Article Text

Abstract
Background To investigate the interpersonal and physical environment mediators of the Transform-Us! mid-intervention effects on physical activity (PA) during recess and lunchtime.
Methods Transform-Us! is a clustered randomised school-based intervention with four groups: sedentary behaviour intervention (SB-I), PA intervention (PA-I), combined PA+SB-I and control group. All children in grade 3 from 20 participating primary schools in Melbourne, Australia were eligible to complete annual evaluation assessments. The outcomes were the proportion of time spent in moderate-to-vigorous PA (MVPA) and light PA (LPA) during recess and lunchtime assessed by accelerometers. Potential mediators included: perceived social support from teachers; perceived availability of line markings; perceived accessibility of sports equipment; and perceived school play environment. Generalised linear models were used and mediation effects were estimated by product-of-coefficients (a·b) approach.
Results 268 children (8.2 years, 57% girls at baseline) provided complete data at both time points. A significant intervention effect on MVPA during recess in the SB-I and PA-I groups compared with the control group (proportional difference in MVPA time; 38% (95% CI 21% to 57%) and 40% (95% CI 20% to 62%), respectively) was found. The perceived school play environment was significantly positively associated with MVPA at recess among girls. An increase in perceived social support from teachers suppressed the PA+SB-I effect on light PA during recess (a·b= −0.03, 95% CI −0.06 to −0.00). No significant mediating effects on PA during recess and lunchtime were observed.
Conclusions A positive perception of the school play environment was associated with higher MVPA during recess among girls. Future studies should conduct mediation analyses to explore underlying mechanisms of PA interventions.
- Children
- Intervention Effectiveness
- Physical Activity Measurement
Statistics from Altmetric.com
Introduction
Childhood obesity is a global phenomenon,1 and physical activity (PA) is an important modifiable determinant to target in prevention interventions.2 Ecological models acknowledge that behaviour, including PA, is influenced by environmental factors.3 Environmental influences on behaviour are particularly important for children due to lower autonomy in their behavioural decisions.4 Furthermore, earlier research has indicated that objective and perceived environmental factors are different constructs, and the perceived environment may be a stronger correlate of PA behaviour in children and adolescents.5 Since children spend nearly half of their waking hours at school, this setting provides a potential opportunity for making environmental changes to influence children's PA.3 Changes in the physical environment at school, for example, facility and equipment provision, have shown favourable effects on children's PA.6 ,7 Considering that most children have recess and lunchtime every school day, changes in their PA during these periods could make a significant contribution to their overall PA levels.8 ,9
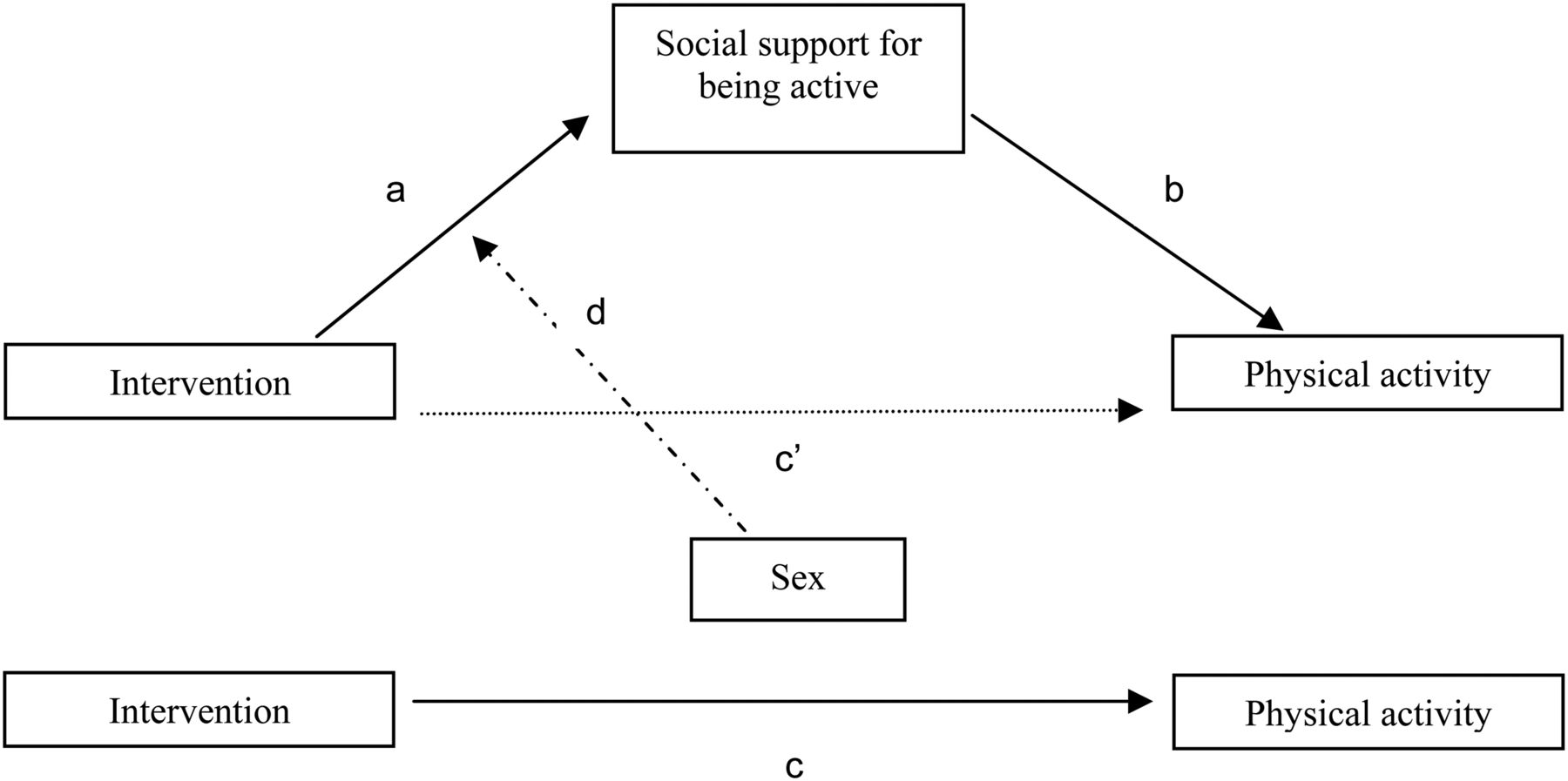
Most school-based obesity prevention and PA promotion studies focus on evaluating whether an intervention worked or not. Few studies have examined how, why and for whom interventions worked.10 These issues can be explored with mediation and moderation analyses. A mediator is an intervening causal variable that lies between a predictor and the outcome.11 An intervention may increase participants’ PA, for example, through increasing social support for being active (figure 1). Moderators are variables that may enhance, reduce or directionally change the predictor–outcome relationship.10 Sex is a frequently studied moderator in childhood obesity prevention interventions, with girls generally shown to benefit more from interventions than boys.12
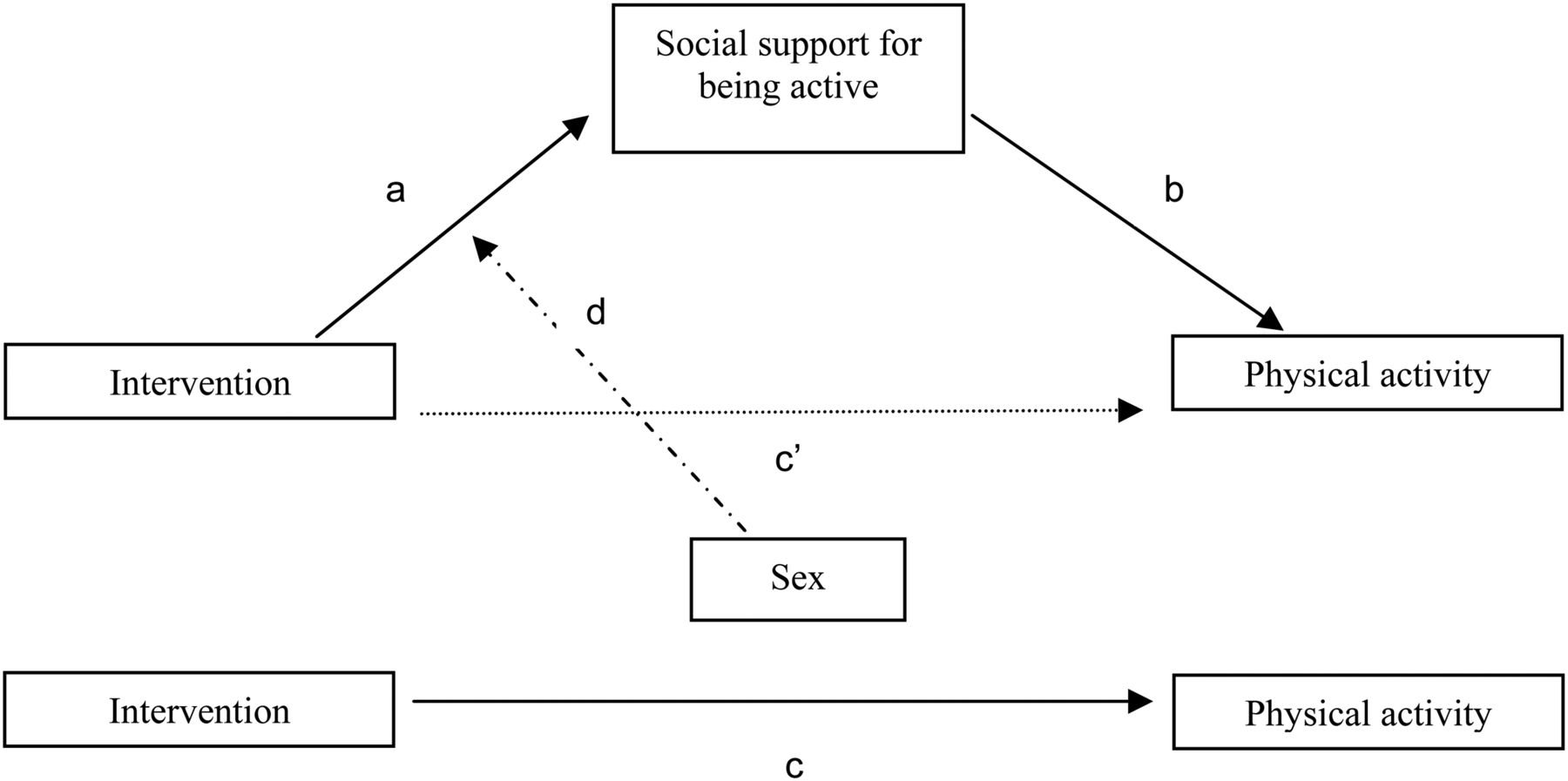
Mediating effect of social support and moderating effect of sex. (a) Intervention effect on the mediator; (b) effect of the mediator on outcome variable while controlling for the intervention effect; (c) overall intervention effect on the outcome variable; c′: direct effect of intervention on the outcome variable while controlling for the mediator variable; (d) moderating effect of sex on the intervention effect on social support.
Transform-Us! (T-Us) is a cluster-randomised controlled trial aiming to increase children's PA and decrease their sedentary behaviour through a behavioural and environmental intervention in the school and family settings in Melbourne, Australia.13 T-Us is based on social cognitive theory,14 behavioural choice theory15 and ecological systems theory.16 This paper investigated whether key intervention components, interpersonal (social support from teachers) and environmental (availability of line markings, accessibility of sports equipment, perceived school environment) factors mediated the mid-intervention effect of the T-Us intervention on objectively measured PA during recess and lunchtime. The potential moderating effect of sex on the intervention effects on the potential mediators was also examined. Exploring mid-intervention mediating mechanisms is useful for determining whether the study is meeting its aims and objectives.
Methods
Sample
Schools with enrolments >300 students, with at least two year 3 classes and within a 50 km radius (31 miles) of Melbourne, Australia were selected from low and mid-high socioeconomic strata (SES) (based on the suburb socioeconomic index for areas score) and randomly ordered.13 Eight of 41 schools in the low SES areas and 12 of 96 schools in the mid-high SES areas agreed to participate. All year 3 children (n=1606) and their parents at participating schools received the programme. As required by ethics, parents signed a consent form for their child to participate in the study evaluation assessments; a total of 599 parents provided consent for their child to complete one or more Transform-Us! evaluation assessments (participation in all components was not compulsory) (figure 2). Varying numbers of children had consent for each evaluation component (n=599 had consent for at least one Transform-Us! assessment component, n=547 children had consent for accelerometer, n=544 had consent for survey and n=512 had consent for both accelerometer and survey evaluations at baseline). The study was approved by the Deakin University Human Research Ethics Committee, the Victorian Department of Education and Early Childhood Development and the Catholic Education Office. Sample and recruitment details are described elsewhere.13

Flow of participants through the intervention.
Intervention
The T-Us is a four-arm cluster-randomised controlled trial (five schools per intervention arm) with a 2×2 factorial design consisting of an 18-month intervention and 12-month booster maintenance periods. Using computer-generated blocks of four, schools were randomly assigned by the project coordinator to one of four groups: physical activity intervention (PA-I); sedentary behaviour intervention (SB-I); combined intervention (PA+SB-I); or usual care control (C). This paper focuses on children's PA only as the mediators of interest are specific to PA. However, it is important to include all intervention groups even those with no focus on PA. Possible subsidiary effects may occur in these groups, such as increasing PA as a result of reducing SB. Intervention components are presented in table 1.13
Intervention components of the Transform-Us! study
Measures
For the current study only baseline and mid-intervention (5–9 months postbaseline) data were used. Baseline data were collected February–July 2010 and mid-intervention data November–December 2010. Children completed questionnaires at school in small groups supervised by trained research staff. Parent questionnaires were self-completed at home.
Physical activity
PA was measured objectively using ActiGraph-GT3X accelerometers.17 Accelerometers were fitted at school by trained researchers. Participants wore accelerometers on a belt over the right hip for eight consecutive days during waking hours at baseline and mid-intervention. Data were collected using the uniaxial function and 15 s epochs. Non-wear time was defined as ≥20 min of consecutive 0 counts. Freedson's age-adjusted cut-points (specific to participants’ age at each time point) were used to categorise children's PA into light-intensity (LPA; >100 cpm—3.9 metabolic equivalent of tasks (METs)), moderate-intensity (4–5.9 METs) and vigorous-intensity PA (≥6 METs).18 ,19 Data from the school recess and lunchtime periods were extracted based on bell times provided by schools. The average recess and lunchtime durations were 31 (±5 min) and 53 (±10 min) minutes, respectively. The outcome variables included the average proportion of time spent in LPA and moderate-to-vigorous PA (MVPA) during recess and lunchtime on weekdays (excluding eating time). Children were required to have data for at least 50% of the recess and lunchtime periods on at least 3 weekdays to be included in analyses.8 As PA data were collected during different seasons at baseline and mid-intervention, maximum temperatures at measurement occasions were used as covariates,20 derived from an online weather service (http://www.tutiempo.net/en/Climate/).
Potential mediators
The potential mediators that were targeted by T-Us for PA change and assessed at mid-intervention were child-reported interpersonal (social support from teacher) and environmental (perceptions of the school environment, availability and accessibility) factors. As change in school-based PA was the focus of this paper, the most relevant social and physical school environment factors were therefore the potential mediators included in the analyses. Online supplementary appendix 1 includes a description of the targeted mediators presented in this paper, the behaviour change technique and intervention components.
Interpersonal
Social support from teachers: five items (yes/no responses) asked the children whether the class teacher comes outside with them, plays games with them, watches them play games, rewards or praises them for playing active games and encourages them to play active games. The total score ranged 0–5 (sum of the ‘yes’ answers), with higher scores indicating more social support from the teacher. One week test–retest reliability for these items ranged between κ=0.2–0.7 and per cent agreement is 70–87%.
Environmental
Perceived school play environment: children were asked to report how much they liked the areas to play in at their school using a five-point Likert-type scale ranging from ‘really dislike’ (score=−2) to ‘really like’ (score=2). One week test–retest reliability for this item was κ=0.2 and per cent agreement=83%.
Perceived availability of line markings: a single item asked children to report (yes/no) whether their school has line markings on the walls or playground to help them play games (eg, 4-square, target on the wall). One week test–retest reliability for this item was κ=0.8 and per cent agreement=97%.
Perceived accessibility of sports equipment: a single item asked children to report (yes/no) whether they are allowed to use school sports equipment during recess and lunchtime. κ Values could not be computed due to lack of variability in responses but percent agreement was 100% for 1 week test–retest reliability.
Demographics and weight status
Children's sex and age were self-reported. Parents (either mother or father) reported their highest level of schooling (as a proxy of socioeconomic status), which was grouped into three categories: <12 years of schooling, 12 years of schooling and university. Weight status of children at baseline was determined from body mass index (BMI) based on measured weight (using portable electronic Wedderburn Tanita scales) and height (using SECA portable stadiometers). Height was measured to the nearest 0.1 cm and weight to the nearest 0.1 kg by trained researchers. Height and weight were each measured twice and the average was calculated. When there was a discrepancy of over 1 cm or 1 kg, a third measurement was taken and the average of the closest two used. Children were categorised as overweight/obese or normal weight based on international definitions.21
Statistical analyses
Only cases that provided complete data for all potential mediator variables and provided valid PA data at both time points were included. All analyses were performed using generalised linear models (GLM) and adjusted for clustering within schools using Stata V.11. Differences at baseline between the study groups were estimated. Drop-out selectiveness was assessed for sex, intervention status, baseline BMI, parental education level, baseline values of PA and mediators.
PA outcome data were positively skewed, therefore GLMs were used with γ variance and logarithmic link function to indicate the proportional difference in PA variables between each intervention group and the control group. For binary outcomes logistic regression models were used, and ORs were reported. Maximum temperature at measurement occasions, sex (when it is not a moderator), baseline BMI and baseline values of outcome and/or mediator (where appropriate) were added as covariates.
Mediation analyses
The effects of the interventions on the outcomes were tested while controlling for baseline outcome measures and relevant covariates. Dummy coded variables were created automatically in Stata to be able to compare each group (ie, PA+SB-I, SB-I and PA-I) to the control group in the same data analysis. The same applied to the intervention effects on the mediators. Mediation analyses were conducted in four steps22:
-
Total intervention effect on PA outcomes were calculated (path c, figure 1),
-
Action Theory Test; intervention effect on potential mediators were tested (path a, figure 1). The moderating effect of sex on these intervention effects was estimated by adding Sex by Intervention group interaction terms. In cases of significant interaction further exploratory subgroup analyses were conducted on both paths a and b, to be able to calculate mediated effects in boys and girls separately.
-
Conceptual Theory Test; the relationship between potential mediators and PA outcomes was estimated (path b, figure 1), while adjusting for the intervention effect on the PA outcome variable (path c, figure 1).
-
The mediated effect was calculated with the product-of-coefficients test (path a · path b).22 The statistical significance of the mediating effect was established by calculating asymmetric CIs using the FORTRAN program called PRODCLIN.23
Sample size calculation for the mediation analysis (based on a simulation study from Fritz et al24) indicated that to detect a moderate mediated effect with 0.05 significance level and 0.80 level of power, with the PRODCLIN method requires a sample size of 74 (without accounting for clustering in schools). Assuming a commonly observed school clustering effect of 5% (intraclass correlation (ICC)=0.05), the sample size required was ‘standard sample size’ × (1+(number of observations per cluster—1)×ICC)=74×(1+(20 schools−1)×0.05)=74×1.95=144.
For all analyses, the statistical significance level was set at p<0.05, except moderation tests where significance was set at p<0.10 due to low statistical power for moderation analyses.25
Results
Participant characteristics
A total of 268 children (of 599) provided complete data for all variables of interest at both baseline and mid-intervention (figure 2). The major reason for excluding children from the final analysis was having inadequate accelerometer wearing time either at baseline or mid-intervention (n=260 of 331 excluded children). However, baseline values of PA and mediators, sex, intervention status, parental education level and baseline BMI were not related to dropping out at mid-intervention. The mean age of children was 8.2 years, 43% were boys, 48% of responding parents had a university education and 22% of the children were overweight/obese at baseline. There were no significant differences between the intervention groups and control group at baseline for sex, age or parental education level except BMI and proportion overweight/obese (as shown in table 2).
Baseline characteristics of the Transform-Us! study participants shown as means (SD) or as percentages
Table 3 shows the proportion of time spent in MVPA and LPA during recess and lunchtime as well as the hypothesised mediators from both baseline and mid-intervention. There were no significant baseline differences between the intervention groups and control group except lunchtime LPA (table 3).
The proportions of recess and lunchtime physical activity and mean (SD) and percentages of potential mediators at baseline (T1) and mid-intervention (T2)
Mediation analyses
Intervention effect on PA during recess and lunchtime (c-path)
At mid-intervention, PA-I and SB-I groups had significantly higher MVPA levels during recess compared to the C group (table 4). Furthermore, children's LPA during recess was significantly higher in the PA-I group compared with the C group. There were no significant differences in lunchtime PA levels between the intervention groups and the C group at mid-intervention (table 4).
Intervention effect on physical activity during recess and lunchtime compared to control group (path c)
Intervention effect on potential mediators (a-path)
As shown in table 5, there was a significant positive mid-intervention effect on perceived social support from teachers in the PA-I and PA+SB-I groups. Sex moderated the intervention effect on perceived school environment in the PA-I and SB-I groups. Among boys the intervention had a negative effect on perceptions of the school environment (the areas to play in at school), whereas among girls the intervention effect was positive. There was no significant intervention effect on the perceived availability of line markings or perceived accessibility of sports equipment (table 5).
Mid-intervention effects on mediators (path a)
Effect of potential mediators on PA during recess and lunchtime (b-path)
Table 6 shows the relationship between the hypothesised mediators and PA during recess and lunchtime, adjusting for intervention group. There were significant inverse relationships between social support from teachers and LPA during recess, and between perceived availability of line markings and LPA during recess and lunchtime. There was a significant positive relationship between the perceived school environment and MVPA during recess (table 6). After stratification, this relationship was evident for girls only.
Effect of potential mediators on recess and lunchtime physical activity—single mediator tests (path b)
Mediated effects
There were no significant mediated effects. There was a significant suppression effect of social support from teachers on the intervention effect on children's LPA during recess in the PA+SB-I group (see online supplementary appendix 2 and figure 3). This means that more social support from the teacher was associated with less LPA during recess. Since none of the mediators were significant in the single-mediator models, we did not conduct multiple mediator analyses.

{kind=link}
{kind=link}
{kind=link}
Suppression effect of social support from teachers on the intervention effect on light physical activity at recess among the PA+SB-I group.
Discussion
To our knowledge, this is the first study that examined the mediating mechanisms of an intervention effect on PA during school recess and lunchtime. Both the PA-I and SB-I showed significant positive effects on MVPA during school recess; the PA-I also had a significant mid-intervention effect on LPA during recess. There were no significant mediating effects.
The school environment (eg, area type and area size) has previously been shown to be an important factor influencing children's PA at recess and lunchtime.6 ,26 ,27 In the current study children's liking of the school play environment was significantly positively related with MVPA during recess among girls. We also found a moderating effect of sex on the effect of the SB-I and PA-I intervention on perceived school environment, with negative intervention effects among boys and positive effects among girls. In general boys are more dominant in the school playground during school breaks,28 but the changes in the school play environment as part of T-Us might have been appreciated by girls due to having more playground space for play. A previous school-based intervention implemented by Ridgers et al29 aimed at increasing PA during recess by redesigning the school playground environment using playground markings and physical structures showed favourable effects on PA levels during recess-lunchtime combined over time. They found that initial changes in the physical environment had a positive impact on children's PA. Another school-based recess intervention highlighted the effectiveness of providing sports equipment to increase children's PA during recess.30
In the current study perceived accessibility of sports equipment was not significantly associated with MVPA during recess and lunchtime, possibly because children in all groups had access to such equipment. Most of the children reported favourably on the accessibility of sports equipment at baseline, which could have produced a ceiling effect, leaving limited room for improvement in the perception of accessibility of sports equipment. Indeed, process evaluation data confirmed that all teachers who were provided with sports equipment for the study reported making this equipment available for the children to use during recess and lunch breaks. An unexpected finding was that perceived social support from teachers appeared to suppress the intervention effect on recess LPA in the PA+SB-I group. Children who perceived more social support from teachers had lower LPA during recess. A possible reason for this could be that teachers were encouraging children to do more structured activities that might not be attractive to children resulting in lower levels of PA. It has been shown that children are more likely to participate in PA in unstructured play settings and a recent study found low adherence to a structured PA break-time programme.31 ,32 Children in the PA+SB group received all the intervention strategies, that is, reducing sitting during class and promoting PA during recess and lunchtime. Teacher support both during classes and school breaks might be perceived as too much control over a child's behaviour since recess may be viewed by children as ‘their time’ and teacher interactions might be perceived as playground discipline.32 ,33 Furthermore, in this age group children are likely to be more sensitive to social support from their peers rather than adults.34
Another unexpected result was that the line markings were significantly inversely related to LPA during recess and both MVPA and LPA at lunchtime. This suggests that at the mid-intervention point, the selected line markings were not effective in increasing children's activity during their recess and lunchtime. Process evaluation found that schools in the SB and C groups reported that they had additional line markings painted in the school grounds during the intervention period even though this was not promoted by the T-Us intervention for these groups.
Strengths of the current study include being the first study to explore the underlying mechanisms with mediation analysis of mid-intervention effects on PA change during recess and lunchtime, and the measurement of PA by accelerometry. We explored the mid-intervention effects on LPA in addition to MVPA during recess and lunchtime. Studying changes in LPA may be important in terms of children's daily energy expenditure and increases in PA may not always be at a moderate or vigorous intensity.
There were also some limitations, such as the self-reported measurement of the mediators, which is subject to socially desirable response bias; and the potential low sensitivity to change of these measures. Some mediating variables had low κ value (despite showing high per cent agreement), which generally happens due to instability in the κ statistic as a result of having a high per cent of responses in one category.35 The perceived school environment was measured by a single item, which prevented us exploring more detailed aspects of its influence on PA change during recess and lunchtime. Low reliability of some of the mediator measures may also be one of the reasons for the lack of significant mediated effects. Although process evaluation data suggest otherwise, the intervention strategies may not have been adequately implemented or may not be the most appropriate for changing the potential mediators. Furthermore, there could be other potential mediators not assessed in this study that may explain children's recess and lunchtime PA. Children who provided complete data were 45% of the total population, mainly due to inadequate accelerometer data at baseline and/or follow-up. This low retention rate is partly explained by the optional nature of the evaluation components, with children not required to complete all evaluation assessment to be enrolled. Non-compliance with accelerometer wear protocols also contributed to inadequate data. However, there was no selective dropout regarding sex, intervention status, baseline BMI, parental education level, baseline values of PA and mediators. It indicated that dropout did not impact the overall representativeness of the sample. The ICCs from the current study ranged 0.07–0.22, which were higher than the a priori estimated ICC (0.05) in the sample size calculation. This may have contributed to a loss of the power of the study and reduced the likelihood of detecting existing associations between the variables of interest.
Contributions and future research
To our knowledge previous PA intervention studies have not explored the mediation mechanisms of their effects on children's PA during recess and lunchtime. There is a current shift in PA research towards ecological models, which emphasise that behaviour is influenced by the physical environment as well as social, cultural, policy and cognitive factors.36 As shown in this study, the perceived school play environment may be one such important influence, being positively associated with children's recess PA behaviour. Apparently recess and lunchtime PA have different mediators and more research is needed to explore what these mediators are to be able to effectively change these behaviours.
Conclusion
The Transform-Us! intervention positively affected children's MVPA and LPA during recess but not lunchtime. There were no significant mediating effects on PA at recess or lunchtime. However, a positive perception of the school play environment was significantly related to girls’ PA during recess. Researchers should explore mediating effects of PA interventions to assist in understanding how such interventions work and to improve ongoing and future interventions.
What are the new findings?
-
Mediation analyses are important for understanding which interpersonal and physical environmental factors explain physical activity behaviour change during school time.
-
Mediation analyses also disentangle suppressing elements of the intervention.
-
Transform-Us! successfully increased children's physical activity during school recess at mid-intervention.
-
The school play environment was positively associated with children's physical activity during recess.
How might it impact on clinical practice in the near future?
-
Future studies should conduct mediation analyses to explore the underlying mechanisms of school physical activity interventions.
-
School-based physical activity promotion studies should also take into account the influence of the school play environment on children's physical activity.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
Footnotes
-
Contributors MY carried out the data analysis, drafted the initial manuscript and reviewed the manuscript. JS took the lead in designing the Transform-Us! intervention and HB, DC, KDH, MJMC and EC contributed by designing the Transform-Us! intervention study. LA coordinated and supervised the data collection, provided the datasets to MY. All the authors commented on the conception of this manuscript and the data analysis plan, critically reviewed and revised the manuscript and approved the final manuscript as submitted.
-
Funding Transform-Us study is supported by a National Health and Medical Research Council (NHMRC) of Australia Project Grant (2009–2013; ID533815) and a Diabetes Australia Research Trust (DART) grant.
-
Competing interests The contribution of MY was funded by the Wereld Kanker Onderzoek Fonds (WCRF NL 2008/65), as part of the World Cancer Research Fund International grant programme and the IRSES (International Research Staff Exchange Scheme) programme of the 7th Frame Work programme of the European Commission. KDH is supported by National Heart Foundation of Australia (NHFA) Career Development Awards; VC is supported by Endeavour Research Fellowship; NDR is supported by an Australian Research Council Discovery Early Career Researcher Award; and JS is supported by a NHMRC Principal Research Fellowship (APP1026216). The funding bodies played no role in the study design; data collection, analysis, and interpretation; in the writing of the manuscript; or in the decision to submit the manuscript for publication.
-
Ethics approval The Deakin University Human Research Ethics Committee, the Victorian Department of Education and Early Childhood Development and the Catholic Education Office.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Deakin University has the rights to use the unpublished data from the Transform-Us! project and it is not open for data sharing.