional objectives were to compare injury rates between sexes, age groups, type of sports, during the precompetition compared with the competition period.
Methods
This cohort study was a component of a large injury and illness surveillance study completed at the London 2012 Paralympic Games.28 The study was approved by the Sports Science Committee of the International Paralympic Committee (IPC) and conducted with full cooperation of the London Organizing Committee for the Olympic and Paralympic Games (LOCOG). Research ethics approval was obtained through the University of Brighton in the UK (FREGS/ES/12/11) and the University of Cape Town Health Sciences Research Ethics Committee (HREC/REF 436/2012). All data were stored on highly secured, password-protected computers. Athlete names were not collected. A unique numeric identifier for each athlete was used for the purposes of database management. This unique identifier was removed from the final database. The final database contained no information that could personally identify any athlete. Athlete consent to use their deidentified medical information for research purposes was obtained prior to their arrival to the Paralympic Village.
Data sources
The details of the data sources used in this study have been described.28 Deidentified athlete information (age, gender, sport) was obtained from an IPC database of competitors. Information regarding athlete injuries was obtained from two sources. The first source was a database populated from the electronic medical data capture system (EMDCS) used at all of the LOCOG medical stations (ATOS, France). LOCOG medical personnel completed standardised forms whenever an athlete was seen at one of their medical stations.
The second source was a more comprehensive, custom-built, web-based injury and illness surveillance system (WEB-IISS) developed at the University of Cape Town in Cape Town, South Africa. Medical personnel from the National Paralympic Committees (NPCs) were asked to complete this survey of injuries on a daily basis. In addition to obtaining more detailed injury information, the WEB-IISS required the NPCs to report how many athletes were present in London on every day of the study, thus allowing for calculation of exposure in terms of total athlete-days.
If an athlete sustained an injury, they could be seen either at an LOCOG medical station, in which case the information was populated in the EMDCS, and/or by the delegation's medical personnel, in which case the team medical staff completed the web-based survey, thus populating the WEB-IISS. We are aware of several small NPCs that shared a single physician. In these cases, the physician was given the ability to enter injury information into the WEB-IISS for all athletes that he/she saw, regardless of which country the athlete was from.
Following the conclusion of the Games, members of the research team reviewed every entry in both the EMDCS and WEB-IISS databases, which were subsequently merged into one larger database. If a single injury was captured by both databases, all of the information for this injury was merged into one encounter, identifying and aligning the variable that occurred in both. If an athlete sustained more than one distinct injury, each of the injuries was recorded separately.28
Procedures
A study of this size relies on numerous healthcare providers and research team members to capture meaningful data. It was therefore imperative to make every effort to ensure collaboration among all parties involved. Extensive measures were taken to inform the LOCOG and NPC medical staff about the project to maximise participation and minimise unreported injuries and unpopulated data fields. The IPC research team began communications regarding the study with the LOCOG Chief Medical Officer (CMO) 2 years prior to the Games. The CMO disseminated information about the project to all LOCOG medical staff. Communications were sent to NPC medical personnel by email 6 weeks and 2 weeks prior to the opening of the Paralympic Village. The first of these communications was a general announcement about the project and the second communication included a brochure with detailed information regarding data collection. The project was presented in an in-depth manner to all LOCOG and NPC medical personnel who attended the Team Physicians Meeting that took place several days prior to the start of competition. All NPC medical personnel were provided with detailed printed information about the project, including detailed instructions on how to complete the WEB-IISS. NPC medical staffs were provided with unique usernames and passwords to access the WEB-IISS. Members of the research team visited every athlete medical station at the competition venues and spoke directly with each station's Venue Medical Officer and other LOCOG medical personnel. The research team emphasised to the LOCOG staff the importance of completing all pertinent data fields on the medical encounter forms, including non-mandatory fields. Each athlete medical station was provided with both an electronic and hard copy list of the important fields to improve data capture.
The research team made every effort to communicate frequently with the NPC medical personnel about the importance of the project and the need to have all delegations that brought medical staff to the Games complete the WEB-IISS daily. Compliance with completing the WEB-IISS was monitored on a daily basis through an automated, electronic compliance-reporting programme. Communications with NPC medical personnel were made in person, by email and by telephone.
In this study ‘injury’ is defined as any sport-related musculoskeletal or neurological complaint prompting an athlete to seek medical attention, regardless of whether or not the complaint resulted in lost time from training or competition. ‘Acute traumatic injury’ included any musculoskeletal or neurological complaint that started at a single, identifiable point in time (eg, due to a collision, fall or acute tissue overload). ‘Acute on chronic injury’ included any musculoskeletal or neurological complaint that an athlete had prior to the Games, with subsequent exacerbation of the same symptoms during the study period. ‘Chronic (overuse) injury’ included any injury that did not have an identifiable acute or traumatic onset and was due to repetitive overload of soft tissue or bone. Injury ‘severity’ data, mechanism of injury and other clinical data were only available from the WEB-IISS and not the EMDCS. Therefore, these data could not be included in this analysis and will be reported in future.
The period of data collection was 14 days, from 27 August through 9 September 2012. This included 11 days of the competition period and 3 days of the precompetition period.
In summary, a total of 4176 athletes from 164 delegations competed at the Games. Four delegations elected not to participate in the study. Although no exposure data and no WEB-IISS surveys were available from these delegations, none of the athletes from these four countries were included in the analysis. Thus, 3565 athletes (84% compliance by athletes) from 160 delegations (98% compliance by delegation) participated in the study. A total of 49 910 athlete-days were monitored for the purposes of this study. The calculation of athlete-days is explained elsewhere.28
Eighty-two delegations with a total of 236 athletes did not bring their own medical staff to the Games, and did not use the medical staff of another delegation. Seventy-eight delegations with 3329 athletes either had their own medical staff or shared the medical staff of another country that spoke the same language.
Statistical analysis
The statistical analyses completed in this study are individual-level descriptive analyses. Injury IRs and 95% CI were estimated based on frequency of injuries reported (ie, overall, by sex, by age group, by sport and by anatomical region) and total number of athletes-days of participation (estimated based on the total number of athlete-days for each delegation). The incidence proportion (IP) of injuries (95% CI) have been reported as the number of injuries per 100 athletes.
Results
Overall incidence of injuries (total period)
A total of 633 injuries in 539 athletes were documented during the period of the study. Among the 78 delegations that brought their own medical personnel to the Games, 123 injuries were captured in the LOCOG database and 458 injuries were captured in the WEB-IISS. Among the 82 delegations that did not have access to their own medical support, 52 injuries were captured in the EMDCS database and no injuries were captured in the WEB-IISS. The overall IR was 12.7 injuries/1000 athlete-days (95% CI 11.7 to 13.7). The overall IP was 17.8 injuries/100 athletes (95% CI 16.5 to 19.0). Eighty-one injured athletes (15%) presented with more than one injury. Of these multiple injuries, 32% occurred within 2 days of each other; 72% occurred within 5 days and the all injuries occurred within 11 days of each other.
Incidence of injuries by sex, age and time period (precompetition and competition)
The incidence and proportion of all injuries by sex and age for the total study period, the 3-day precompetition period and the 11 day competition period have been summarised in table 1. There were 1218 female athletes (34.2%) and 2347 (65.8%) male athletes. Among female athletes, there were 196 injuries (IR=11.5 injuries/1000 athlete-days (95% CI 9.9 to 13.2)). Among male athletes there were 437 injuries (IR=13.3 injuries/1000 athlete-days (95% CI 12.1 to 14.6)). The female IP was 16.1 injuries/100 athletes (95% CI 14.0 to 18.2) and male IP was 18.6 injuries/100 athletes (95% CI 17.0 to 20.2). There was no significant difference in the incidence of injuries in female compared with male athletes.
The median age of all athletes was 30 years (range 13–67). The median age of injured athletes was 30 years (range 15–56). To determine the relationship between age on injury rates, athletes were divided into three age groups as follows:<25 (n=1142), 26–34 (n=1249) and >35 (n=1174). By age group, the highest IR was in the middle tertile (ages 26–34; IR=14.5 injuries/1000 athlete-days (95% CI 12.8 to 16.4)) compared with the youngest tertile (ages 13–16; IR=11.3 injuries/1000 athlete-days (95% CI 9.7 to 13)) and the oldest tertile (ages 35–67; IR=12.1 injuries/1000 athlete-days (95% CI 10.5 to 13.9).
The overall IR of injuries was not different between the precompetition and the competition periods (table 1). However, for women the Precompetition rate of 16.7 (95% CI 12.8 to 21.4) is significantly higher than the competition period rate of 10.1 (95% CI 8.4 to 11.9).
The incidence rate (IR) of all injuries by sex and age for the total study period, the 3-day precompetition period and the 11-day competition period
Incidence of injuries by sport for the total period
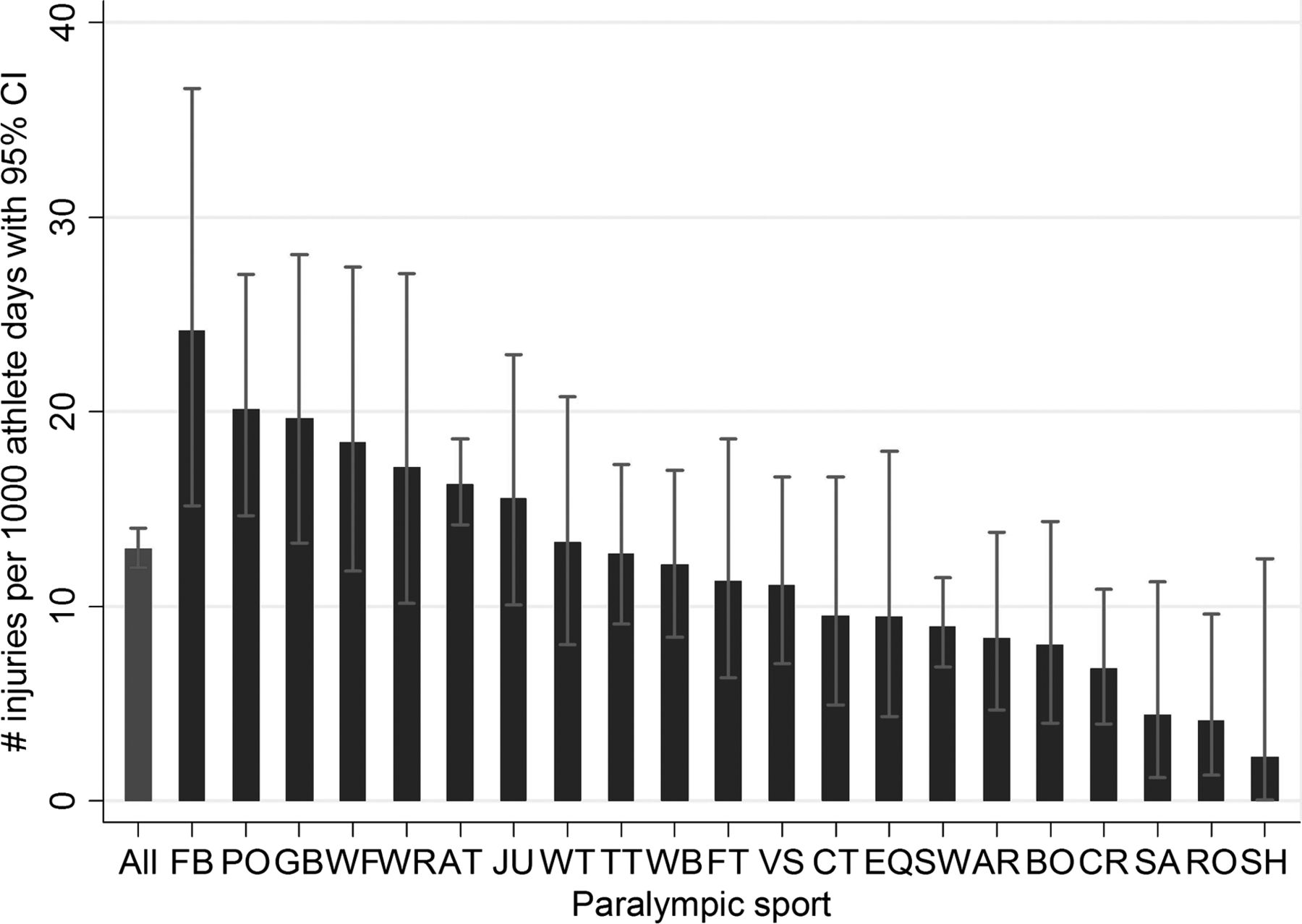
The IR of injury in each sport and the (IP in each sport in the total period are depicted in table 2. The IR of injury per sport is summarised in figure 1. The highest IR was found in football 5-a-side, followed by powerlifting, goalball, wheelchair fencing, wheelchair rugby, athletics and judo. The injury rates for football 5-a-side (IR 22.4) and powerlifting (IR 19.3) were higher than that of the overall injury rate (IR 12.7).

Sport-specific injury rates (injuries/1000 athlete-days). AR, archery; AT, athletics; BO, boccia; CR, cycling road; CT, cycling track; EQ, equestrian; FB, football 5-a-side; FT, football 7-a-side; GB, goalball; JU, judo; PO, powerlifting; RO, rowing; SA, sailing; SH, shooting; SW, swimming; TT, table tennis; VS, seated volleyball; WB, wheelchair basketball; WF, wheelchair fencing; WR, wheelchair rugby WT, wheelchair tennis.
The incidence rate (IR) of injury in each sport and percentage of athletes injured in each sport in the total period
Incidence of injury by anatomical region for the total period
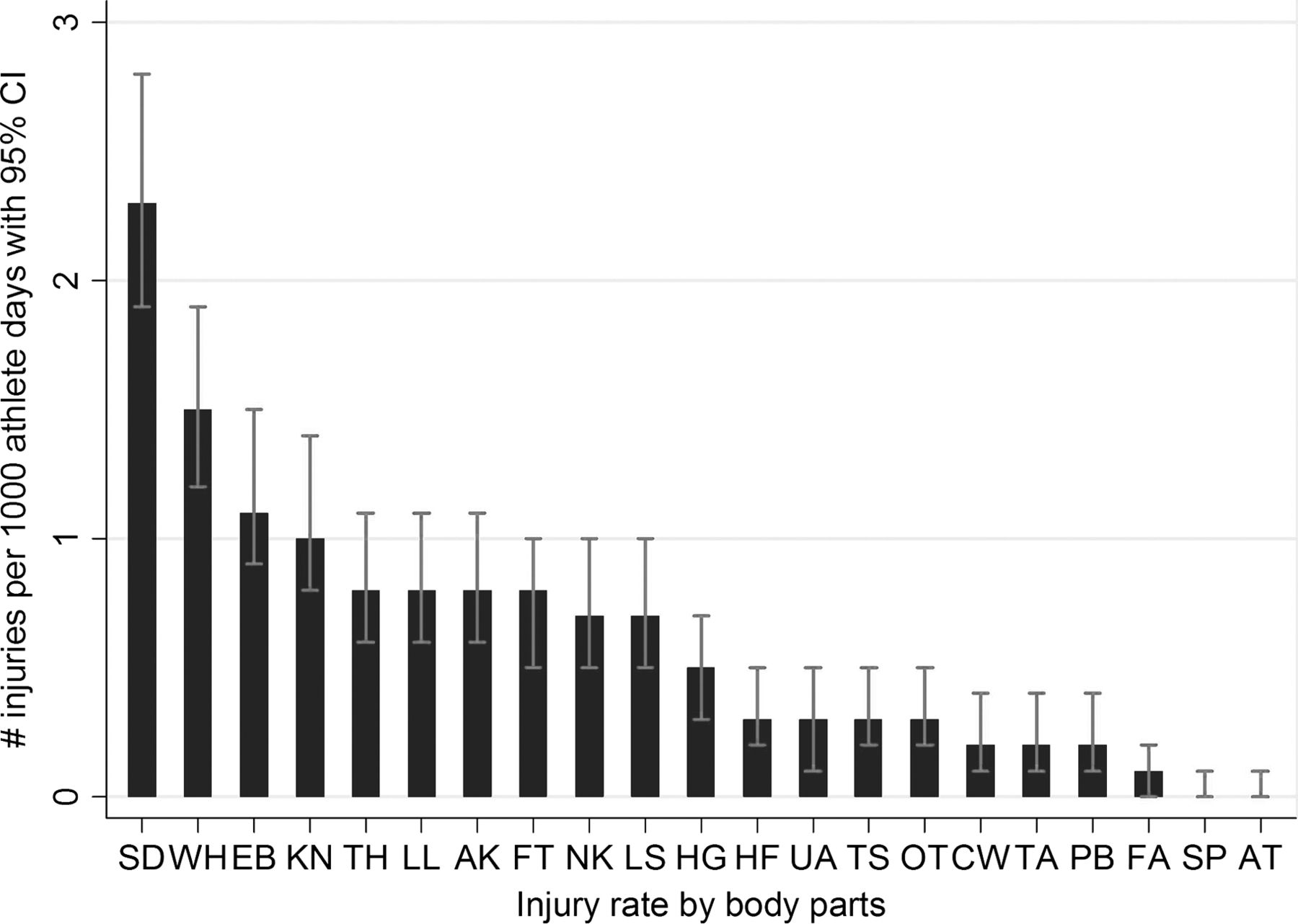
Injury rates by anatomical region are summarised in figure 2. There was a predominance of upper limb injuries, with the shoulder having the highest injury rate (IR=2.3 injuries/1000 athlete-days (95% CI 1.9 to 2.8)), followed by wrist/hand (IR=1.4 injuries/1000 athlete-days (95% CI 1.2 to 1.8)) and elbow (IR=1.1 injuries/1000 athlete-days (95% CI 0.8 to 1.5)). The knee was the most commonly injured area of the lower limb (IR=1.0 injuries/1000 athlete-days (95% CI 0.7 to 1.3)). The number and percentage of injuries by anatomical region are summarised in table 3. There was a predominance of upper limb injuries (50.2% of upper limb injuries out of all injuries), with shoulder injuries being most prominent (17.7% of all injuries), followed by wrist/hand injuries (11.4% of all injuries) and elbow injuries (8.8% of all injuries). The knee was the most common injured region of the lower limb (7.9% of all injuries).
The number and percentage of injuries per anatomical region
{kind=link}
{kind=link}
Injury rates (injuries/1000 athlete-days) by anatomical region. AK, ankle; AT, Achilles tendon; CW, chest wall; EB, elbow; FA,f; FT, foot; HF, head and face; HG, hip/groin; KN, knee; LL, lower leg; LS, lumbar spine; NK, neck; OT, other; PB, pelvis/buttock; SD, shoulder; SP, stump; TA, trunk and abdomen; TH, thigh; TS, thoracic spine; UA, upper arm; WH, wrist/hand.
Injury patterns by onset of injury (acute, acute-on-chronic and chronic) for the total period
Acute traumatic injuries accounted for 51.5% of all injuries captured. Chronic overuse injuries accounted for 31.8% of all injuries, and acute on chronic accounted for 16.7% of all injuries. The breakdown of sport by onset of injury is summarised in table 4. The sports with the highest proportion of acute traumatic injuries were boccia (91%; acute:chronic is 10 times), goalball (77%; acute:chronic is 7 times) track cycling (75%; acute:chronic is 3 times), football 7-a-side (73%; acute:chronic is 13 times) and road cycling (71%; acute:chronic is 5 times). The sports with the highest proportion of chronic (overuse) injuries were powerlifting (61%: chronic: acute is 1.5 times) followed by wheelchair fencing (58%; chronic:acute is 1.4 times).
Number and onset of injuries by sport, as a proportion (%) of all injuries incurred in each sport
Discussion
The IPC is dedicated to improving the safety of Paralympic sport, and pursues multiple courses of actions to decrease injury risk. Among these are educational initiatives and the continual process of refining competition rules and regulations on playing fields and equipment. The IPC also promotes sports science investigations that have the potential to improve the health and wellness of Paralympic athletes. The data presented in this study is one example of the IPC's efforts in this area. Injury surveillance and prevention may be even more important in adaptive sports than in able-bodied sports because the functional consequences of injuries can be more significant for an athlete with an impairment compared with the same injury sustained by an athlete without impairment.29–31
Prior to 2012, injury surveillance had only been completed during the Winter Paralympics, commencing with the Salt Lake City 2002 Winter Games.26 At the time, that study was the largest and most comprehensive reporting of injuries seen in athletes competing in Paralympic Sport. Analysis of injuries during the 2002 Games identified a high number of lower limb injuries in ice sledge hockey. This finding prompted rules changes to improve protection of the lower limbs. Following the rule changes, the Paralympic ISS documented a dramatic reduction in lower limb injuries during sledge hockey during both the 2006 and 2010 Paralympic Games compared with the 2002 Games.,26 ,32 This small but important success provided the impetus to conduct the Paralympic ISS at the Summer Games for the first time in London. The size and scope of the Summer Paralympics are much larger than the Winter Paralympics, with approximately 10 times as many athletes competing in four times as many sports. Prior to the London Games, the resources required to conduct an injury surveillance project on such a large scale were not available.
There are several important findings in the present study. Among Paralympians participating in the summer Games, the overall IR is 12.7/1000 athlete-days and the IP is 17.8/100 athletes. Men and women have similar IRs and IPs for injury. One particular interesting finding is that Paralympians in the youngest age tertile have marginally lower injury rates than athletes in the middle but not the older age tertiles. These data need to be analysed in greater detail, taking into account that the IPC and the various sport federations continue to consider minimum age limits for competition.
Overall, injury rates were not higher in the competition period compared with the precompetition period. However, for women there was a significantly higher injury rate in the precompetition compared with the competition period. The precise reason for this is not clear and requires further investigation but it could be related to a number of factors including; increased availability of medical facilities at the polyclinic, anxiety regarding minor precompetition symptoms, and increased training loads. However, the clinical implication is that medical staff should be aware that injuries are reported as frequently during the preparation phase before competition as during the competition.
The IRs and IPs for injury are sport specific, and the highest rate of injury was found in football 5-a-side (played by athletes with visual impairment), powerlifting, goalball, wheelchair fencing, wheelchair rugby, athletics and judo. Future injury prevention interventions should initially target these higher risk sports. The IR and distribution of injuries is similar to prior reports.9 ,33
A novel finding of this study was the preponderance of upper limb injuries in Paralympic athletes, particularly to the shoulder, wrist and elbow. This is not surprising, given that wheelchair athletes rely on their shoulders for all mobility, and there are fewer functioning lower limbs in competition than upper limbs owing to the nature of impairments seen in some of these athletes. In the lower limb, the knee was the most commonly injured area.
These data have direct clinical relevance. A clinician travelling to a 10-day event with 100 Paralympic athletes can anticipate seeing about 12–13 injuries, about half of which will be new onsets, acute injuries. If the team composition includes athletes participating in the higher risk sports listed above, it is likely that the team will incur more than 12–13 injuries. The clinician should be ready to diagnose and treat a high percentage of upper limb injuries, depending on the spectrum of the athletes’ impairments. Although different study methodologies have been used in past studies, the percentage of acute traumatic injuries during these Games is similar to what has been previously reported.9
Strengths and limitations
There are several strengths to this study. First, it is the largest study to date reporting on injuries in Paralympic athletes. Second, exposure data in terms of athlete-days was captured, providing the ability to report injury IRs and not only injury IPs. Third, the addition of a custom-built, web-based survey provided the ability to capture injury information in greater detail than is possible using the standard medical encounter form alone. Finally, there was very good compliance with 98% of delegations and 84% of athletes participating.
This study faced many of the same limitations encountered by prior injury epidemiology studies at major competitions. One limitation of the study is the inability to ensure complete data entry for every injury. For example, the medical encounter forms used at the LOCOG medical stations did not include important injury details such as injury severity, injury mechanisms and also contained non-mandatory fields. Therefore, they could be submitted with empty data fields. Another limitation of the study is the inability to ensure that the NPC medical personnel reported every injury that they saw in the WEB-IISS. If the NPC medical staff did not record all injuries in the web-based survey, this would result in an underestimate of the IR. Although efforts were made to translate injury capture forms in several languages, for some delegations language may have presented an additional barrier.
Another limitation of the study is the imprecise nature of ascertaining injury severity. The primary measure of injury severity was estimated by the evaluating medical personnel as the number of training and competition days lost. We are aware of cases where the medical professional estimated several days or longer of time loss, yet the athlete competed the very next day, at times even winning a medal. Thus, the reported injury severity may overestimate the actual time loss of the injuries. However, because we were unable to obtain follow-up information on the athletes following the end of the Games, the error in the estimate of severity cannot be determined with certainty.
An additional limitation concerns the challenges of analysing injuries by athlete classification status. Classification is the system whereby athletes with a disability are placed in different competition groups according to various factors such as their clinical diagnoses, impairments and functional status. Athlete impairment types are known to affect injury characteristics.34 However, there are over 110 separate classifications across the 20 summer Paralympic sports. Different sports utilise different types of classification methods and many of the classification systems are frequently modified. Finally, it was not possible to gather information on the impairments of injured athletes through the EMDCS used at LOCOG medical stations, which limits interpretation of data. For all of these reasons, it is not currently realistic to make comparisons of injuries across classification groups.
Finally, while participation in the study was good, there were still four delegations that chose not to participate. The IPC will continue to make efforts to engage the participation of all delegations at the Games.
Conclusions
The Paralympic Injury Surveillance Study was successfully carried out during the 2002, 2006 and 2010 Winter Paralympic Games. This study is the first comprehensive, prospective cohort study of injuries at the Summer Paralympic Games, and the largest Paralympic injury surveillance study undertaken to date. It is also the first time that exposure data was captured for all athletes at the Paralympic Games. Compliance on the part of the many health professionals who contributed to data collection was high. The use of a novel, web-based injury survey improved the ability to obtain detailed information about injuries. The incidence of injuries at the London 2012 Summer Paralympic Games is relatively low at 12.7/1000 athlete-days. The IPC will continue to conduct longitudinal injury and illness surveillances at future Paralympic Games in order to improve the medical care of athletes and implement safety initiatives. Additional research will focus on identifying risk factors for and mechanisms of injury in Paralympians.
What are the new findings?
-
Male and female Paralympic athletes have similar injury rates.
-
Injury rates are the lowest in the younger athletes.
-
Overall injury rates are similar in the precompetition and competition periods of the Games; in female athletes, higher precompetition injury rates are documented.
-
Slightly more than half of all injuries seen at the Summer Paralympics are new onset, acute injuries.
-
Injury rates differ by sport, with the highest rates of injury found in football 5-a-side, followed by powerlifting, goalball, wheelchair fencing, wheelchair rugby, athletics and judo.
How might it impact clinical practice in the near future?
-
Clinicians taking care of athletes with impairment should anticipate treating a high proportion of upper limb injuries, particularly shoulder injuries.
-
Clinicians taking care of athletes with an impairment can anticipate higher injury rates in certain sports (eg, football 5-a-side, powerlifting, goalball, wheelchair fencing, wheelchair rugby, athletics and judo).
-
The use of custom-built, web-based injury surveillance systems facilitates improved data collection methodology and compliance in sport epidemiology research.
Acknowledgments
The authors wish to extend their deepest gratitude to all members of LOCOG medical services who assisted with the data collection. LOCOG Chief Medical Officer Dr Richard Budgett was particularly instrumental in facilitating the study. The authors also thank all the NPC medical personnel who participated in data collection. Special recognition is deserved by Dr Harry Benjamin-Laing, Janey Orr and Greg Vice. They also thank Acer for donating 20 computer tablets as incentive to team physicians for their participation. This study was approved and supported by the International Paralympic Committee.
References
Footnotes
-
Contributors All the authors contributed in a substantial manner to the planning and conduction of the testing, literature review and/or manuscript preparation.
-
Funding No specific grant funding was obtained for this research project. However, financial support for this study was received from the IOC Research Centre in Cape Town. Members of the Medical Committee of the International Paralympic Committee receive travel expenses for the period of the Paralympic Games. There are no other relevant financial disclosures.
-
Competing interests None.
-
Ethics approval University of Brighton, UK.
-
Provenance and peer review Not commissioned; internally peer reviewed.
-
Data sharing statement This study is a collaborative effort between the International Paralympic Committee (IPC), the IPC Medical Committee and researchers from the University of Calgary and University of Cape Town. A Memorandum of Understanding was signed by all authors prior to the start of the study. Additional unpublished data from the study, which resides in secured servers at the IPC Headquarters in Bonn and the University of Cape Town, is available to all signatories to the memorandum of understanding.
-
▸ References to this paper are available online at http://bjsm.bmj.com