Article Text

Abstract
Purpose We describe exercise level in mid-pregnancy, associated sociodemographic variables, and investigate the association between exercise in mid-pregnancy and subsequent low-back pain, pelvic girdle pain and depression at 32 weeks of pregnancy.
Material and methods The study included 3482 pregnant women participating in the Akershus Birth Cohort study (response rate 80.5%). Data were collected by a questionnaire in pregnancy weeks 17–21, pregnancy week 32 and electronic birth journal. The results were analysed by logistic regression and are presented as crude (cOR) and adjusted OR (aOR) with 95% CI.
Results Only 14.6% of the respondents followed the current exercise prescription for exercise during pregnancy (≥3 times a week, >20 min at moderate intensity). One-third of the study sample exercised less than once a week at pregnancy weeks 17–21. Women exercising either 1–2 times or ≥3 times a week at mid-pregnancy were more often primiparous, higher-educated and had less often prepregnacy body mass index >30 kg/m2 compared with women exercising less than once a week. Women who exercised ≥3 times a week were less likely to report pelvic girdle pain (aOR: 0.76, 95% CI 0.61 to 0.96), while women exercising 1–2 times a week were less likely to report low-back pain (aOR: 0.80, 95% CI 0.66 to 0.97) and depression (aOR: 0.66, 95% CI 0.48 to 0.91).
Conclusions Few Norwegian women follow current exercise prescriptions for exercise in mid-pregnancy. The results may indicate an association between exercising mid-pregnancy and lower prevalence of low-back pain, pelvic girdle pain and depression in late pregnancy.
- Exercise
Statistics from Altmetric.com
Introduction
In the absence of medical or obstetrical contraindications, pregnant women are recommended to be physically active on most, if not all days, for at least 30 min of moderate intensity,1 ,2 or exercise 3–5 times a week for at least 15 min at moderate intensity progressing to 30 min.3 These exercise prescriptions are in line with current exercise recommendations for the general population.4 Exercise during pregnancy has been associated with health benefits. Studies have reported reduced risk of gestational diabetes,5 preeclampsia,6 improved maternal glucose tolerance,7 increased well-being, self-esteem plus fewer depressive symptoms,8 ,9 shorter duration of labour and higher prevalence of vaginal delivery.10
Pregnancy is related to significant changes in the musculoskeletal system with possible subsequent complaints. It has been claimed that virtually all women have some degree of musculoskeletal discomfort during pregnancy.11 ,12 Studies have demonstrated that low-back pain affects nearly 50% of all pregnant women13 and 20–45% experience pelvic girdle pain.14 ,15 Additionally, mood disturbances and depression are common in pregnant and postpartum women.16 Bennett et al17 reported a prevalence of depression of 7.4%, 12.8% and 12% in the first, second and third trimester, respectively. These conditions lead to a reduction in daily activity, lower quality of life and may lead to increased sick-leave.16 ,18 ,19
Knowledge considering exercise level during pregnancy and sociodemographic predictors of exercise behaviour is of public health importance. Previous studies often had low response rates.20–24 We found only two studies with response rates ≥80%.25 ,26 However, the external validity of these studies may be questioned, as both studies included women with higher educational levels compared to the general pregnant population.
Women participating in the Akershus Birth Cohort (ABC study) at Akershus University Hospital (Ahus) responded to questions regarding exercise in mid-pregnancy (pregnancy weeks 17–21; n=3751). The response rate for the study is >80%. This provides a unique opportunity to explore exercise in pregnancy. The aims for the present study were: (1) describe exercise-level mid-pregnancy; (2) examine sociodemographic variables associated with exercise and (3) analyse the association between exercise in mid-pregnancy and low-back pain, pelvic girdle pain and depression in pregnancy week 32, within a population-based group of pregnant Norwegian women. We hypothesised that women exercising in mid-pregnancy had less low-back pain, pelvic girdle pain and depression in late pregnancy.
Material and methods
The ABC study methods are detailed elsewhere.27 Briefly, Ahus is located near Oslo, the capital of Norway, and serves a total population of 400 000 from both urban and rural surroundings. On average, 4200 women give birth at the hospital each year. Women were recruited to the ABC study at the routine fetal ultrasound examination in pregnancy week 17, from November 2008 to April 2010. This examination is part of the public antenatal care programme, offered free of charge to all pregnant women in the hospital's catchment area. All pregnant women able to complete a questionnaire in Norwegian were eligible for the ABC study. There were no other exclusion criteria. The participants received one questionnaire at four different time points; between pregnancy weeks 17–21 (Q1), at pregnancy week 32 (Q2) and 8 weeks (Q3) and 2 years (Q4) postpartum. If the questionnaires were not returned within 2 weeks, at least one reminder was sent by mail. The questionnaires are linked to electronic birth records (PARTUS) with information regarding the woman, labour and the child. The study was approved by the Regional Committee for Ethics in Medical Research in Norway, and all participants provided informed consent (S-08013a).
Information on exercise level and parity were obtained in Q1, while other sociodemographic variables were retrieved from PARTUS. Information regarding low-back pain, pelvic girdle pain and depression were collected through Q2.
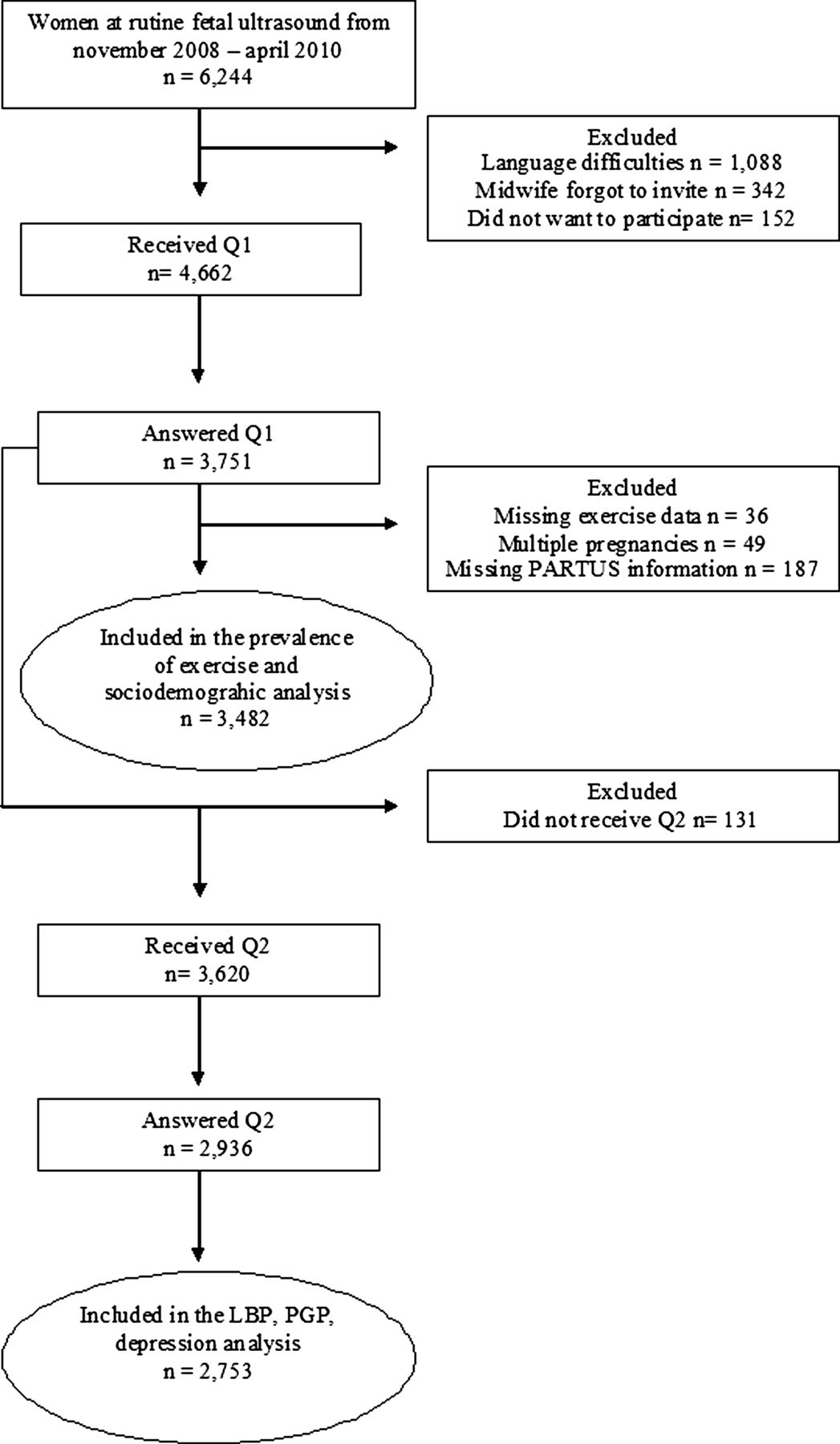
During the recruitment period, 4662 of 6244 women (74.7%) were included into the ABC study. Reasons for not participating were language difficulties (n=1088), midwife forgot to invite (n=342) and choose not to participate (n=152). Of the included women, 80.4% (n=3751) answered Q1. We excluded women with missing information regarding frequency of exercise during pregnancy (n=36), multiple pregnancies (n=49) and missing information in PARTUS (n=187) (three women had missing information on both exercise and PARTUS). Thus, 3482 women were included in the description of exercise levels, and the association between exercise in pregnancy weeks 17–21 and sociodemographic variables (figure 1).

{kind=link}
Flow chart of the participants.
Only women who returned Q1 received Q2. Furthermore, 3% (n=131) did not receive Q2 due to different reasons, for example, moving out of the area or perinatal death. Of the 3620 women who received Q2, 2936 responded. As we excluded women with missing exercise and PARTUS information and with multiple pregnancies, a total of 2753 women were included in the analysis of the association between exercise in pregnancy weeks 17–21 and low-back pain, pelvic girdle pain and depression in pregnancy week 32 (figure 1).
Variable specifications
Exercise
The three questions asked concerning frequency, intensity and duration of exercise were as follows: (1) after conception, how often do you engage in exercise (eg, brisk walking, skiing, commuting to work by bike and sports/exercise) (never, <once a week, once a week, twice a week, three times a week and ≥3 times a week); (2) if you engage in exercise, how strenuously do you exercise? (no sweating and normal breathing, modest sweating and light breathing, sweating and breathing heavily); (3) if you engage in exercise, for how long do you exercise? (10, 11–20, 21–60 and >60 min). Additionally, we categorised exercise by frequency of exercise into three groups: <once a week (never+<once a week), 1–2 times a week and ≥3 times a week.
Sociodemographic variables
Included sociodemographic variables that may influence exercise during pregnancy weeks 17–21 were as follows: age, parity (0, 1, ≥2), education (primary/secondary school versus college/university), marital status (single, cohabitant and unknown), smoking at the time when pregnancy started (smokers versus non-smokers) and prepregnancy body mass index (BMI) (<18.5, 18.5–24.9, 25.0–29.9, 30.0–34.9 and 35+). In this study, parity was defined as the number of previous births.
Low-back pain, pelvic girdle pain and depression
Low-back pain has been defined as pain between the 12th rib and the gluteal fold, with or without leg pain28 and the question asked was: ‘At present, do you experience any low-back pain?’ (yes versus no). Pelvic girdle pain has been defined as pain experienced between the posterior iliac crest and the gluteal fold, particularly in the vicinity of the sacroiliac joints. The pain may radiate in the posterior thigh and can also occur in conjunction with/or separately in the symphysis.15 The question asked was: ‘At present, do you experience pelvic girdle pain (in Norwegian: ‘Bekkenløsning’)?’ (yes versus no). Ability to separate low-back pain and pelvic girdle pain in questionnaires has previously been found by Bø and Backe-Hansen.29
The Edinburgh Postnatal Depression Scale (EDPS) was used to assess depression.30 The EDPS was developed to screen for depression in the postnatal period, but the scale has also shown good psychometric properties, and good test–retest reliability (0.81) in pregnant populations.31 It consists of a self-rating, 10-item scale, with a sum score ranging from 0 to 30. A cut-off of ≥12 was set to define depression.30
Statistical analysis
The statistical package SPSS Statistical Software V.15.0 was used for the statistical analyses. Sociodemographic characteristics of the study sample and exercise level are presented by numbers and percentages. Univariable and multiple logistic regression analyses were used to calculate the association between exercise and sociodemographic variables and low-back pain, pelvic girdle pain and depression. Women exercising <once a week (never+<once a week) was used as the reference group for the logistic regression analysis. On the basis of prior studies, we included known covariates in the adjusted regression analysis that may influence exercise during pregnancy and have an association with the included sociodemographic variables and low-back pain, pelvic girdle pain and depression. Sociodemographic variables with missing values were replaced by dummy variables and are included in the statistical analysis.
The results are presented as crude (cOR) and adjusted OR (aOR) with 95% CI. p Values of <0.05 were considered significant.
Results
Sociodemographic characteristics of the study sample are shown in table 1. Of the 3482 women included in the study, mean age was 31.1 (SD=4.8) years.
Sociodemographic characteristics of the participants (n=3482)
Exercise level in mid-pregnancy is reported in table 2. About one-third of the study sample exercised less than once a week. Approximately 40% exercised 1–2 times a week, while 26.6% exercised ≥3 times a week. A significant proportion were not sweating or out of breath when they exercised (39.1%). Most of the exercising women reported exercise bouts of >20 min (71.9%; table 2). A total of 14.6% followed the current guidelines for exercise during pregnancy and exercised ≥3 times a week at moderate intensity, for at least 20 min.
Frequency, intensity and duration of exercise in pregnancy week 17–21 (n=3482)
Women who exercised either 1–2 times or ≥3 times a week in pregnancy week 17–21 were more likely to be primiparous and have had more education (college/university) compared with women who exercised <1 a week.
Exercising 1–2 times a week was inversely associated with prepregnancy BMI between 30 and 35 kg/m2, while exercising ≥3 times a week were both inversely associated with prepregnancy BMI between 30–35 and 35 kg/m2 (table 3).
Association between exercising 1–2× per week and ≥3× per week in pregnancy week 17–21 and sociodemographic variables (n=3482)
Table 4 shows the regression analysis of the associations between exercise and low-back pain, pelvic girdle pain and depression. Of the 2753 women included in the analysis, 51.2%, 51.7% and 8.2% reported low-back pain, pelvic girdle pain and depression in pregnancy week 32, respectively. Women who were exercising ≥3 times a week in pregnancy weeks 17–21 were significantly less likely to experience pelvic girdle pain in late pregnancy, and there was a trend towards a dose–response relationship comparing exercising 1–2 times a week and ≥3 times a week. A significant association between exercising 1–2 times a week and lower prevalence of low-back pain and symptoms of depression was also found. These associations did not reach statistical significance regarding exercising ≥3 times a week (table 4).
Association between exercising 1–2× per week and ≥3× per week in pregnancy week 17–21 and low-back pain, pelvic girdle pain and depression in pregnancy week 32 (n=2753)
Discussion
In the present study, we demonstrated that only 14.6% of the respondents followed the current guidelines for exercise during pregnancy and one-third exercised less than once a week. Women who exercised were more likely to be primiparous, more highly educated and had less often prepregnacy BMI >30 kg/m2. A noteworthy proportion of the women reported low-back pain, pelvic girdle pain and depression. We also found an association between exercising in mid-pregnancy and having less low-back pain and pelvic girdle pain in late pregnancy. This may appear paradoxical for some women who might assume that exercise would predispose them to low-back or pelvic girdle pain. As in other clinical settings,32 exercise was inversely associated with the rate of depression.
Prevalence of exercise behaviours
Reported exercise levels during pregnancy vary across studies, depending on the definitions used, which trimester the exercise level was measured, and the type of population studied. We found a higher prevalence of women who engaged in exercise less than once a week (31.3%) compared to Haakstad et al33 (24.6%). This discrepancy may be due to differences in the populations studied, as our study had fewer participants with higher education, thereby being more representative for the overall pregnant population. However, our results concerning number of women following exercise guidelines during pregnancy correspond with those of Evenson et al and Petersen et al, where 15.6% and 14% exercised at least five times a week for at least 30 min at moderate intensity, participated in vigorous-intensity activities three times a week for at least 20 min, or did both. However, gestational age of the participants was not reported in these studies, and the response rate reported in Evenson et al23 was 49%.34 On the basis of prior studies demonstrating a decrease in exercise and total amount of physical activity during pregnancy,24 ,33 it is reasonable to believe that our prevalence estimates would have been even lower if we had measured level of exercise later in pregnancy. This was not possible in the present study, as questions about exercise level were posed only in Q1. Because of the very few exclusion criteria, the large study population and a response rate above 80%, our exercise estimates likely represent pregnant Norwegian women living in the areas surrounding Akershus University Hospital and most probably pregnant Norwegian women as a whole.
We can speculate as to reasons for the low exercise level; our study provides an important rationale for investigation of this phenomenon of physical inactivity during pregnancy. We speculate that it may be due to residual dogma that exercise may lead to fetal hypoxia, fetal growth restriction and hyperthermia with potential teratogenic effects.3 In addition, barriers toward exercise during pregnancy are pregnancy-related complaints, lack of time, too much effort to get started and childcare difficulties.20 ,26 Our results extend previous studies reporting that women who exercise regularly are more likely to be primiparous, more highly educated and less likely to be overweight.20 ,21 ,23–25 ,34 As exercise has health benefits for both the mother and the fetus,11 there is a clear need to communicate to women that current exercise guidelines are safe, and that women can achieve these benefits through a range of different and motivating activities.
Self-reported low-back pain and pelvic girdle pain
Our findings concerning the associations between exercise and low-back pain and pelvic girdle pain suggest that exercise in mid-pregnancy decreases the prevalence of such complaints in late pregnancy. In addition, we found a trend towards a dose–response relationship between exercise and pelvic girdle pain, where the OR for having pelvic girdle pain became lower with exercising ≥3 times a week. Previous studies have demonstrated that women with pelvic girdle pain report higher degrees of disability compared to women with low-back pain.19 ,35 These and our results suggest that the disorders should be differentiated.14 Earlier observational studies have concluded that leisure-time physical activity before pregnancy decrease the risk for developing pelvic girdle pain and/or low-back pain during pregnancy.36–38 These results may be explained by the hypothesis that pregnant women in good physical condition are more likely to handle the changes in the musculoskeletal system better (eg, increased ligament laxity and joint impact) compared to their sedentary counterparts.
Does exercise in pregnancy prevent depression occurring?
The present results showed an association between exercising 1–2 times a week and fewer symptoms of depression. However, the results did not reach statistical significance among participants exercising ≥3 times a week. The lack of this dose–response relationship may be explained by wide CI and that only 26% undertook exercise ≥3 times a week, while 42.7% exercised 1–2 times a week. A possible association between exercise and reduced depressive symptoms has previously been explained as exercise causing distraction from discomfort, pain and light depression, leading to improved self-efficacy and increased levels of endorphins, norepinephrine and serotonin.39 We have no available data to investigate this hypothesis. In a recent randomised controlled trial (RCT) a supervised, 3-month aerobic exercise programme reduced depressive symptoms among pregnant women.40 Earlier observational studies have shown conflicting results. Some studies have found an association between exercise and/or total physical activity level (occupational, recreational and transportation activities) and less depressive symptoms in pregnancy.9 ,41–45 Other studies have not found such associations.8 ,46 ,47 The lack of documented associations in these studies may be because of small sample sizes (n=≤65).8 ,46 and a homogeneous study sample, considered to be more active than the general population.47 To our knowledge, the present study is the first to show an association between exercise and depression during pregnancy among pregnant women in Western Europe, using a valid and reliable instrument to measure depression in a pregnant population.
There are some limitations to address. First, women who were not able to complete a questionnaire in Norwegian were excluded, making it impossible to generalise the results to non-Scandinavian ethnic groups. Additionally, we have no information concerning sociodemographic variables of the non-respondents. However, with a response rate at 80.5% we consider the risk for selection bias to be minimal. Second, there was no clinical assessment to diagnose low-back pain, pelvic girdle pain and depression. In addition, there may be other unknown and unavailable confounding variables (eg, heavy workload for lumbupelvic pain) that are not included in the statistical analysis. Another limitation is the self-reporting of exercise, which may be prone to measurement biases, as recall bias and overestimation of physical activity level.48 There are few validated questionnaires that are designed especially to measure physical activity in a pregnant population.49 ,50 However, the questions are similar to the questions used to measure frequency, duration and intensity of exercise in the Physical Activity Pregnancy Questionnaire.50 Haakstad's et al questionnaire was found to correctly categorise exercise levels according to the current guidelines for exercise during pregnancy.
The present study of a population-based sample of women provides novel data that exercise in pregnancy may be associated with reduced prevalence of low-back pain, pelvic girdle pain and depression later in pregnancy. To further examine whether exercise has a causal relationship with such health outcomes will require RCTs.
What this study adds
-
Only 14.6% of the Norwegian population sample followed current exercise guidelines for exercise in mid-pregnancy.
-
The prevalence of self-reported symptoms at week 32 of pregnancy was as follows: low-back pain, 52.1%; pelvic girdle pain, 51.7% and depression, 8.2%.
-
Exercising 1–2 times a week mid-pregnancy was associated with lower prevalence of low-back pain (adjusted OR (aOR): 0.80) and depression (aOR: 0.66), while exercising ≥3 times a week was associated with lower prevalence of pelvic girdle pain (aOR: 0.76).
How clinicians can act on this study
-
Acknowledging the limitations outlined, these data should add confidence to clinicians in telling patients that exercise in mid-pregnancy may reduce the possibility of low-back pain, pelvic girdle pain and depression in late pregnancy.
Acknowledgments
We thank Tone Breines Simonsen, Wenche Leithe and Ishtiaq Khushi for the data collection.
References
Footnotes
-
Contributors KG: idea of the study, data analysis, manuscript writing. KB: idea of the study, manuscript writing/editing. KMO: manuscript editing. ME-G: idea of the study, project leader and manuscript editing.
-
Funding The Akershus Birth Cohort is supported by grants from the Norwegian Research Council, Project number 191098.
-
Competing interest None.
-
Ethics approval Regional Committee for Ethics in Medical Research in Norway (approval number S-08013a).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com