Article Text

Abstract
With measurement of physical activity becoming more common in clinical practice, it is imperative that healthcare professionals become more knowledgeable about the different methods available to objectively measure physical activity behaviour. Objective measures do not rely on information provided by the patient, but instead measure and record the biomechanical or physiological consequences of performing physical activity, often in real time. As such, objective measures are not subject to the reporting bias or recall problems associated with self-report methods. The purpose of this article was to provide an overview of the different methods used to objectively measure physical activity in clinical practice. The review was delimited to heart rate monitoring, accelerometers and pedometers since their small size, low participant burden and relatively low cost make these objective measures appropriate for use in clinical practice settings. For each measure, strengths and weakness were discussed; and whenever possible, literature-based examples of implementation were provided.
- Exercise
- Evaluation
- Measurement
Statistics from Altmetric.com
Regular participation in physical activity provides an array of important health benefits.1 ,2 Prospective epidemiological studies have demonstrated that the risk of all-cause mortality is lower in physically active and/or fit adults than in their inactive counterparts3 ,4 and that a mid-life increase in physical activity or fitness reduces risk of all-cause mortality.5 ,6 This has prompted numerous medical and public health organisations to issue position statements and official recommendations endorsing the promotion of physical activity for enhancement of public health.7–9
Although the US Preventive Services Task Force has concluded that the current evidence base is insufficient to recommend for or against behavioural counselling to promote physical activity in primary care settings,10 many healthcare organisations and government agencies recommend that primary care providers routinely counsel individuals about physical activity.11–14 In 2007, the American College of Sports Medicine (ACSM) and the American Medical Association (AMA) launched the Exercise is Medicine initiative, to encourage patients to incorporate physical activity and exercise into their daily routine (http://www.exerciseismedicine.org). Importantly, a priority of the Exercise is Medicine programme is to encourage the physicians to routinely record physical activity as a vital sign during patient visits and to prescribe exercise to their patients.15
With measurement of physical activity becoming more common in clinical practice, it is imperative that healthcare professionals become more knowledgeable about the different methods available to measure physical activity behaviour. Although patients are normally able to describe their exercise habits in general terms, obtaining detailed and accurate assessments of physical activity is an extremely difficult undertaking. Unlike other health behaviours, physical activity does not come in handy easy to measure packages or containers (eg, packets of cigarettes/day); and while cardiorespiratory fitness is moderately correlated with physical activity, physical activity lacks a precise biological marker. Physical activity is also an exceedingly complex health behaviour characterised by multiple dimensions and multiple domains. The dimensions of physical activity include frequency, duration, intensity and type, while the domains of physical activity include leisure time physical activity, occupational physical activity, transportation activity and activities associated with work in the house, yard or garden.16 Ideally, a physical activity measurement tool would provide valid and reliable assessments of all four dimensions of activity behaviour in each of the aforementioned domains. However, no such measurement tool currently exists.
Objective measures of physical activity do not rely on information provided by the patient, but instead utilise technology to measure and record the biomechanical and/or physiological consequences of performing physical activity, often in real time. As such, objective measures are not subject to the reporting bias or recall problems associated with self-report methods. The purpose of this article was to provide an overview of the different methods used to objectively measure physical activity in clinical practice. The strengths and weakness of the respective methodologies will be discussed; and whenever possible, literature-based examples of use will be provided. The review will be delimited to heart rate monitoring, accelerometers and pedometers since their small size, low participant burden and relatively low cost make these objective measures appropriate for use in clinical practice settings.
Heart rate monitoring
Relatively inexpensive heart rate monitors with multiple-day storage capacity for minute-by-minute heart rate have made continuous heart rate monitoring a feasible method for assessing physical activity. Heart rate monitoring remains an attractive approach to assessing physical activity because of the linear relationship between heart rate and energy expenditure during steady-state exercise. However, there are several problems associated with this method. First, it is widely recognised that factors such as age, body size, proportion of muscle mass utilised, emotional stress and cardiorespiratory fitness influence the heart rate–oxygen consumption (VO2) relationship. Second, because heart rate response tends to lag momentarily behind changes in movement and tends to remain elevated after the cessation of movement, heart rate monitoring may mask the sporadic activity patterns of children. Third, because a large percentage of a patient's day is spent in relatively inactive pursuits (ie, sitting behind a desk), heart rate monitoring may be of limited use in assessing total daily physical activity.17 However, it is important to note that several techniques have been devised to overcome some of these limitations. These include the use of heart rate indices that control for individual differences in resting heart rate and the calibration of heart rate and work rate on an individual basis (HR FLEX method).17 ,18
Accelerometers
Accelerometry-based motion sensors have become one of the most commonly used methods for assessing physical activity in free-living participants. Worn on the hip or wrist, accelerometers typically sample the acceleration of the body in the vertical, anteroposterior and media-lateral planes at a rate of 10–30 times/s. The acceleration signal is typically filtered, rectified and integrated to provide a generic measure of activity intensity called ‘counts’. Importantly, the algorithmic conversion of the raw acceleration signal to counts varies by make and model, and therefore is not directly comparable. Regardless of how counts are computed, it has been shown that activity counts are strongly correlated with energy expenditure or work rate, and can provide an indication of physical activity intensity. Thus, when recorded in real time, this information can be used to examine the quantity, quality and packaging of free-living physical activity behaviour.
Relative to heart rate monitors, accelerometers present fewer burdens to participants (no electrodes or chest straps) and are capable of detecting the incidental physical activity and the intermittent activity patterns characteristic of children. However, a well-recognised limitation of accelerometers is that they are not able to account for the increased energy cost associated with walking up stairs or an incline and do not accurately measure activities such as cycling, lifting or carrying objects. Nevertheless, it is assumed that the contribution of these activities to the overall physical activity is small. Owing to this assumption, accelerometers may underestimate total or physical activity energy expenditure.19
Interpreting accelerometer data: the issue of cut-points
As physical activity guidelines are typically expressed in terms of frequency, intensity and duration of physical activity, the conversion or calibration of activity counts to units of energy expenditure has received a considerable amount of research attention. The most common approach thus far has been to develop a regression equation that defines the linear or non-linear relationship between counts and energy expenditure. Once a single regression equation has been developed, the activity counts obtained by an individual performing an unknown activity can be used to estimate energy expenditure. Activity count thresholds or ‘cut-points’ denoting the dividing line between light-and-moderate physical activity and moderate-and-vigorous physical activity are typically identified. These cut-points are then used to estimate the amount of time spent in light, moderate and vigorous intensity physical activity.19
Although the application of cut-points continues to be the standard practice, there is a growing recognition that the relationship between accelerometer counts and energy expenditure is dependent on the activity being performed and varies considerably across studies. This has led to the proliferation of multiple and often conflicting sets of intensity-related cut-points which we refer to as the cut-point conundrum.19 Lyden et al20 evaluated the predictive validity of nine published and two proprietary energy expenditure prediction equations for three different models of accelerometers. Across a range of laboratory-based and free-living physical activities, prediction equations consistently underestimated energy expenditure by 0.5–1.3 kcal/min. Physical activity intensity (eg, light, moderate and vigorous) was misclassified 20–35% of the time, with vigorous intensity physical activities being most often misclassified. In a similar fashion, Trost et al21 evaluated the accuracy of the cut-point approach in children aged 5–15 years. Across a range of lifestyle activities, the cut-points misclassified the intensity of physical activity between 33% and 68% of the time.
An emerging approach to accelerometer data reduction that promises to significantly improve accelerometer-based measurement of physical activity and sedentary behaviour is pattern recognition or machine learning. In this approach to data reduction, recurring patterns or distinguishing features in the accelerometer data are ‘extracted’ and entered into sophisticated statistical-learning models that predict the physical activity type and/or intensity. For more detailed information about pattern recognition approaches to accelerometer data reduction, the reader is referred to the recent review by Liu et al.22
Application of accelerometers in clinical practice
We now provide two examples that illustrate promising applications for accelerometry in the clinic setting and in clinical populations.
Example 1
Objective physical activity measures are important in clinical care to examine the effectiveness of interventions, especially if the expected outcome is increased physical activity.23 As clinicians frequently design interventions to promote physical activity and functional mobility, it is important that they use objective measures to determine outcome effectiveness.23 We recently explored the feasibility and clinical utility of accelerometry in a busy paediatric clinic by objectively measuring the physical activity and selected cardiovascular disease risk factors in children who are overweight and obese. Paediatricians provided medical interventions and behavioural counselling during clinic visits. They often referred patients to nutritionists and social workers but did not make referrals to physical therapy to measure or provide physical activity interventions. We conducted this study to increase awareness of physical activity measures and to determine feasibility and utility of these measures in the management of childhood obesity in primary care.
A total of 114 patients were referred to this measurement project by their paediatricians and 82 children (72%) participated. The children had a mean age of 10.3±1.9 years, and a mean body mass index (BMI) centile of 97.9±2.0. The children completed assessments of cardiorespiratory fitness (Balke submaximal treadmill test) and blood pressure in the clinic. On completion of the fitness assessments, the children wore an ActiGraph GT1M accelerometer for seven consecutive days. Parents provided proxy reports of their children's physical activity level.
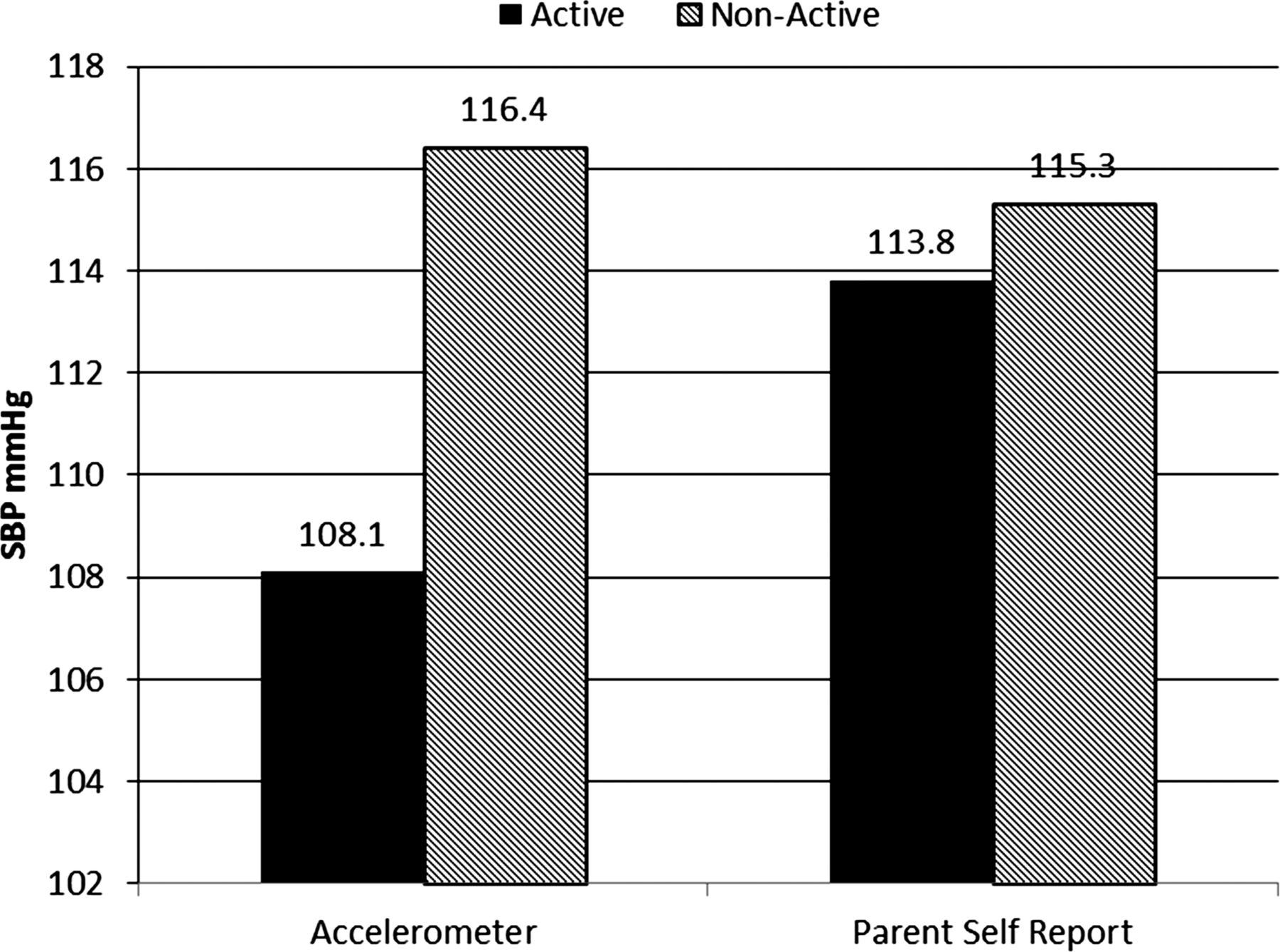
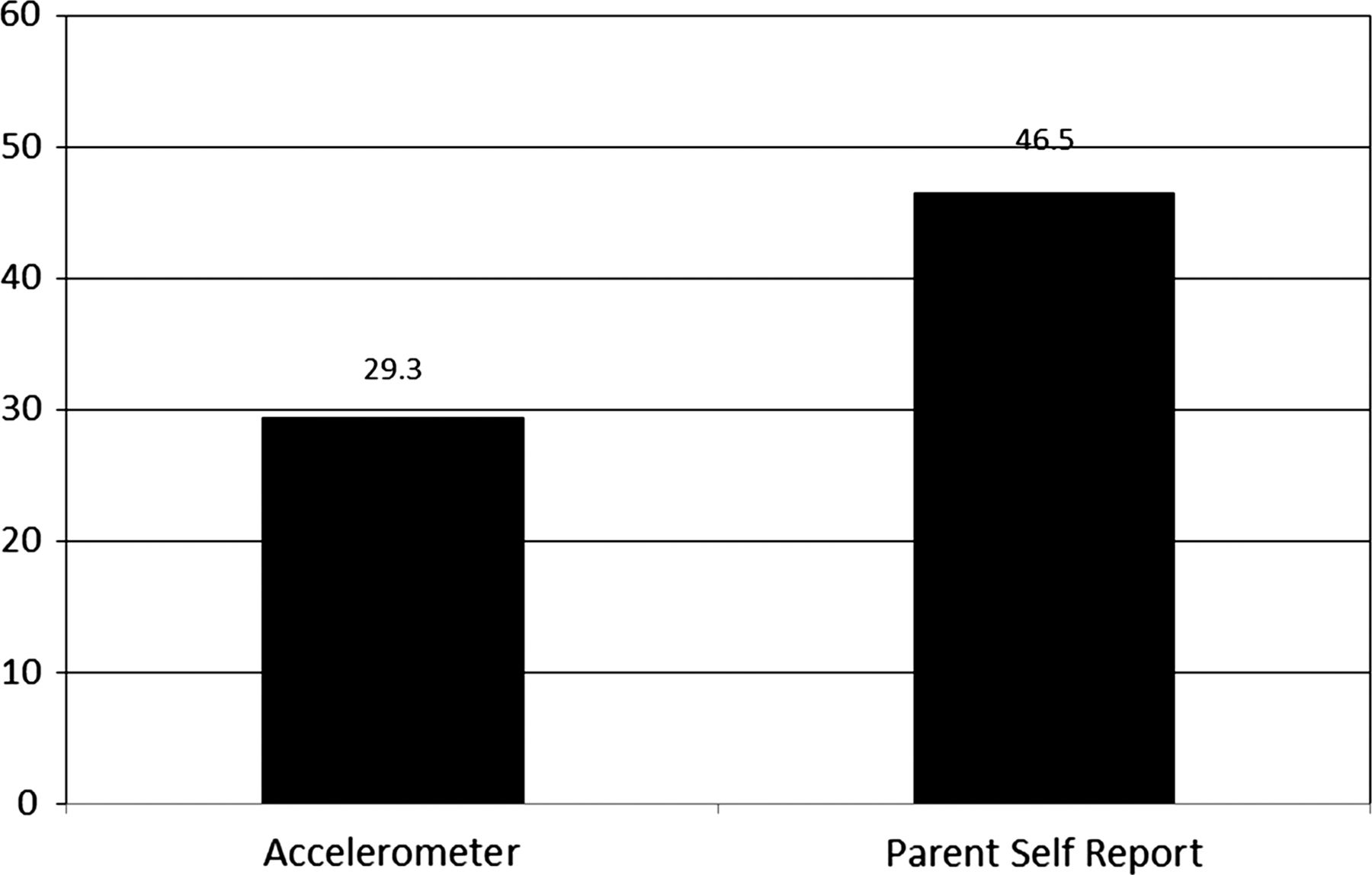
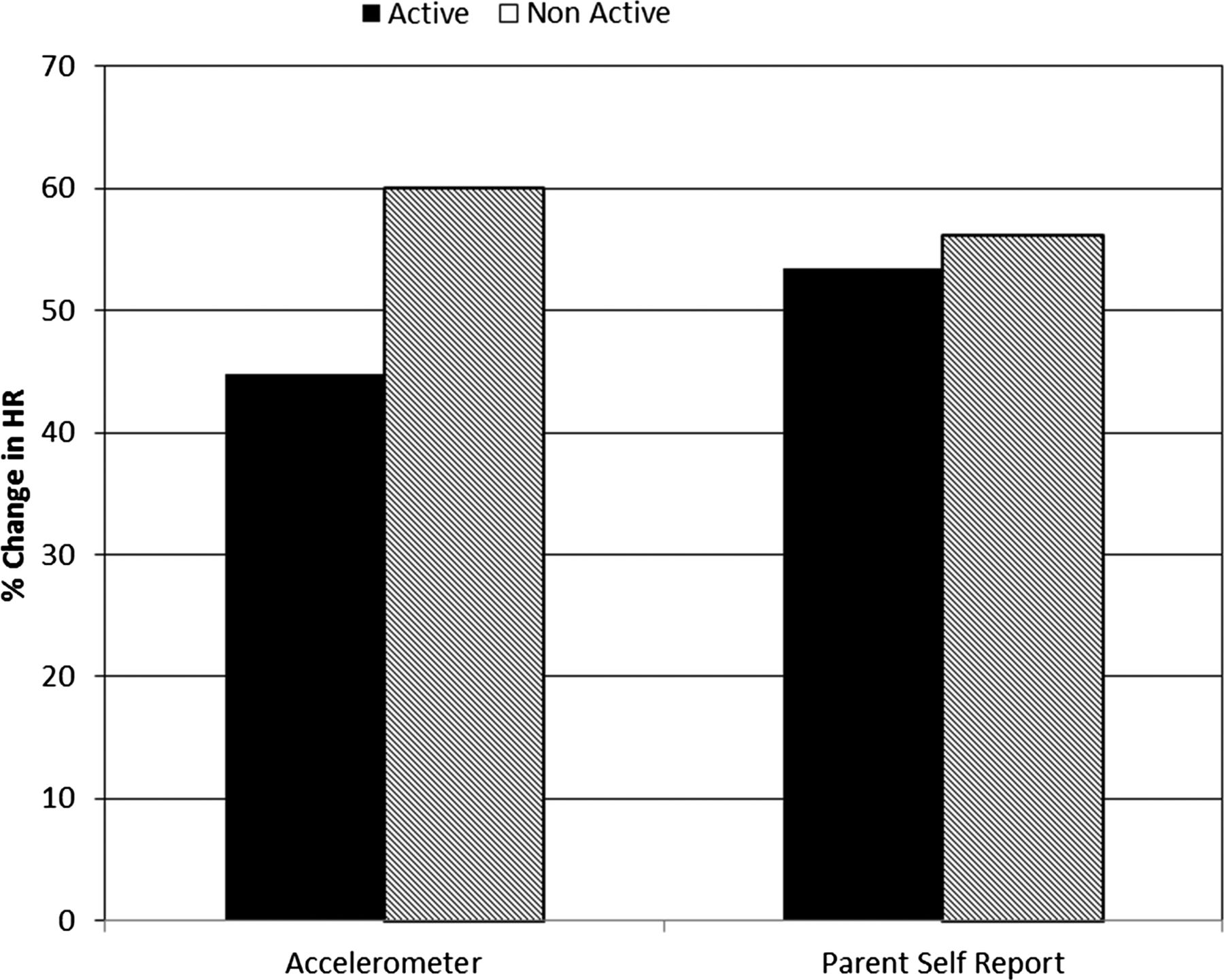
Based on the accelerometer data, only 29% of the children accumulated the recommended 60 min of moderate-to-vigorous physical activity on a daily basis. In contrast, self-report data from parents indicated that nearly half (46.5%) of the children met the 60 min recommendation (figure 1). Of note, children classified as meeting activity guidelines based on the accelerometer data exhibited a significantly higher levels of cardiorespiratory fitness than low-active children, as evidenced by the lower percentage increase in heart rate during the Balke submaximal treadmill test. No differences in cardiorespiratory fitness were observed when activity status was based on parent self-report (figure 2). In a similar fashion, the children meeting the guidelines on the basis of the accelerometer data exhibited significantly lower systolic blood pressures than low-active children. Importantly, no significant blood pressure differences were observed when physical activity status was based on self-reports from parents (figure 3).
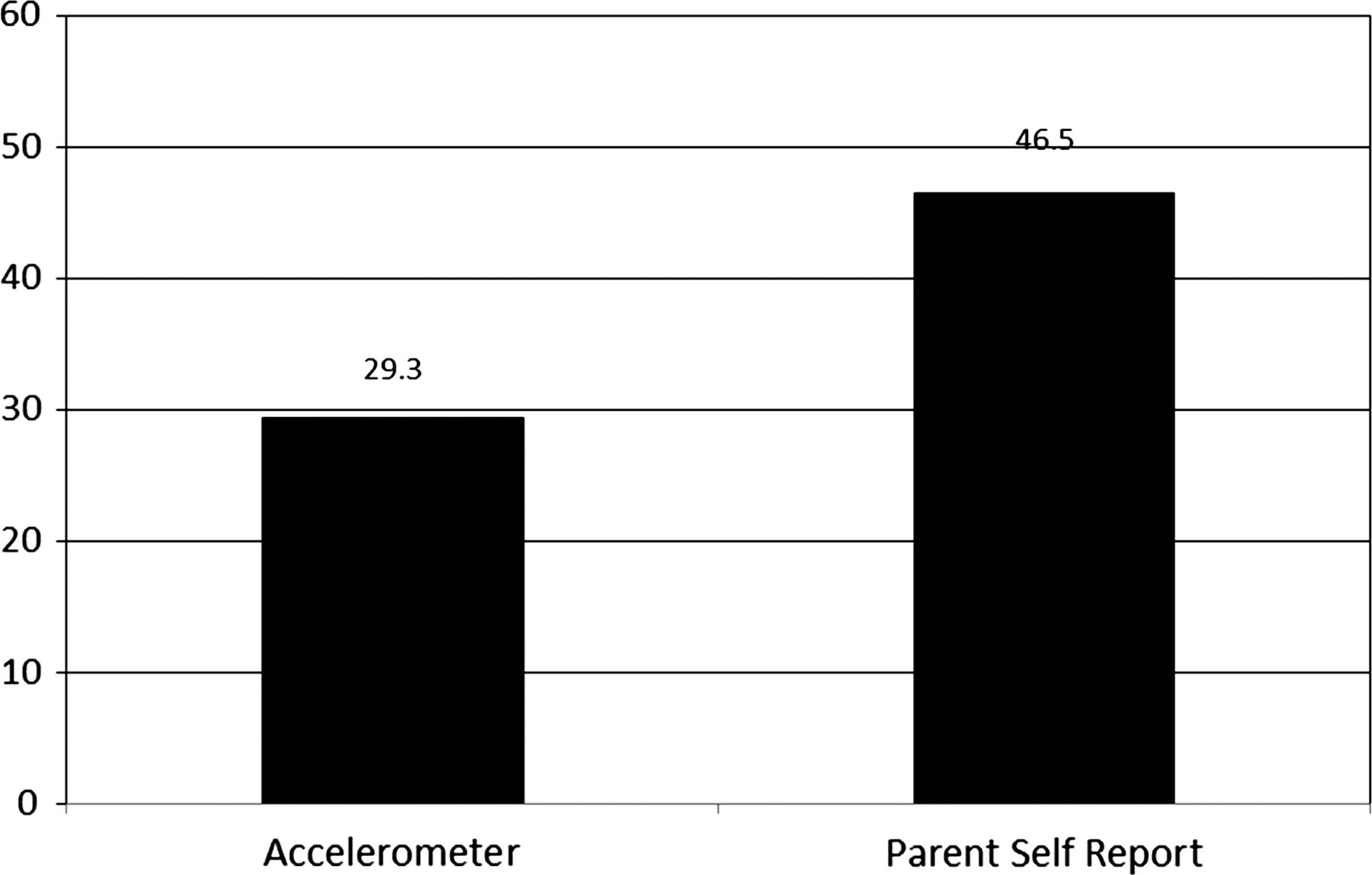
Percentage of participants meeting daily 60 min moderate-to-vigorous physical activity recommendation as measured by accelerometry and parent self-report.

Cardiorespiratory fitness differences in children meeting and not meeting the daily 60 min moderate-to-vigorous physical activity based on accelerometry and parent self-report.
{kind=link}
{kind=link}
{kind=link}
Systolic blood pressure differences in children meeting and not meeting the daily 60 min moderate-to-vigorous physical activity based on accelerometry and parent self-report.
Findings from this study suggest that objective measures of physical activity and cardiovascular fitness are feasible in the primary care clinic setting. Furthermore, children who had higher objective measures of physical activity had higher cardiovascular fitness. Therefore, it seems reasonable to use objective measures of physical activity in clinical management of childhood obesity as a baseline measure of health status and to examine the effectiveness of primary care interventions to promote healthy behaviours.
Example 2
Objective physical activity measures are also being used more frequently in physical therapy interventions for children with disabilities such as cerebral palsy (CP).24 ,25 CP is the most prevalent physical disability of childhood and the most prevalent condition for which paediatric physical therapy is provided.26 Children with CP who are ambulatory often receive physical therapy interventions that emphasise activity and fitness exercises.27 ,28 Therefore, objective measures of physical activity that capture several dimensions of physical activity (frequency, intensity and duration) are important to determine the outcome effectiveness.
Several studies using accelerometers have been conducted to determine the reliability and validity of objective physical activity measures in children and youth with CP.24 ,29 As two types of activity monitors are used most frequently for children and youth with CP (StepWatch and ActiGraph), our group conducted a study to examine which is a more reliable measure of physical activity (interinstrument and test–retest reliability) and which is a more valid measure of physical activity intensity relative to energy expenditure measured by indirect calorimetry. The preliminary findings from our physical activity protocol study with 51 youth with CP suggest that the ActiGraph (intraclass correlation coefficient (ICC)=0.985, 95% CI 0.982 to 0.987) and the StepWatch (ICC=0.977, 95% CI 0.97 to 0.98) have excellent interinstrument reliability. With respect to physical activity intensity, the ActiGraph showed marginally stronger concurrent validity (Spearman correlation=0.85, p<0.001) than the StepWatch monitor (Spearman correlation=0.77, p<0.001). These findings support the use of accelerometry as an objective outcome measure for physical activity frequency and intensity for those interventions that focus on increased fitness and physical activity in youth with CP. Too often, clinical measures rely on self-report assessments which are influenced by bias and which may not be responsive to change. Furthermore, the use of accelerometry as a proxy for physical activity intensity may prove very useful clinically as it is not often feasible for children and youth with CP to participate in an aerobic capacity test using indirect calorimetry, these measures are usually used in laboratory setting only. And oftentimes, children and youth with CP are highly sensitive and do not tolerate use of the face mask for measures of VO2.
Pedometers
A cost-effective alternative to accelerometry is to measure physical activity with a pedometer. A pedometer is an electronic or electromechanical device worn on the waist or hip that counts each step a person takes by detecting the acceleration of the body's centre of mass during the gait cycle. When the acceleration exceeds a critical threshold, the device counts a step. Pedometers can also be used to estimate distance travelled or energy expended. However, because the distance of each person’s step varies, an informal calibration, performed by the user, is required. A number of commercially available pedometers also offer automated data recording and downloading features, and provide estimates of physical activity intensity and energy expenditure. However, the validity of these estimates varies considerably across makes and models of pedometers.30 The primary limitation of pedometers is that they function like an on and off switch and do not consider the magnitude of the movement detected. Hence, movement above a given threshold is counted as a step regardless of whether it occurs during walking, running or jumping. Pedometers also do not detect the increased energy cost associated with walking up stairs or an incline and do not accurately measure certain physical activities such as cycling, swimming or lifting and carrying objects.19
Application of pedometers in clinical practice
Pedometers are the most commonly used assessment tools to objectively monitor and promote physical activity in clinical settings. Bravata et al31 conducted a meta-analytic review of studies evaluating the effectiveness of pedometer-based physical activity intervention among outpatient adults. In studies that employed randomised controlled designs, pedometer users significantly increased their physical activity by approximately 2500 steps/day more than the control participants. The increase in physical activity associated with pedometer use was associated with a significant reduction in BMI and systolic blood pressure. An important predictor of increased physical activity was the provision of a step goal, such as 10 000 steps/day. Another meta-analytic review of pedometer-based walking interventions concluded that such programs provided a modest, yet significant, weight loss (−1.3 kg, 95% CI −1.85 to −0.70 kg).32 The magnitude of weight loss was associated with the length of pedometer use, with participants losing an average of 0.05 kg/week.33
Pedometers have also been used to monitor and increase physical activity in paediatric patients. Conwell et al34 evaluated the feasibility and efficacy of a pedometer self-monitoring programme in obese children with impaired glucose tolerance. Twenty obese children (mean age 11.8±2.3 years, BMI 34.5±4.9 kg/m2, BMI–standard deviation scores 3.45±0.41) were recruited via paediatrician referral. Prior to the 10-week physical activity programme, each participant was visited by a research assistant and given instructions on how to wear and operate a pedometer. Mean steps per day increased significantly from 10 363±927 at baseline to 13 013±1131 at week 10. Over the 10-week intervention period, insulin sensitivity and parental support significantly improved.
Self-monitoring with a pedometer is also an effective adjunct to more traditional physical activity promotion strategies such as brief physician counselling and referral to a clinical exercise physiologist. A randomised trial tested the effectiveness of three strategies to promote physical activity in general practice.32 ,35 Sedentary patients between the ages of 50 and 70 years were randomly assigned to one of three hierarchical intervention groups: brief advice from a general practitioner (GP); brief GP advice and counselling from an exercise specialist and the combination of brief GP advice, exercise counselling from an exercise physiologist and self-monitoring with a pedometer. At 12 and 24 weeks of follow-up, physical activity levels increased significantly in all groups by an average of 84 min/week and 128 min/week, respectively. With respect to the percentage of patients meeting public health guidelines (150 min/week) at 24 weeks follow-up, those who received the combination of brief GP advice, exercise counselling from an exercise physiologist and self-monitoring with a pedometer were 2.39 times (95% CI 1.01 to 5.64) more likely to meet the guideline than the patients receiving brief GP advice alone.
Summary
We reviewed the methods used to objectively measure physical activity in clinical practice and illustrated the clinical context. For more detailed discussions on measurement of physical activity behaviour, the reader is referred to the reviews by Welk,36 Tudor-Locke and Lutes37 and Atkin et al.38 It should be noted that when selecting an approach to measuring physical activity there will always be a trade-off between accuracy and practicality. All measures of physical activity have inherent strengths and weaknesses. As such, the decision related to which methodology to use will depend on the patient's circumstances and the resources available to the clinician.
What are the new findings?
-
Pedometers are the most commonly used assessment tools to objectively monitor and promote physical activity in clinical settings.
-
Self-monitoring with a pedometer is also an effective adjunct to more traditional physical activity promotion strategies such as brief physician counselling and referral to a clinical exercise physiologist.
-
Objective measures of physical activity can be used in the clinical management of childhood obesity as a baseline measure of health status and to examine the effectiveness of primary care interventions to promote healthy behaviours.
-
Accelerometry serves as an objective outcome measure of physical activity frequency and intensity for interventions that focus on promoting fitness and physical activity in youth with cerebral palsy.
References
Footnotes
-
Contributors SGT planned the review and prepared the final version of the manuscript and submitted it to the journal. SGT and MO identified relevant studies and information, wrote the manuscript, and commented/edited on each other's sections.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.