Article Text

Abstract
Background/aim The main purposes of this study were to determine the injury incidence and severity in Australian amateur taekwondo athletes, and to investigate potential risk factors for injury in competition taekwondo.
Methods Data were collected at New South Wales State Championships in 2010 and 2011. Injuries were diagnosed by onsite sports medicine personnel and the actual number of days lost from full participation was used to determine injury severity. Injury incidence rates were calculated per 1000 athlete-exposures (injury incidence rate (IIRAE)) and per 1000 min of exposure (IIRME) and presented with 95% CI.
Results The overall IIRAE and IIRME were 59.93 (95% CI 51.16 to 69.77) and 16.32 (95% CI 13.93 to 19.00), respectively. Children under 10 years had significantly lower IIRAE compared with older age groups and black belts had significantly higher IIRAE compared with yellow belts, however, after accounting for the exposure time it was revealed that 10-year-olds to 14-year-olds and red belts incurred higher IIRME. This study highlights the importance of including IIRs that account for exposure-time. In contrast with previous estimates, the current data indicated that one-third of injuries were moderate to severe. Relative to other body regions the upper limb had a higher proportion of moderate-to-severe injuries, and compared with the lower limb there was a disproportionate number of upper limb injuries resulting in fractures.
Conclusions The findings suggest that the impact of injury on taekwondo athletes is significant, and should serve as an impetus to stakeholders to develop and implement injury prevention activities within the sport.
- Sporting injuries
- Martial Arts
- Injury Prevention
Statistics from Altmetric.com
Introduction
Modern taekwondo is an amalgamation of unarmed combat styles originating from the Korean peninsula. Over the last half-century taekwondo has grown in popularity, and has arguably become the most commonly practised martial art in the world.1 ,2 Taekwondo is characterised by its emphasis on dynamic kicking techniques delivered from a mobile stance. Agility, strength, speed, balance, flexibility, coordination and stamina are all important attributes for a taekwondo athlete to be able to execute the highly demanding kicking combinations.1 The competition rules and regulations for Olympic-style taekwondo, which are governed by the World Taekwondo Federation, allow full-contact kicking techniques to the head and torso and punches to the front of the torso.3 Athletes are required to wear protective gear during bouts (fights), including: trunk protector, head protector, groin guard, forearm and shin guards, mouthguard and gloves.
Although the positive effects of regular physical activity are undisputed, participation in sport and active recreation are not without risk and injuries can be an adverse outcome. Indeed, sport injury is identified as a major public health problem in the Western world,4–7 accounting for 19–59% of all injuries in children.8 It is estimated that 8% of youths discontinue active recreation and sporting activities annually because of injury, which may lead to a loss of health benefits in the future.9 Many risk factors may predispose athletes to injury, even before the inciting event,10 hence identification of risk factors is paramount to developing effective risk mitigation strategies.
As in any contact sport, there is an inherent risk of injury to practitioners of combative martial arts such as taekwondo, and the aim of any sport should be to keep the risk acceptable. In a review of the literature, Pieter summarised injury incidence data from 10 prospective studies, most of which arose from elite-level athlete populations. Individual studies suggested that certain subpopulations of taekwondo athletes incur injuries at a higher rate,11 for example, junior females >adult females,12 females >males12 ,13 and young males >young females.14 However, the data appeared to be conflicting, and in a systematic review with meta-analysis, Lystad et al1 found no evidence that gender, age or belt rank had any significant effect on overall injury occurrence. Further research with sufficient power seems necessary to get a clearer picture of the injury risk in various subpopulations, and to identify opportunities for prevention.
There is a seeming paucity of data on injury severity in taekwondo. Pieter summarised the findings from four studies reporting time-loss from participation and concluded that the majority of taekwondo competition injuries resulted in less than 1 week of restricted participation.11 ,15–18 Lystad and colleagues provided a descriptive analysis of two additional studies that reported on injury severity.1 ,19 ,20 Despite recommendations to include recording of actual time-loss,1 ,21 ,22 all of the aforementioned investigations have relied on time-loss estimates based on the type of injury. Thus, there is a need for research that measures injury severity in terms of actual, as opposed to estimated, time-loss from participation.
The main purpose of this study was to determine the injury incidence and severity in Australian amateur athletes competing in taekwondo. Secondary aims included identifying risk factors for injury, such as age, gender and level of experience.
Methods
Data collection
Injury and exposure data were collected from Australian amateur taekwondo athletes competing at six consecutive New South Wales (NSW) State Championships in 2010 and 2011. The athletes were appropriately matched according to age (2-year intervals for those under 18), weight (3–6 kg intervals depending on age) and belt rank (yellow, blue, red or black). Match lengths by age category and belt rank are provided in online supplementary table A. Injury data were recorded onsite by a team of trained research assistants using a simple check-off injury reporting form. The form included information about age, gender, skill level, weight division, mechanism of injury and injury diagnosis. Belt rank was used as a proxy for skill level, that is, yellow<blue<red<black. All injuries were diagnosed by official tournament sports medicine personnel, and subsequently recorded according to the Orchard Sports Injury Classification System, V.10 (OSICS-10) by trained research assistants.
This study adhered to the operational injury definitions recommended by Lystad et al.1 Thus, an injury was defined as any physical complaint for which an athlete would seek assistance from tournament medical personnel. Injury severity was defined in terms of the number of days that have elapsed from the date of injury to the date of the athlete's return to full participation in training and match play. Actual time-loss was determined by conducting post-tournament follow-up telephone interviews of all injured athletes. Injuries were categorised as: slight (0–1 days), minimal (2–3 days), mild (4–7 days), moderate (8–28 days) and severe (>28 days). The unit of exposure was defined as a single taekwondo fight. Thus, one athlete-exposure (AE) was defined as one athlete participating in one taekwondo fight. The actual duration of a single fight varied between 2 and 6 min depending on age and belt division. Hence, 1 min of exposure (ME) was defined as one athlete participating in a taekwondo fight for the duration of 1 min. All exposure data were gathered from official tournament records.
Written informed consent was obtained from athletes during the weigh-in sessions prior to the start of the tournaments. This study was approved by the Macquarie University Human Research Ethics Committee.
Data analysis
Injury incidence rates (IIRs) per 1000 AEs (IIRAE) and per 1000 MEs (IIRME) were calculated using standard methods. Subpopulations were compared by computing the rate ratio (RR) of two IIRs. The relative risk of incurring upper-extremity fractures versus lower extremity fractures was calculated by dividing the proportion (number of fractures/number of injuries) of upper extremity fractures with the proportion of lower-extremity fractures. Ninety-five per cent CIs were computed for all IIRs, RRs and relative risks using standard formulae for Poisson rates and binomial proportions.23 ,24 The CIs for RRs and relative risks were used to determine whether two rates or proportions differed significantly from one another, that is, two IIRs were deemed statistically different from one another if the CI for their RR did not include the number 1. Poisson mixed-effects generalised linear modelling was also used to examine the multivariate relationships between IIRs and potential risk factors (age, weight, gender and belt rank). The mixed-effects model used a random intercept for each athlete to account for the correlation induced by multiple observations of the same person. All statistical modelling was performed using Stata IC 12.25
Results
The six NSW State Championships included 2112 tournament-entries (635 women and 1447 men), and comprised a total of 2770 AEs, 10 173MEs, and 166 injuries. Frequencies and proportions of tournament-entries by gender, age category and belt rank are provided in online supplementary table B, and a cross-tabulation of tournament-entries by age category and belt rank is provided in online supplementary table C. The overall IIR per 100 tournament-entries, IIRAE and IIRME for Australian amateur taekwondo athletes were found to be 7.86 (95% CI 6.71 to 9.15), 59.93 (95% CI 51.16 to 69.77) and 16.32 (95% CI 13.93 to 19.00), respectively.
Table 1 provides an overview of the distribution of injuries by anatomical location. Within both the upper and lower extremities the vast majority of injuries were found to occur in the distal portion of the limbs, that is, wrist and hand for the upper extremity, and foot, ankle and shin for the lower extremity. Table 2 presents an overview of the distribution of injuries by injury type. Of the eight fracture injuries that were recorded, four were located in the upper extremities and two were located in the lower leg (see online supplementary table D). The relative risk of upper-extremity fractures versus lower extremity fractures was found to be 9.90 (95% CI 2.12 to 46.20), which suggests that a significantly disproportional number of upper limb injuries result in fractures in comparison with the lower limb. Table 3 shows the distribution of injuries by mechanism of injury.
Distribution of injuries by anatomical location per 1000 athlete-exposures (IIRAE) with 95% CIs
Distribution of injuries by injury type per 1000 athlete-exposures (IIRAE) with 95% CIs
Distribution of injuries by mechanism of injury per 1000 athlete-exposures (IIRAE) with 95% CIs
A total of 150 injuries were followed up post-tournament to determine the actual number of days lost from full participation. The remaining injuries (N=16) were lost to follow-up due to either missing or incomplete contact information, or because athletes did not consent to be contacted post-tournament. Table 4 provides an overview of the distribution of injuries by the degree of severity. Figure 1 shows the proportion of injuries resulting in less than 1 week and more than 1 week by anatomical region. The upper limb was found to have a higher proportion of injuries resulting in more than week lost from full participation relative to other body regions. However, a significant difference was only detected when compared with the head and neck region (relative risk 4.17 (95% CI 1.38 to 12.55)). There were no significant differences in the proportion of injuries resulting in less than 1 week and more than 1 week by neither gender nor belt rank. However, the comparison of age groups revealed that the under 10 age group incurred significantly fewer moderate and severe injuries compared with all other age groups except for 10-year-olds to 14-year-olds (figure 2). Contusions dominated both the less severe and more severe injuries. Of the 108 contusions with accompanying injury severity data, 26 (24.1%) were found to result in more than 1 week of lost or restricted participation (see online supplementary table E).
Distribution of injuries by injury severity per 1000 athlete-exposures (IIRAE) with 95% CIs

Proportions of injuries resulting in less than 1 week and more than 1 week of restricted participation by anatomical region. Injury proportions were deemed significantly different when the CI of their relative risk did not include 1 (asterisk).

Proportions of injuries resulting in less than 1 week and more than 1 week of restricted participation by age group. Injury proportions were deemed significantly different when the CI of their relative risk did not include 1 (asterisk).
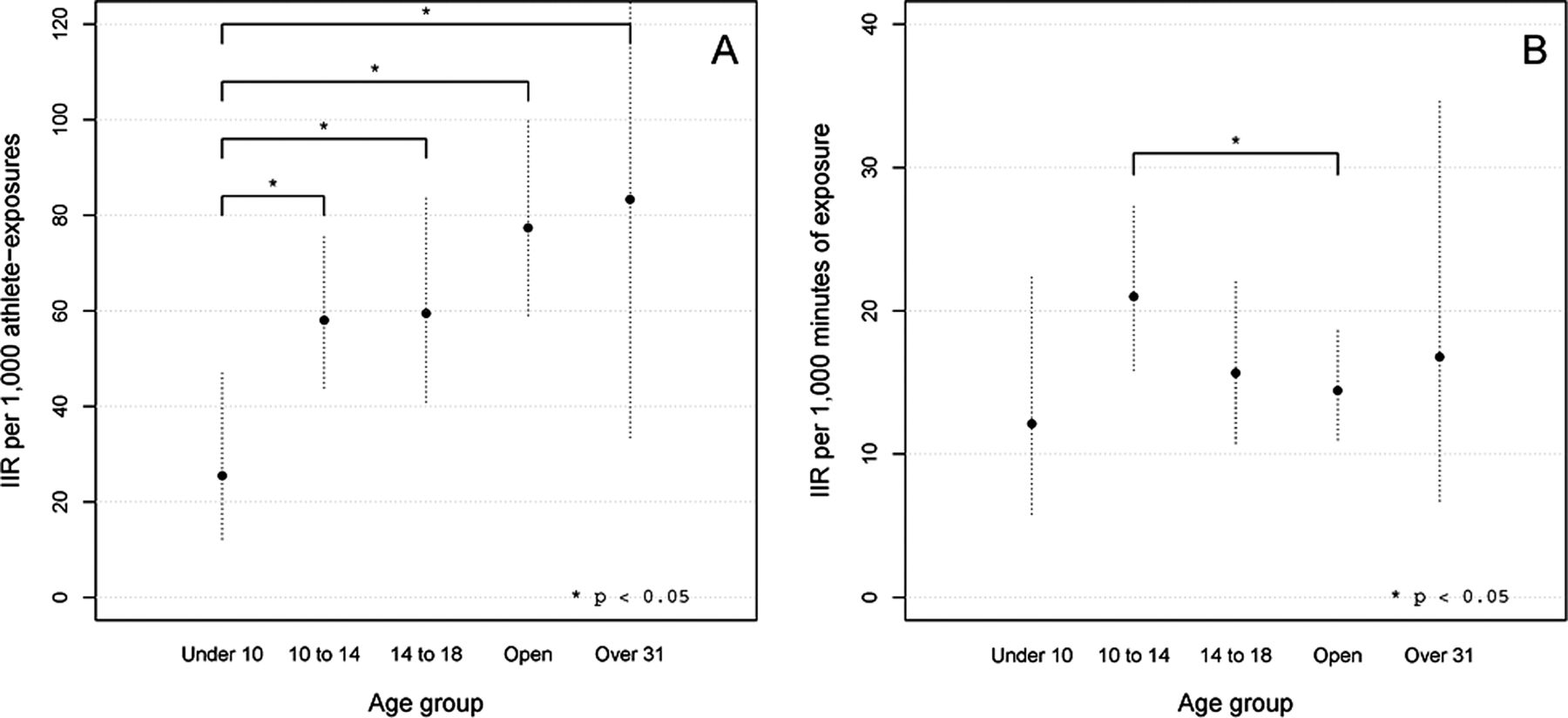
Table 5 provides an overview of IIRs and RRs of potential risk factors (ie, gender, age group and belt rank). There appeared to be a positive relationship between higher belt rank and increases in IIRAE (figure 3A), with black belts having a significantly higher IIRAE compared with yellow belts (RRAE 1.78 (95% CI 1.13 to 2.82)). However, after adjusting for exposure-time (ie, comparing IIRME rather than IIRAE), there was no longer any significant difference between yellow and black belts (RRME 1.06 (95% CI 0.67 to 1.67); figure 3B). Rather, there was a trend indicating red belts having higher IIRME, albeit only significant when compared with black belts (RRME 1.50 (95% CI 1.02 to 2.19)). Similarly, there appeared to be a positive relationship between older age groups and increases in IIRAE (figure 4A), with the under 10 years age group having a significantly lower IIRAE compared with all other age groups. Again, after adjusting for the exposure-time there was a trend indicating that the 10–14 age group had a higher IIRME, albeit only significant when compared with the open division (RRME 1.45 (95% CI 1.01 to 2.09)).
Injury incidence rates (IIRs) and rate ratios (RRs) per 1000 athlete-exposures (AE) and 1000 minute-exposures (ME) with 95% CIs by gender, age and belt rank categories

Injury incidence rates (circles) with 95% CIs (dashed lines) by belt rank. Injury incidence rates were deemed significantly different when the CI of their rate ratio did not include 1 (asterisk).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Injury incidence rates (circles) with 95% CIs (dashed lines) by age group. Injury incidence rates were deemed significantly different when the CI of their rate ratio did not include 1 (asterisk).
Age and weight were treated as continuous variables in the Poisson mixed-effects generalised linear modelling and were found to be highly correlated so that both could not be included at once in the model. A slightly better fit was achieved by using weight rather than age in the models. Table 6 contains the results from the final fitted models, which essentially confirmed the findings from the univariate analyses, that is, black belts had higher IIRAE (p=0.045) but not IIRME (p=0.712) compared with yellow belts.
Rate ratio estimates per 1000 athlete-exposures (RRAE) and 1000 minute-exposures (RRME) with 95% CIs using Poisson mixed-effects generalised linear modelling
Discussion
This is the first study to measure injury severity in terms of actual, as opposed to estimated, time-loss from participation; and in contrast to what has previously been suggested, the current data indicated that one-third of injuries were moderate to severe. Relative to other body regions the upper limb had a higher proportion of moderate-to-severe injuries; and compared with the lower limb a disproportionate number of upper limb injuries result in fractures. This study highlights the importance of including exposure-time adjusted IIRs because significant differences in IIRAE found among various subpopulations were not maintained after accounting for the exposure time.
Injury incidence
The overall IIRAE in the current study (59.93 (95% CI 51.16 to 69.77)) was lower than the rate Lystad et al1 reported in their systematic review with meta-analysis (79.3 (95% CI 22.8 to 275.4)). A possible explanation may be that most of the data included in the meta-analysis was derived predominantly from elite athlete populations, whereas this study investigated amateur athletes. The reason for this difference is unclear, but may be associated with elite athletes’ ability to generate larger forces or their willingness to take larger risks when competing at a higher level. Caution should be exercised when comparing the findings from different studies as study design and methodology may vary considerably across studies. Moreover, rule changes may be implemented from time to time, generally without any research to investigate the actual effects of the implemented changes.
Both the distribution of injuries by anatomical location and by type of injury were aligned with the trends reported in previous literature reviews,1 ,11 that is, lower-limb injuries and contusions were the most common, respectively. The vast majority of peripheral injuries occurred in the distal parts of upper and lower extremities, which is to be expected considering these are the principal areas of contact when blocking or delivering blows. In comparison with lower-limb injuries, a disproportional number of upper-limb injuries result in fractures. Considering that upper-limb structures are more delicate than the heavier and more robust lower-limb structures, it is perhaps to be expected that more fractures occur in the upper extremity compared to the lower extremity. In addition, it is also worth considering the fact that while the upper limb predominantly receives blows, the lower limb predominantly delivers blows.
Injury severity
In a review of the literature, Pieter11 concluded that the majority of competition time-loss injuries led to more than 1 week of restricted taekwondo participation, however all previous studies have relied on time-loss estimates, rather than actual measurements of the number of days lost from full participation in training and match play, and the findings from these studies should therefore be interpreted with caution. The current study found that 32% of injuries result in more than 1 week time-loss. This suggests that the impact of injury on taekwondo athletes is significant, and it should serve as a strong impetus to implement injury prevention activities within the sport.
Relative to other body regions the upper limb had a higher proportion of injuries resulting in more than week lost from full participation. This finding is consistent with the disproportionate number of upper-limb fractures compared to lower-limb fractures described above, and similar arguments can be made when attempting to explain it. The predominance of moderate and severe injuries in the upper limbs, particularly in the distal parts, is a cause for concern considering the potential burden of these injuries. An injury to the dominate hand, for instance, may be associated with greater impairment of activities of daily living and loss of productivity (eg, lost time at work or school) compared with the same time-loss from a leg injury.
Risk factors
The available data on gender differences in the literature is at best conflicting. The present study found no difference in IIRs between men and women, which is consistent with the meta-analysis by Lystad et al.1 RR calculations revealed that the under 10-year-olds had a significantly lower IIRAE in comparison with all other age groups. This finding is consistent with the review by Pieter,11 which concluded that adults are at a higher risk of injury compared with children. However, because the actual duration of an exposure varies across different age divisions, it is necessary to factor in the actual exposure time to make more meaningful comparisons. After adjusting for exposure time it was revealed that adults did not have significantly higher IIRME. On the contrary, the only significant difference was the 10–14 age group having a higher IIRME compared to adults (RRME 1.45 (95% CI 1.01 to 2.09)). Although it is not clear exactly why this age group is more vulnerable to injury, Caine et al26 suggested that children in the years of growth increase activity frequency and intensity levels as they begin to compete more intensely. Recently, Quatman-Yates et al27 discussed the possible role of immature sensorimotor mechanisms and/or regressions in sensorimotor function that coincide with this time frame, which could, at least in theory, create a period of higher vulnerability for injury. More research is needed to better understand why pubescent athletes have a greater risk of injury compared with both younger and older counterparts and to identify potential preventative strategies.
This study used belt rank as a proxy for level of experience or skill level. RR calculations revealed that black belts had a significantly higher IIRAE compared with yellow belts, however after accounting for exposure-time red belts were found to higher IIRME compared with black belts.
Moreover, Poisson mixed-effects generalised linear modelling revealed results similar to the univariate analyses. Taken together, the age group and belt rank findings presented herein highlight the importance of including exposure-time adjusted IIR calculations, and reiterates the recommendation by Lystad et al1 that future studies report injury incidence rates using multiple denominators. The findings presented above should aid in directing future research efforts to generate more knowledge about specific risk factors for injury in taekwondo, which may in turn lead to effective injury prevention strategies for the sport of taekwondo.
Limitations
This study only included data from NSW State Championships organised by Taekwondo Australia, which may limit the generalisability of the findings; however there are no obvious reasons why this cohort should be significantly different from those in other Australian states. For pragmatic reasons this study adopted a medical-attention injury definition, thus one can expect a number of injuries to go unreported. This may result in underestimating the actual risk of injury. Although all injuries were diagnosed by qualified health professionals, in the absence of advanced diagnostic technologies there is potential for misdiagnosis and misreporting. The findings reported above should be interpreted in the light of these limitations.
Conclusion
Both red belts and 10-year-olds to 14-year-olds had significantly higher IIRME, but not IIRAE, compared with other belt ranks and age groups, respectively. This highlights the importance of including IIRs that account for exposure-time. In contrast to previous estimates, the current data found one-third of injuries to be moderate to severe. Relative to other body regions the upper limb had a higher proportion of moderate to severe injuries, and compared with the lower limb a disproportionate number of upper-limb injuries resulted in fractures. The findings suggest that the impact of injury on taekwondo athletes is significant, and should serve as an impetus to stakeholders to develop and implement injury prevention activities within the sport.
What are the new findings
-
By measuring actual, as opposed to estimated, time-loss from participation, this study found that one-third of injuries in amateur competition taekwondo were moderate to severe.
-
Relative to other body regions, the upper limb had a higher proportion of moderate-to-severe injuries; and compared with the lower limb a disproportionate number of upper-limb injuries result in fractures.
-
Red belts and 10-year-olds to 14-year-olds have higher exposure-time adjusted injury incidence rates compared to other belt ranks and age groups, respectively.
How might it impact on clinical practice in the near future
The findings of this study suggest that the impact of injury on taekwondo athletes is significant, and should serve as an impetus to stakeholders to develop and implement injury prevention activities within the sport.
Acknowledgments
Taekwondo Australia (NSW), in particular Tournament Director Mr Matt Vale and Medical Team Manager Mr Tony Su, are thanked for their support and co-operation. All research assistants involved with collecting the data are thanked for their efforts.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Correction notice This article has been corrected since it was published Online First. The affiliation for the second author, Petra L Graham, was incorrect.
-
Contributors RPL substantially contributed to conception and design, data collection, analysis and interpretation of data; drafting the article and revising it critically for important intellectual content and final approval of the version to be published. PLG contributed to design, analysis and interpretation of data and revising the article critically for important intellectual content. RP was involved in interpretation of data and revising the article critically for important intellectual content.
-
Funding This research was supported by a grant (reference number 9201000) from the NSW Sporting Injuries Committee (Australia).
-
Competing interests None.
-
Ethics approval Macquarie University Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com