Article Text

Abstract
Background No data exist on ambulatory blood pressure (ABP) in athletes.
Objectives To identify ABP and examine recommended follow-up of high office blood pressure (OBP) in male professional football players and secondary study indicators of sympathetic activity.
Methods Players with high OBP (cases) from a previous screening of 594 players (n=28) were matched for age and ethnicity with players with optimal OBP (controls). High ABP was defined as a mean of ≥135/85 mm Hg during daytime and ≥120/75 mm Hg during night-time. The players replied to questions regarding follow-up of high OBP. High night-time ABP and lack of nocturnal dip (≤10% decline in average BP) were taken as indicators of increased sympathetic activity.
Results 26 cases and 26 controls, mean age 28±4 years, were included. 15 (58%) of the cases had sustained hypertension and 11 (42%) white coat hypertension. Among the controls, 17 (65%) had normotension and 9 (35%) masked hypertension. ABP during night-time was high in 23 (88%) of the cases and in 16 (64%) of the controls, and nocturnal dip was absent in 9 (35%) and 11 (42%), respectively. 10 (38%) of the cases had no follow-up of high OBP.
Conclusions More than one-third of the players with optimal OBP had masked hypertension during daytime and more than half of all players had high ABP during night-time, which are novel findings in athletes. Together with the reduced nocturnal dip, this might indicate increased sympathetic activity. Follow-up of high OBP after preparticipation screening is random and should be organised.
- Cardiovascular epidemiology
- Athletics
- Soccer
Statistics from Altmetric.com
Introduction
Blood pressure (BP) status in athletes is mainly derived from preparticipation office BP (OBP) screening on one occasion without organised follow-up.1 The common opinion is that OBP is higher than ambulatory blood pressure (ABP).2 ABP, which can reveal masked hypertension, is recommended as an adjunct to OBP measurements by international guidelines,3 and is superior to OBP in predicting cardiovascular (CV) events.4 There are, however, no studies of masked hypertension in athletes, despite the fact that young age, male gender, physical activity and mental stress characterise both athletes and people with masked hypertension.5–7
During preparticipation cardiac screening of male professional football players in Norway, 7% had high OBP (≥140/90 mm Hg), and there was a significant linear relationship between increasing OBP and indexed LV massBSA.8 Increased BP was also significantly associated with increased heart rate (HR) and pulse pressure (PP),8 both of which might be reckoned as indicators of sympathetic activity.9 ,10 Players with high BP were recommended additional BP recordings after the screening, but there was no organised control.
The main aims of this investigation were to identify the prevalence of high ABP in male professional football players in Norway and to examine the players’ compliance to recommended follow-up of high BP. Second, we wanted to study if indicators of sympathetic activity were increased in players with high BP.
Methods
From February to April 2008, male professional football players from the Norwegian elite and first division leagues underwent mandatory preparticipation cardiac screening11 when attending a preseason training camp in La Manga, Spain.8 They responded to a questionnaire regarding their height and weight, from which body mass index (BMI) was calculated. They were also asked if their ethnicity was Caucasian (white), Afro-American (black) or other. When in doubt, birthplace or parents’ homeland was used. If the parents came from different continents, the players were categorised as ‘mixed’ ethnicity.
Based on the players’ BP from the screening in 2008, we designed a case–control study and recorded ABP from October 2010 until February 2011. All available players with untreated high BP (n=37) were assessed for eligibility as cases, excluding players living abroad. Controls were randomly selected from players with optimal BP (n=250), according to a predefined protocol, and individually matched for age group (or maximum age difference 4 years), ethnicity and professional football team. All participants gave informed written consent. The study was approved by the Regional Ethical Committee.
Office blood pressure
BP was measured at least 1 h after exercise and after 5 min rest in a sitting position, using a validated automatic BP monitor (Dinamap ProCare DPC300N, GE, Milwaukee, Wisconsin, USA). Systolic BP (SBP) and diastolic BP (DBP) were registered as the mean of two consecutive BP recordings.
Ambulatory blood pressure
On the recording day, the players resigned from snuffing and exercise in the morning, and they did not participate in football or other sport activities for the following 24 h. Outside this, they engaged in normal activity in accordance with the guidelines from the European Society of Cardiology and the European Society of Hypertension.3 The project leader (HMB) fastened the cuff, adjusted it to the upper-arm girth of the players’ non-dominant arm and the ABP device (Tonoport, Cardiosoft, GE Healthcare, Oslo, Norway) was kept in a belt. The ABP device was programmed with software CardioSoft V.6.61 to obtain BP readings at 30 min intervals from 7:00 until 21:59 h and at 60 min intervals during the night. Night-time was later adjusted to reported time in bed, and daytime the rest of the time. During daytime, they were informed to relax their arm when the recordings started. Measurements were automatically repeated when registered as not valid. The players also reported if they used any medications, if something extraordinary occurred during the recording period, and if they had undergone additional OBP or ABP recordings after the screening in 2008.
Data definitions
Among the 52 players, daytime ABP monitoring was successfully committed in all players, at night-time in 51 players. The mean valid measurements were 26.9±4.5 and 8.3±3.4 during the day and night, respectively. According to the published guidelines, high OBP was defined as ≥140/90 mm Hg, high ABP during daytime ≥135/85 mm Hg, during 24 h ≥130/80 mm Hg and during night-time ≥120/75 mm Hg.3 ,12 We used daytime ABP, which is most common, when the players were categorised in four BP subgroups:13 True normotension (OBP <140/90 mm Hg and daytime ABP <135/85 mm Hg), white-coat hypertension (OBP ≥140/90 mm Hg and daytime ABP <135/85 mm Hg), masked hypertension (OBP <140/90 mm Hg and daytime ABP ≥135/85 mm Hg) and sustained hypertension (OBP ≥140/90 mm Hg and daytime ABP ≥135/85 mm Hg). After ABP monitoring, both players with true normotension and white-coat hypertension were defined as normotensive players, and both players with masked hypertension and sustained hypertension were defined as hypertensive players.
PP was calculated as the difference between systolic BP (SBP) and diastolic BP (DBP). Mean arterial pressure (MAP) was defined as DBP+1/3 (SBP–DBP). Nocturnal dip in BP was defined as a mean 10% decline in average SBP or DBP at night compared with daytime.14 High HR,10 increased PP and9 night-time ABP, and lack of nocturnal dip14 were considered as indicators of increased sympathetic activity.
Data analysis
The outcome variables for this study were mean SBP, DBP, MAP, HR, PP and nocturnal dip in SBP and DBP. Correlation between office and daytime ambulatory MAP was tested using Pearson's bivariate correlation analysis. Differences between two groups were analysed using t tests for continuous variables, and Fisher's exact tests for categorical variables. Differences in means between all BP subgroups were calculated using analysis of variance test for trend for continuous variables, and linear-by-linear analysis for categorical variables (Otable 1). Differences in means between the subgroups were calculated using the Bonferroni procedure to control the risk of a type I error (table 1). Included cases and controls were compared with the remaining players with high and optimal OBP, respectively, to test for selection bias.
Comparisons of all 52 players divided into four blood pressure subgroups defined by office and ambulatory blood pressure
Data are presented as mean±SD or as numbers (percentages). A p<0.05 was considered statistically significant, and all tests were two-tailed. The statistical analyses were conducted using SPSS (V.18.0; SPSS Inc).
Results
Individuals
Of the 594 male professional football players, 250 (42%) had optimal, 197 (33%) normal, 108 (18%) high normal, 37 (6%) hypertension grade I and two had hypertension grade II.8 Twenty-six of the 28 (93%) non-treated hypertensive players (cases) still living in Norway, and 26 controls were included in this study (figure 1). OTable 2 shows the baseline characteristics of the study group. Compared with controls, cases had a significantly higher BMI, MAP and PP (table 2).
Baseline characteristics of the study group in 2008
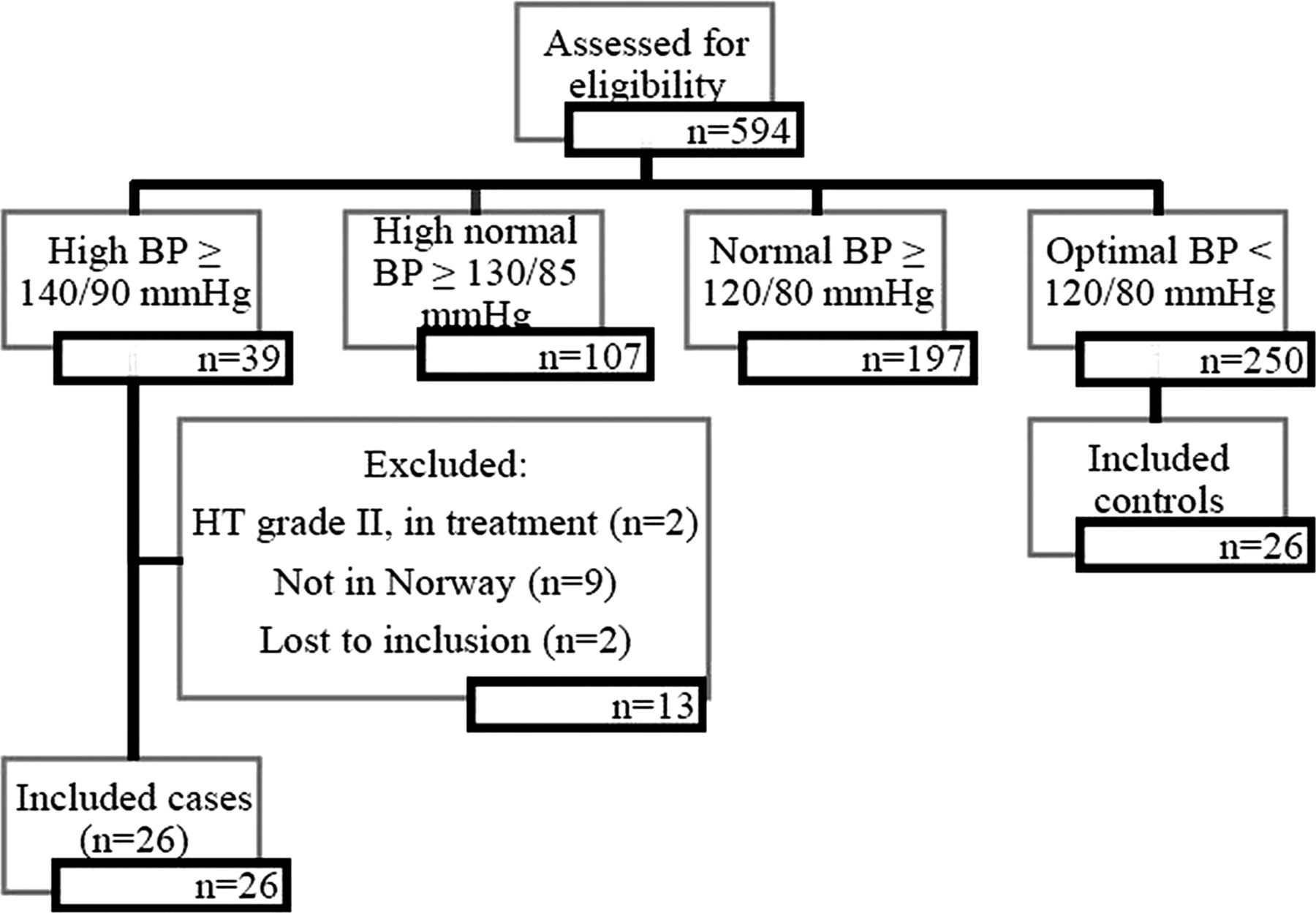
Study flow chart. HT, hypertension.
There were no differences between our controls (n=26) and the remaining and not included football players with optimal BP (n=224) regarding baseline characteristics, except the following: Our controls had higher DBP (68.3±6.2 vs 65.5±6.4 mm Hg; p<0.05) and MAP (83.5±4.7 vs 81.2±5.2 mm Hg; p<0.05) than the not included controls (n=224). There were also less black players (1 vs 4; p<0.05) among the cases than among the not included cases (n=11).
Ambulatory blood pressure
Table 3 shows the ABP results separately for cases and controls. Overall, the players’ mean age was 28.3 years (range 20–35). Significant correlation was found between office and ambulatory daytime MAP (R2=0.21; p<0.01). Compared with controls, cases had significantly higher daytime SBP, DBP and MAP, which was also the case for 24 h and night-time ABP (table 3). Mean night-time ABP was high in 23 (88%) of the cases, and in 16 (64%) of the controls. The cases had less nocturnal BP fall for both SBP and DBP, but the differences were not significant. Nine (35%) cases and 11 (42%) controls had less than 10% nocturnal dip in BP.
Ambulatory blood pressure of the study group in 2010
Table 1 shows the prevalence of all players divided into four BP subgroups: Among the 26 controls, 17 (65%) had true normotension, while 9 (35%) had masked hypertension. Among the 26 cases, 15 (58%) had sustained hypertension, while 11 (42%) had white coat hypertension. Figure 2 illustrates a significant linear relationship between BP subgroups for daytime ambulatory SBP and DBP. Table 1 shows the same characteristics for 24 h and night-time ABP, including MAP and PP. The relationship was not significant for HR.

{kind=link}
{kind=link}
Office blood pressure (OBP) and daytime ambulatory blood pressure (ABP) of the study group. The diagram illustrates the significant linear relationship for BP subgroups (normotension (NT), white coat hypertension (WCH), masked hypertension (MH) and sustained hypertension (SHT)) versus mean (±SD) daytime ambulatory systolic and diastolic BP, and the differences between BP subgroups. *p<0.001 versus NT, †p<0.05 versus WCH, ‡p<0.001 versus WCH.
In all, 24 (46%) players had high daytime ABP (table 1). If high ABP instead was defined according to cut-off values for 24 h or night-time ABP, 34 (65%) or 39 (75%), respectively, had high ABP. Nine (38%) of the players had isolated ambulatory systolic daytime hypertension. The players did not report the use of any medication or extraordinary events during the 24-h ABP recordings that should affect the results.
Follow-up of BP recordings
After the screening in 2008, 16 (62%) cases and 16 (62%) controls had new OBP recordings as part of the football teams’ annual screening. One case was at the family physician and had an ABP recording. Two players with hypertension grade II had received antihypertensive treatment and were not included in this study.
Discussion
The main and novel findings of the present study were a high prevalence of masked hypertension (35%), high ABP during night-time and a random follow-up of high OBP after preparticipation screening of male professional football players. We consider high ABP, both day and night, to be of particular interest, since all participants were young athletes.
Masked hypertension in young athletes
If we extrapolate the results from this case-control study to the entire cohort of 555 professional football players without high OBP in the preparticipation screening study, the number of players with masked hypertension would have been 192 (35%), or 32% of all players (n=594),which seems to be higher than expected. There are, however, no studies of ABP in young athletes and limited knowledge of ABP in healthy young men. The most comparable results derive from Schettini et al’s6 general population study, showing similar office and ambulatory SBP in 20-year-old to 39-year-old men, and from Selenta et al15 reporting masked hypertension prevalence of 23% among 319 normotensive participants (50% men) with a mean age of 27 years (range 17–68 years). In Verberk et al’s16 meta-analysis based on 24 studies of both genders from 20 to 72 years, the prevalence of masked hypertension was 19±4%, varying from 1% to 61%. In Bobrie et al's17 systematic review, the prevalence varied from 8% to 48%. Both studies included papers with major distinctions in measurement methods, cut-off values, age, sex and participating patients; normotensives, untreated or treated hypertensive patients.
Considering that Schettini et al and Selenta et al are showing approximately the correct prevalence of masked hypertension in young men, it is essential to identify whether our results reflect a true higher prevalence of masked hypertension in young male athletes. In this context, it is important to emphasise that the prevalence of masked hypertension in a study population will be relatively higher when only patients with normotension are included, or when the prevalence of hypertension is low, as in our study. The opposite holds good when all BP categories are included or when the prevalence of hypertension is high. Moreover, the inclusion rate of 93% of possible cases in the present study and no clinically important selection bias among the controls may support that our results are representative of young male professional football players.
On the other hand, our results might reflect an overestimation of masked hypertension due to ‘spurious systolic hypertension’, which might be an innocent clinical condition of isolated systolic hypertension in physically active people.18 Athletes may have increased PP and SBP, while DBP is normal according to a higher resting stroke volume and cardiac output, resulting in the central systolic pressure being normal and much lower than the brachial systolic pressure.18 However, only 38% of the hypertensive players in our study had isolated ambulatory systolic hypertension. Our small number of participants and thus less statistical power have also to be taken into consideration. Hence, two players with more or less high ABP would have changed the prevalence of masked hypertension to 42% and 27% (40% and 25% of all players), respectively. The lower estimated value (27%) will still be of considerable size and clinical importance.
Masked hypertension and increased sympathetic activity
There was a significant positive linear relationship between the increasing PP and ABP subgroups, indicating increased sympathetic activity, which has been considered as one of the underlying physiological mechanisms of masked hypertension, similar to sustained hypertension.19 Players with high OBP had less nocturnal BP fall than players with optimal BP, which may indicate increased sympathetic activity in these players. This might be due to mental stress because of a high number of matches during the season and hence the lack of sufficient recovery. The significant association, however, between BP and resting HR reported in our previous study8 was not repeated for ambulatory HR, which is in accordance with other studies of variance of HR, related to OBP and ABP.20 Fagard et al20 suggest that the ‘white-coat’ effect with stimulation of the sympathetic nervous system when BP is measured by an investigator can explain the stronger relationships between HR and OBP than between HR and ABP.
Clinical implications
Although the diagnoses of masked hypertension without repeated OBP recordings do not strictly follow the ESH's guidelines,3 players with high ABP should be regarded as hypertensive because of the superiority of ABP compared with OBP in predicting CV events.4 Verdecchia et al21 have suggested that prognosis is worse when the BP load is persistent throughout the 24 h than when limited to the daytime hours and that hypertension in young adults increases the CV risk, because of the persistent BP load over many years. Although the risk for CV morbidity and mortality is comparable for subjects with masked and sustained hypertension in meta-analysis,13 this is not validated in a young study population. Isolated systolic hypertension could also decrease the CV risk according to a small recent study of young subjects with isolated systolic hypertension and low central BP.22 Besides, young healthy athletes, slim and physically active, commonly score better than the general population of similar age regarding CV risk factors.21
Only 65% of the players with high OBP in the preparticipation screening study had additional BP recordings, which reflect poor compliance with the guidelines in this area.3 The reason for this inconsistency might be that the positive findings of high BT in otherwise healthy young athletes were not sufficiently emphasised. The challenge, however, is to select for follow-up only the players with increased risk, especially when the OBP is normal.
Limitations
OBP and ABP were not recorded simultaneously and not repeated. Different BP devices were used for OBP and ABP without any agreement analyses; however, there was significant correlation between office and ambulatory daytime MAP.
The ABP recordings were conducted over a limited time period, yet with a different number of workouts for each player. However, owing to the individual matching of case and control within football teams, weekly exercise was still comparable within pairs.
We used no questionnaires regarding personality, earlier diagnoses of high OBP or level of anxiety or stress. Persons with higher levels of type A personality usually have higher OBP23 and earlier hypertension labelling has been proven in other studies to increase OBP.5 ,24 Increased physical activity and psychosocial factors such as anxiety and job stress may selectively raise the ABP relative to OBP.13
The prevalence of high OBP could have been underestimated in the preparticipation screening study due to postexercise hypotension,25 since some of the players, owing to strict timetables, had been exercising up to 1 h before the BP recordings.8 This was, however, not representative of the majority of the players. We therefore consider that this cannot explain the present high prevalence of players with masked hypertension.
Perspective
In conclusion, this is the first study of ABP in young athletes to reveal a high prevalence of masked hypertension in male professional football players. One reason for this might be enhanced sympathetic activity, which is indicated by high ABP during night-time, lack of nocturnal dip in BP and a significant linear relationship between increasing BP subgroups and PP. Repeated measures of high BP appear random, and we recommend a closer focus on follow-up of BP screening results in athletes.
What are the new findings?
-
This is the first study of ambulatory blood pressure in young athletes.
-
There is a high prevalence of masked hypertension (normal office blood pressure and high ambulatory blood pressure) in professional male football players. This is an independent risk factor for cardiovascular disease.
-
Ambulatory blood pressure during night-time is also high in more than half of the players.
-
The players’ follow-up of high office blood pressure from preparticipation screening is often random.
How might it impact on clinical practice in the near future?
-
We will get a closer focus on blood pressure measurements during preparticipation screening.
-
Ambulatory blood pressure monitoring will be performed when appropriate.
-
Follow-up of high blood pressure will be organised.
Acknowledgments
The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the South-Eastern Norway Regional Health Authority, the International Olympic Committee, the Norwegian Olympic Committee & Confederation of Sport, and Norsk Tipping AS. The authors would like to thank all the players who participated in the study and Professor Ingar M K Holme for statistical support.
References
Footnotes
-
Contributors HMB designed the study, collected all the data, wrote the statistical analysis plan, cleaned and analysed the data, and drafted and revised the paper. She is the guarantor. EES designed the preparticipation study and monitored data collection for the trial, contributed to the design of this study and revised the paper. TEA designed the preparticipation study and monitored data collection for the trial, contributed to the design of this study, and revised the paper. KS designed the preparticipation study and monitored data collection for the trial, contributed to the design of this study, monitored data collection for this study, analysed the data and drafted and revised the paper.
-
Funding This research was supported by the Oslo Sports Trauma Research Center, Oslo, Norway, and the Akershus University Hospital, Lørenskog, Norway.
Competing interests None.
Ethics approval The Regional Committee for Medical Research Ethics, South-Eastern Norway Regional Health Authority, Norway.
Provenance and peer review Not commissioned; internally peer reviewed.