Article Text

Abstract
Acetabular labrum tears (ALT) are present in 22–55% of individuals with hip or groin pain. Tears can occur as a result of trauma or degeneration and are markedly associated with femoral acetabular morphological variations. An ALT can lead to biomechanical deficiencies and a loss of stability to the coxafemoral joint due to the labrum serving as a stabilising structure of this joint. The diagnosis of ALT is complex and multidimensional. Although tremendous improvements in diagnostic utility for ALT have occurred in the past 25 years, there are few patient history, clinical examination and special test findings that are unique to the condition. Imaging methods such as MRI, CT and ultrasonography have demonstrated reasonable accuracy, but not at a level that allows use as a stand-alone measure. Outcomes measures that focus on functional limitation or that are used to measure recovery should envelop the complexities of the condition and be captured using both self-report and physical performance measures. Only when patient history, objective testing, clinical examination special testing and imaging are combined can a clinician fully elucidate the multidimensional diagnosis of ALT.
- Hip disorder
- Evaluation
Statistics from Altmetric.com
Introduction
The reported prevalence of acetabular labral tears (ALT) in patients with hip or groin pain ranges from 22% to 55%.1–4 Differential diagnosis of the hip joint poses a diagnostic dilemma, particularly given that pain in the hip region is often difficult to localise to a specific pathological structure. With the evolution of improved diagnostic imaging and advanced surgical techniques, examination of the hip joint and periarticular structures as a primary pain source for hip-related pain/dysfunction has received a significant increase in attention.5–7 Although limited information exists in support of diagnostic utility, emphasis on patient history, clinical examination findings, MRI, MRI arthrography (MRA) CT arthrography and anaesthetic intra-articular injection pain response is currently advocated for determining the presence of intra-articular hip joint pathology.8 Clearly delineating the specific pathology in the hip can be difficult,9 ,10 since patients visit multiple healthcare providers over an extended period of time prior to diagnosis of ALT.11 Additionally confounding the diagnostic process of the hip joint is a lack of consensus regarding what elements of the examination are considered essential.12 The purpose of this paper was to examine the most current evidence and provide a systematic approach (based on this evidence) for examination of patients with a suggestion of ALT.
Anatomy/biomechanics/epidemiology/mechanism of injury
The acetabular labrum is a fibrocartilaginous structure that lines the majority of the acetabular socket.13 Histologically, the labrum can be divided into capsular and articular portions.14 ,15 The capsular portion consists of dense connective tissue (collagen types I and III), whereas the articular portion consists of fibrocartilage (collagen type II)14 and is contiguous with the acetabular articular cartilage.16 Blood supply to the labrum enters from the capsule and supplies the outer 1/3 of the labrum.14 Pain-sensing free nerve endings are located most densely in the superior and anterior portions of the labrum, suggesting that it is a pain-generating structure.14 ,16
The acetabular labrum increases the articular surface area by 22% and acetabular volume by 33% and is believed to create a seal in the hip joint.16 Biomechanical analyses suggest that the labrum is stressed by a compressive load and extremes of hip joint motion.14 ,17 ,18 Therefore, a tear of the labrum alters physiological functions such as enhancement of joint stability and equitable load distribution.14
Acetabular labral tears are common and frequently asymptomatic; 96% of cadaver hips with a mean age of 78 years (range, 61–98 years) had ALT, with 74% of the tears located in the anterosuperior quadrant.16 Arthroscopic observations support the concept that femoroacetabular impingement (FAI), labral disruption, chondral lesions or combinations of each are frequently inter-related and part of a continuum of degenerative joint disease.18–21
Most ALTs are characterised by the insidious onset of symptoms. An increased prevalence of ALT has been shown to occur in athletes participating in tennis, ballet, hockey, football and soccer. The repetitive twisting and pivoting motions typically performed by these athletes in a flexed, weight-bearing position most likely create microtrauma, resulting in the eventual mechanical alteration of the joint.22
Five categories of ALT have been described based on aetiology: traumatic, congenital, degenerative, capsular laxity and idiopathic. Traumatic tears have an identifiable history and can involve additional acetabular trauma.13 Congenital tears are characterised by the presence of acetabular dysplasia.22 Degenerative labral tears are identified through radiographic evidence and often involve other degenerative changes of the joint.22 Capsular laxity can be divided into either global laxity (due to systemic connective tissue disorders) or focal rotational laxity known to occur in sports such as golf, hockey and baseball.23 In the absence of other findings, ALT are labelled idiopathic and are generally considered as a result of FAI or other bony abnormalities.22
FAI involves the abutment of the femoral head against the acetabulum in a hip flexed-adducted-internally rotated position, impinging the anterior–superior portion of the labrum.24 ,25 Other frequently described specific movements in athletics include sudden twisting or pivoting movements,18 as well as recurrent twisting or pivoting movements in moderate-hip flexion or extension without FAI.26 Recent findings suggest that while FAI is one of the primary predisposing factors to ALT,24 ,25 other conditions such as iliopsoas tendon impingement must also be considered.27 ,28
Examination
Subjective history
At present, the location of symptoms, history and clinical examination alone have proven inadequate in contributing to an accurate diagnosis of ALT.5 ,8 ,29 Since the diagnostic utility of these examination elements is limited, an emphasis on the summative patient history, clinical examination findings, MRI, arthrogram and anaesthetic intra-articular injection pain response is advocated for determining the presence of symptomatic ALT and other intra-articular hip joint pathology.8
The signs and symptoms of an ALT include anterior-groin pain that worsens with prolonged periods of standing, sitting or walking.24 Pain for these patients is predominantly in the groin,2 ,11 ,24 ,30 ,31 exhibiting a reported sensitivity (SN) between 96% and 100%.2 ,30 It has been estimated that between 22% and 55% of patients with groin or hip pain have ALT.24 Referred pain from ALT can also manifest in the buttocks and anterior thigh. Sharp pain often accompanied by mechanical symptoms such as clicking, giving way and hip pain are commonly associated with underlying ALT and cartilage defects,11 ,31 ,32 with a reported SN of 100%, and specificity (SP) of 85%.4 ,11 A labral tear was arthroscopically identified in 90% of individuals with mechanical hip symptoms.33
Outcome measures
Self-reported (outcome) measures are methods of having the patient assess their pain and function. These measures can be region-specific (hip), condition-specific (ALT), dimension-specific (pain), generic (health profile) or individualised to the patient.34 It has previously been recommended that function at the level of the person can be carried out using standardised, psychometrically sound outcome measures complemented by standardised, psychometrically sound physical performance task batteries.35 Indeed, outcome measures are valuable in defining the patient's perspective of their change but have been shown to differ substantially from physical performance measures (PPMs) that involve quantification of output, and are dramatically influenced by changes in pain.36–39 In other words, the patient's perception of their functional ability was inflated in instances of decreased pain. Outcome measures are clearly important, but determining recovery from a single self-report measure or drastically changing a treatment intervention is not warranted since a self-report finding serves only as one element of the assessment for a patient with ALT. Additionally, it has been suggested that no conclusive evidence supports a single patient-reported outcome measure questionnaire for the evaluation of patients undergoing hip arthroscopy.40
A recent systematic review examined various commonly used outcome measures for non-arthritic hip pathology. The Hip-Outcome Score had the highest positive rating for internal consistency, construct validity, agreement, responsiveness, lack of floor/ceiling effect and interpretability. The Non-Arthritic Hip Score showed evidence for validity and lack of floor/ceiling effect. The modified Western Ontario and McMaster Universities Osteoarthritis Index was only strong for internal consistency and was indeterminate for construct validity. Further clinimetric evaluation of these commonly used measures was suggested.41
A newly developed tool, the 33-item International Hip Outcome Tool (iHOT-33), has been suggested as a primary outcome measure for ALT patients due to its development following large sample sizes and the most rigorous methodology. This questionnaire uses a visual analogue scale response format designed for computer self-administration by young, active patients with hip pathology. iHOT-33 has been shown to be reliable, has demonstrated face, content and construct validity, and is highly responsive to clinical change.42
A short version of the International Hip Outcome Tool has been developed. It has very similar characteristics to the original rigorously validated 33-item questionnaire, losing very little information despite being only one-third the length. It is valid, reliable and responsive to change. It has been suggested to be used for initial assessment and postoperative follow-up in routine clinical practice.43
The Copenhagen Hip and Groin Outcome Score (HAGOS) has also been suggested for the assessment of symptoms, activity limitations, participation restrictions and quality of life in physically active, young-to-middle-aged patients with long-standing hip and/or groin pain. HAGOS consists of six separate subscales assessing pain, symptoms, physical function in daily living, physical function in sport and recreation, participation in physical activities and hip and/or groin-related quality of life. It is also a valid, reliable and responsive to change measure. This measure is suggested for use in interventions where the patient’s perspective and health-related quality of life are of primary interest.44
Diagnostic imaging
Diagnostic imaging, like each component of the examination for potential ALT, provides relevant and valuable information for the clinician (table 1). Not unlike other portions of the examination of the hip joint, diagnostic imaging requires careful interpretation on the part of the clinician. Several studies have found hip pathological changes, such as ALT and FAI, in asymptomatic individuals.45–49 Additionally, as noted in table 1, all diagnostic imaging modalities are imperfect. Therefore, imaging should be used to confirm clinical findings and should not be used in the absence of appropriate signs and symptoms not reflective of ALT. The clinician should correlate patient symptoms with history and physical examination when evaluating patients with hip pain and diagnostic imaging abnormalities.
Diagnostic accuracy of diagnostic imaging tests for pathologies including or relevant to an acetabular labral tear
Radiographs
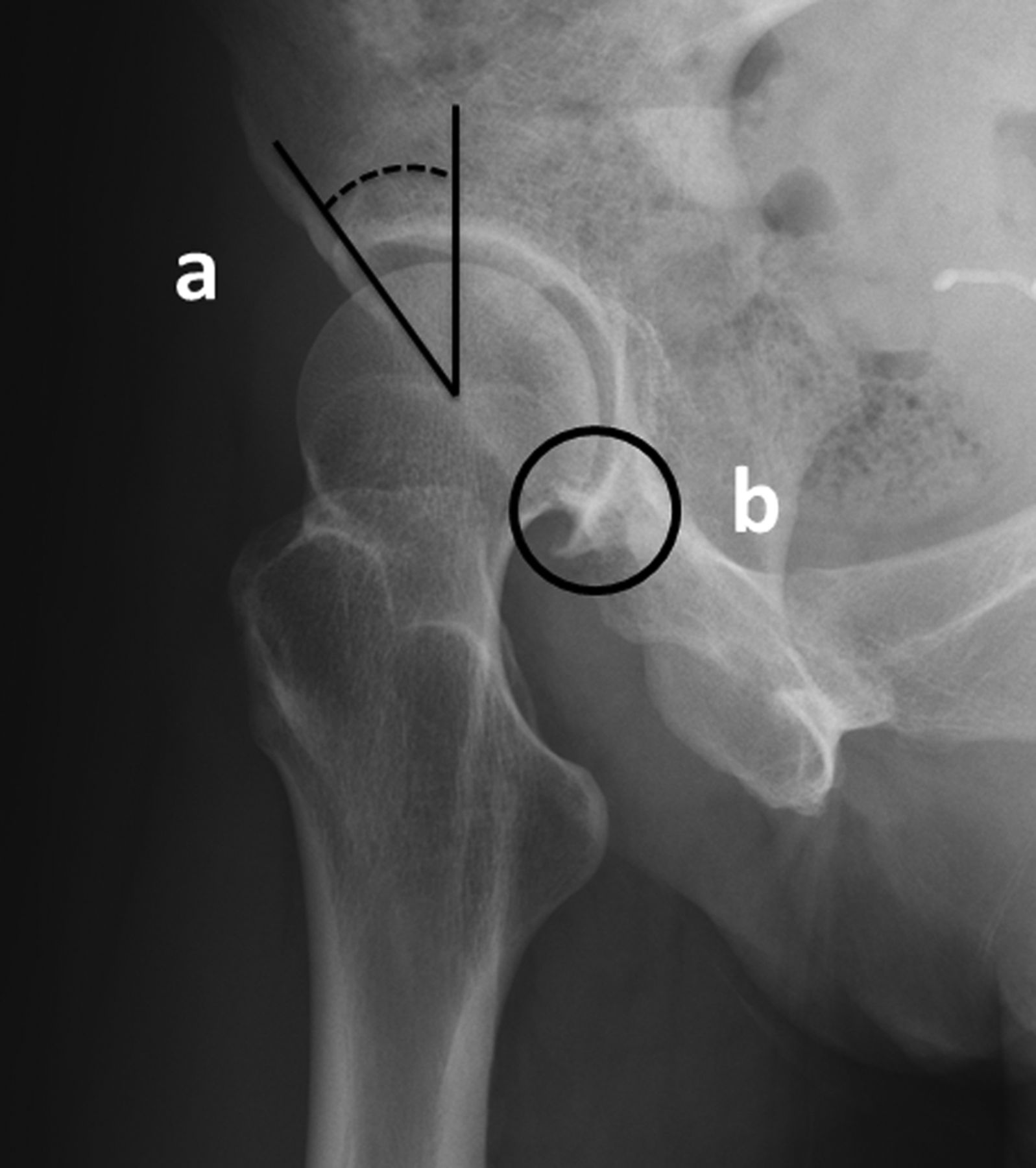
Imaging of the painful hip should begin with radiographs, including at a minimum a weight-bearing AP projection of the pelvis and a lateral projection of the symptomatic hip. There are many lateral projections, including the frog-leg lateral, Dunn lateral (figure 1) and modified Dunn lateral projections. The frog-leg lateral projection is obtained with the hip flexed and abducted 45°. The Dunn lateral projection is obtained with the hip flexed 90° and abducted 20°. The modified Dunn lateral projection is obtained with the hip flexed 45° and abducted 20°.

Dunn lateral radiograph demonstrating α angle.
In patients with a suspected ALT, radiographs should be analysed for abnormal morphology of the acetabulum and femoral head, including anatomy predisposing to FAI and acetabular dysplasia. Radiographs can also reveal alternative causes of hip pain, including advanced osteoarthritis, femoral head avascular necrosis (AVN), fracture and osseous lesions; MRI is more sensitive in the detection of AVN, non-displaced fracture (including stress fracture) and osseous lesions.
FAI is due to the abnormal morphology of the hip, on the side of the femur, the acetabulum or both. Abnormal morphology of the femur is categorised as cam FAI. Abnormal morphology of the acetabulum is categorised as pincer FAI. The most common pathomorphology is a combination of both, the so-called mixed FAI.50 ,51 The pathomorphologies create a pathological ‘conflict’, or contact, between the femur and the acetabulum during normal and/or extreme ranges of motion.
Cam FAI morphology is more prevalent in young males.52 ,53 Asphericity of the femoral head–neck junction, typically anterolateral in location, predisposes to abnormal contact between the femur and the acetabulum. The abnormally shaped femur typically results in tearing at the anterosuperior chondrolabral junction and delamination and other damage to the adjacent cartilage.50 ,54
Cam FAI morphology is evaluated on the anteroposterior (AP) pelvis radiograph as well as the lateral hip projection(s). Normally, there is a concavity (also called ‘cutback’) of the lateral femoral head–neck junction. A convexity (asphericity) of the lateral head–neck junction on the AP pelvis radiograph is abnormal and called a pistol-grip deformity (figure 2), morphology predisposing to cam FAI.55

Pistol grip deformity on anteroposterior radiograph.
On the lateral hip projection(s), a lack of a normal cutback of the femoral head–neck junction, also called insufficient head–neck offset, can be more readily appreciated, as the majority of patients have femur pathomorphology located anterolaterally. There are many quantitative means to evaluate the insufficient offset, the most well described one being the α angle. The α angle is defined as the angle between a line through the centre of the femoral head that parallels the femoral neck and a line from the centre of the femoral head to the point where there is deviation of a best-fit circle of the head and the adjacent proximal femur (figure 1). The α angle can also be measured on AP and cross-table lateral radiographs. An abnormal α angle is typically considered to be one that is greater than 50°–55°;56 ,57 higher angles have even more SP in discriminating subjects with pathology and controls, reducing the possibility of false-positive results.58 ,59
It is not uncommon to see a small round or ovoid lucency (or cluster of lucencies), usually with thin, sclerotic margins, adjacent to the site of insufficient offset at the head–neck junction; this lucency or cluster of lucencies is called by many names, including focal fibrocystic change, a synovial herniation pit or after the original published author of the finding, a Pitt's pit (figure 3).60 ,61 These may be due to the focal intrusion of synovial fluid or intraosseous ganglia formed during repeated episodes of abnormal contact of the femur with the acetabulum. They are more commonly seen in patients with cam FAI morphology, although they can also be seen in pincer FAI morphology.62

Dunn lateral view demonstrating fibrocystic change (circled) associated with femoroacetabular impingement morphology.
Pincer FAI morphology has a higher prevalence in middle-aged women.63 Abnormal coverage of the acetabulum of the proximal femur predisposes to abnormal contact. Abnormal coverage can be complex and/or either focal or global.
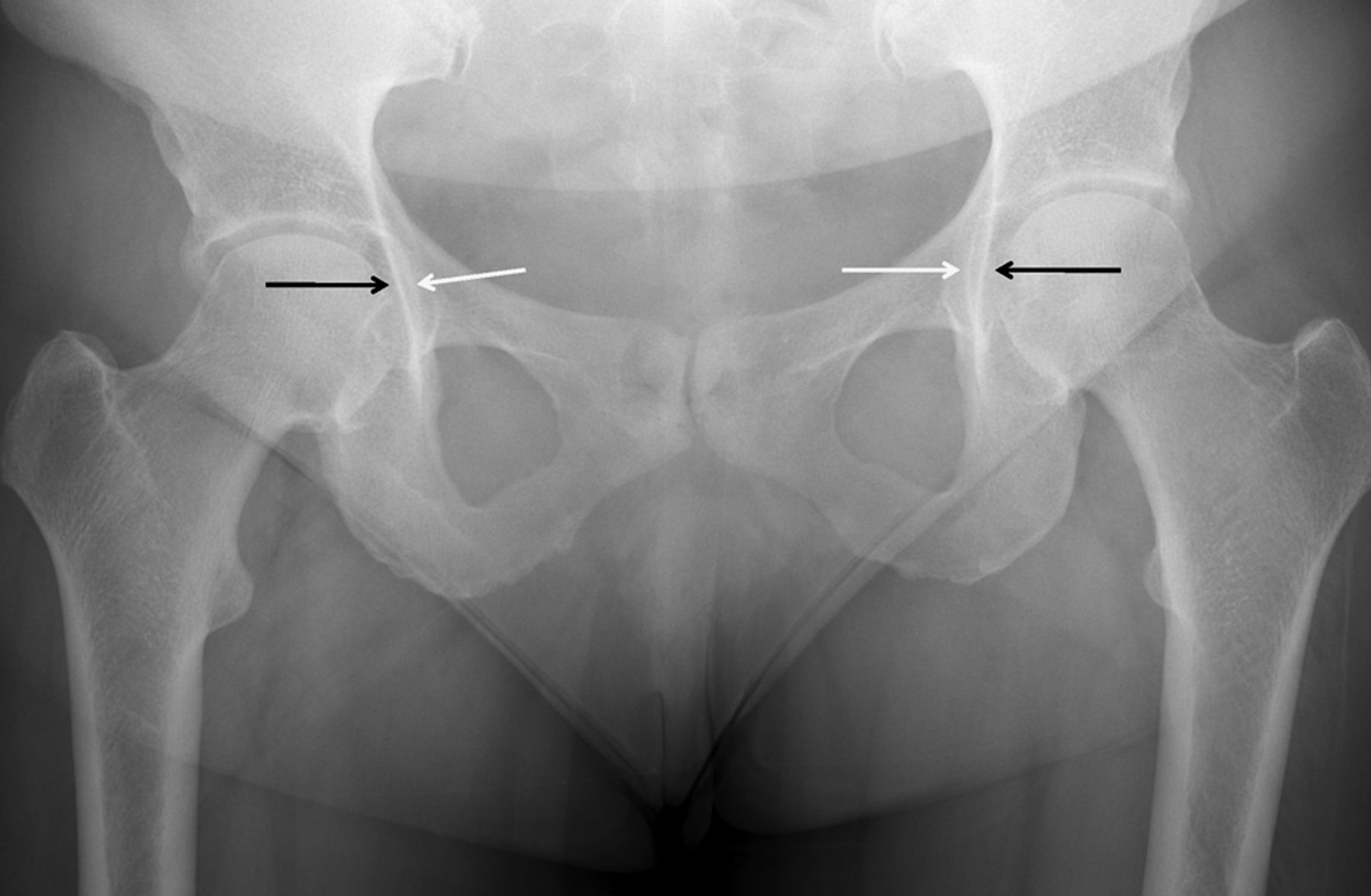
The AP pelvis radiograph is well suited to evaluate for pincer FAI, affording determination of the depth of the acetabulum. Global acetabular overcoverage can vary in extent; acetabuli protrusio is present if the medial femoral head abuts or extends medially to the ilioischial line and coxa profunda exists if the medial acetabular wall, but not the femoral head, extends medially to the ilioischial line (figure 4). The extent of acetabular coverage can also be assessed using the lateral centre-edge angle of Wiberg (LCEA); this angle is formed from a vertical line through the centre of the femoral head and a line from the centre of the femoral head to the lateral margin of the superior acetabulum. Acetabular overcoverage is defined as an LCEA 40° or greater.64 It is important to note that if there is a pelvic tilt, the vertical line must be drawn perpendicular to the pelvis (eg, perpendicular to a horizontal line connecting the tips of the ischial tuberosities).
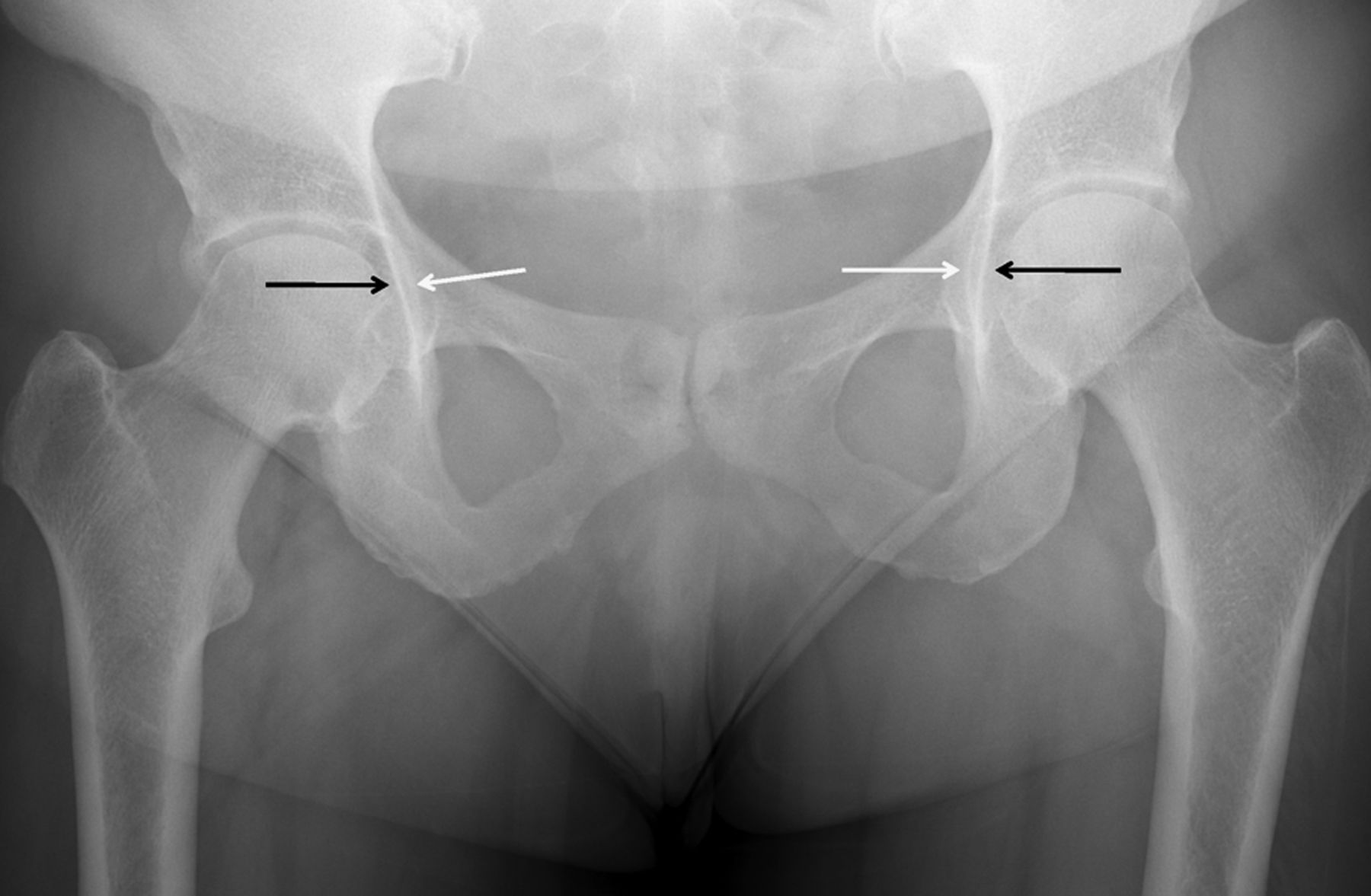
Anteroposterior pelvic radiograph demonstrating coxa profunda, where the medial acetabular wall (arrows pointing laterally), but not the femoral head, extends medially to the ilioischial line (arrows pointing medially).
Focal or global acetabular retroversion can also be assessed on the AP pelvis radiograph. The posterior wall of the acetabulum is normally lateral to the anterior wall on the AP projection. If the anterior wall extends laterally to the posterior wall superiorly, there is cranial acetabular retroversion, predisposing to pincer FAI; this is a so-called crossover or figure-of-eight sign (figure 5).64–67 Global acetabular retroversion exists when the entire anterior wall is lateral to the posterior wall.

Anteroposterior radiograph demonstrating a crossover sign; superiorly, the anterior wall of the acetabulum (dashed line) ‘crosses over’ the posterior wall (solid line).
A false-profile hip projection can be used to assess for abnormal anterior acetabular coverage. A false-profile projection is obtained with the hip of interest rotated 65° (posterior oblique) while standing. An anterior centre-edge angle can be performed, analogous to that for LCEA (figure 6). Abnormal anterior overcoverage is similarly defined by an angle equal to greater than 40°.64
False-profile view demonstrating an anterior centre edge angle (A) and a posteroinferior osteophytosis and joint space loss (B), signs of chondral loss typically seen in pincer femoroacetabular impingement.
In a study utilising CT examining 135 patients, Dolan et al68 found that 90% of patients with labral tears had FAI morphology. Seventy-six per cent of patients had α angle greater than 50°, whereas 43% had acetabular retroversion and 89% had an elevated LCEA.
It is important if there are signs of advanced cartilage loss in the hip, as advanced chondrosis portends an unfavourable outcome of FAI surgery and a significant need for conversion to total-hip arthroplasty (THA).69 A subchondral cyst in the acetabulum and/or femoral head usually denotes overlying high-grade chondral loss and is thus important to note.63 ,70 Additionally, while joint space width is affected by many factors, including pelvis orientation and radiographic beam angulation, a joint space width of 2 mm or less, a surrogate for advanced chondral loss, has a high association with the eventual need for THA.71
In contradistinction to pincer FAI, patients with acetabular dysplasia have an abnormally small LCEA (20° or less).72 Owing to the abnormally low coverage of the femoral head by the acetabulum in these patients, there are increased stresses on the anterosuperior labrum and adjacent cartilage leading to premature degeneration and tearing of the labrum and chondral loss.73 ,74
MRI
MRI has excellent soft tissue contrast, thus affording excellent visualisation of the fibrocartilaginous acetabular labrum. ALTs are diagnosed when a signal is present at the base of the labrum or within the labrum itself. ALTs can also be diagnosed if there is a displaced flap of the labral tissue or if there is an irregular contour and morphology. If present, a paralabral cyst (a small collection of fluid communicating with the labrum or the cartilage-labral junction) is pathognomonic of a labral tear.5 ,75 In addition, measures of insufficient femoral head–neck offset (eg, α angle) and acetabular overcoverage (eg, LCEA) or retroversion can be measured with MRI as previously discussed with radiographs.
MRI is traditionally and commonly performed with intra-articular contrast material (ie, MRA), creating distention of the joint. With appropriate pulse sequence selection, MRI without intra-articular contrast can be performed for the evaluation of ALTs, particularly with greater signal-to-noise ratios afforded by higher strength magnets (ie, 3 Tesla). Less commonly, ALTs can also be diagnosed with MRI after the intravenous administration of gadolinium. The SN, SP and accuracy of MRI in the diagnosis of ALTs is generally good to excellent (table 1).
MR detection and grading of chondral loss/defects are more limited. There is not a dedicated hip surface coil thus there is a resultant lower signal-to-noise ratio and more magnetic field inhomogeneity when imaging the hip, particularly in larger patients. Additionally, the cartilage over the acetabulum as well as femoral head is thin (1–2 mm thick) and imperfectly quantified by MRI,76 making detection of loss more difficult. Also, the surfaces of both the femoral head and, largely, the acetabulum are curved, making the detection and grading of chondral loss yet more difficult. Owing to these limitations, the SN, SP and accuracy of cartilage detection and grading are only fair to good (table 1).
Multidetector CT
Multidetector CT (MDCT) is less frequently used for evaluation of ALTs and chondral loss. As MDCT has much lower soft tissue contrast resolution than MRI, it must be performed with intra-articular contrast to outline the articular surfaces and the labrum. MDCT has excellent spatial resolution, higher than MRI. Additionally, MDCT is obtained in significantly less time than MRI. As compared with MRI, it can be performed in claustrophobic patients. It can also be performed in patients with certain implanted devices that are contraindicated in MRI (eg, pacemakers). However, MDCT does involve ionising radiation, unlike MRI.
As compared with MRI in the evaluation of ALTs and chondral loss, there have been significantly fewer studies evaluating SN and SP with MDCT. In general, the SN of MDCT is excellent in the detection of ALTs (table 1). In the few studies evaluating the detection and grading of cartilage loss, the results have been as good as, if not better than, with MRA.
Ultrasound
In comparison to MRI and MDCT, much fewer studies have been performed evaluating the detection of ALTs with ultrasound (US). The SN of ALT diagnosis is significantly less than with MRI or MDCT. While US involves no ionising radiation and does not require the intra-articular administration of fluid, it is highly operator-dependent, cannot be used to evaluate the posterior labrum and cannot be used to evaluate the cartilage. While there are two studies investigating the diagnostic accuracy of US compared with MRA as a criterion reference for ALT,77 ,78 only one study,79 with moderate SN and SP has investigated the use of US for this diagnosis while using a criterion reference of surgery (table 1).
Observation
The patient with synovitis or inflammation may often purposively position their hip in a flexed, slightly abducted and externally rotated position, as this position places the hip capsule at its largest potential volume.80 ,81 Since these conditions can be common with ALT, the clinician should monitor for such positioning. The patient with these conditions is also likely to avoid full hip extension during gait since this is the position of least hip capsule volume and greatest joint force on the anterior labrum during gait.3
Combined motions of hip flexion and adduction have been shown to cause the greatest magnitude of strain on the overall labrum.17 In fact, the impingement position of hip flexion, adduction and internal rotation not only increases labral strain, but has also been shown to cause complaints of pain in patients with hip intra-articular pathology.4 Therefore, the patient with synovitis or inflammation may demonstrate pain posturing when sitting in chairs (especially lower level chairs), stepping up with the involved leg or squatting as these motions will replicate the combinations of these movements in the hip. Although squatting with externally rotated lower extremities most likely limits the mechanical abutment of the femoral head on the acetabulum, greater strains on the labrum were detected in external rotation versus neutral rotation and internal rotation in a cadaveric model.17
Findings supporting decreased gluteal muscle performance and ALT3 suggest that functional limitations may also be found in the propulsion phase of gait, standing up out of a chair, climbing a steep hill or incline and pushing off into a sprint. Recent findings suggest that marked gluteal muscle performance deficits are necessary to ascertain such functional limitations; thereby implying that detection of such impairments may have limited applicability to those without marked gluteal weakness.82
Observation of a running pattern is of particular importance for the athletic patient. Increased compressive loads and demands for increased eccentric muscular control are required of the athlete with running as compared with walking. Irregularities in running style can lead to altered force displacement and increased stress on the hip joint.83
Triage/screening
Signs of more serious pathology are referred to as ‘red flags’, and it is at this point that the clinician must decide on whether or not to continue with the examination. Suspicion of non-musculoskeletal pathology warrants additional diagnostic imaging, lab testing, potential referral to another healthcare provider or at least caution with continued examination of the hip joint.
Pain in the region of the hip joint can be derived from a number of referred sources. The lumbar spine, pelvic girdle, abdominal viscera and peripheral nervous system are just some of these possible sources. Lumbar radiculopathy referral patterns can involve the posterior hip, iliac crest and anterior thigh/groin (particularly the lumbar nerve roots 1 and 2). The clinician should always be cognisant of pain unrelieved by rest and/or change of positions, night pain, fevers, chills and unexplained weight loss as these signs and symptoms are suggestive of non-musculoskeletal dysfunction.
The clinician must be aware of disorders affecting the abdominal and pelvic organs that can also refer pain to the hip region, mimicking a musculoskeletal dysfunction. A history of cancer, such as prostate cancer in men or breast cancer in women, is a red flag since these cancers may be associated with metastases to the lumbar spine and/or hip joint.84 Pain that is more related to the pelvis and coincides with menstruation may suggest symptomatic ovarian cysts and/or endometriosis,85 ,86 whereas pain that radiates to the testicle in men can indicate urological pathology.87
The clinician should also be aware of other variables, such as previous history of surgeries to the hip or proximal lower extremity, previous abdominal or pelvic organ surgery, insidious onset of pain, symptoms unchanged by position or movement, symptoms related to a woman's menstrual cycle, neurological or vascular diseases, acute hip pain with fever, malaise, night sweats, unexplained weight loss, intravenous drug use, night pain unrelieved by position change, compromised immune system, a history of corticosteroid exposure or alcohol abuse (risk for AVN) and previous history of cancer as aforementioned.84 ,88 ,89 An awareness of these potential red flag concerns can assist the clinician in identifying the need for additional medical intervention.
Fracture or stress fracture to the femur should also be ruled out at this point in the examination for those patients with high suspicion of this pathology.90–94 The patellar-pubic percussion test (tables 2 and 3) has demonstrated excellent SN (95%) and SP (86%) across three different studies with the ability to moderately influence post-test probability of a fracture.9
Diagnostic accuracy of suggested HPE tests for pathologies including or relevant to an acetabular labral tear
Description of suggested physical examination tests for diagnosis of an acetabular labral tear
Once red flags are ruled out, an efficient way to begin to differentiate the many potential pain referral sources is through the lower quarter screening examination. The traditional lower quarter screen consists of testing of dermatomes, myotomes, deep-tendon reflexes and possible upper-motor neuron involvement. Typically, a screening examination should be composed of tests with high SN.95 Since the traditional neurological ‘screen’ includes tests that are primarily SP rather than SN,96 a positive test would implicate pathology versus ruling it out.
The next part of the lower quarter screen consists of ruling out other, potentially relevant sources of pain. These most likely sources include the lumbar spine and pelvic girdle.
Ruling out pain generation from other related structures: lumbar spine and pelvis
When examining the hip joint, the clinician should differentially diagnose the potential contribution of the sacroiliac joint (SIJ)/pelvic girdle and lumbar spine as the primary pain generator for the patient's hip pain. Screening tests for these areas are employed to limit the extent of the differential diagnosis for pathology contributing to the patient's hip pain. A systematic approach to ruling out these other areas is suggested. The key points of this approach are listed here, but the reader is referred to the specific references listed for additional detail.
Rule out lumbar spine
Radiculopathy-related/discogenic-related pathology can be ruled out with a combination of tests, including repeated motions of the lumbar spine, straight leg raise (SLR) test and slump test. The patient repeatedly flexes, extends and sidebends the lumbar spine between 5 and 20 repetitions, looking for a trend in change of symptoms. Repeated flexion may cause the pain to peripheralise (move away from the centre of the back/hip down the leg), whereas repeated extension may cause the pain to move towards the centre of the low back (centralise) if the pain is due to radiculopathy/discogenic-related pathology. In separate studies, repeated motions were found to be SN (92%)97 as well as SP (94%).98 Since both these studies were of high quality and with a low risk of bias, the clinician can feel relatively confident in ruling out radiculopathy-related/discogenic-related pathology with this testing.
Additional tests to help rule out the lumbar spine as a primary-pain generator would include the SLR (SN 97%)99 and slump tests (SN 83%)100 to help rule out radiculopathy/discogenic pathology and the seated extension-rotation test (SN 100%)101 ,102 to rule out facet joint dysfunction. Facet joint dysfunction can be implicated (SP 95%) with posteroanterior joint play assessment.103 All these studies were of high quality, with a low risk of bias, thereby again providing the clinician with increased confidence in ruling out/in lumbar spine pathology.
Rule out SIJ/pelvic girdle dysfunction
Owing to the complexity and controversial nature of SIJ/pelvic girdle dysfunction with limited amounts of movement in this region,104 pain provocation cluster testing is suggested.105 If the discogenic origin of pain was ruled out, a pain provocation cluster of tests exhibited (three of five required to be positive) an SN of 94% and an SP of 78% in a high quality, low-risk bias study.106 The thigh thrust test demonstrated the strongest screening ability (SN 88%).106
Motion tests
Common patterns of lower extremity ROM deficits are often noticed in patients with FAI and ALT. Most notably, patients tend to exhibit reduced hip motions of flexion, internal rotation and/or adduction.11 ,51 ,107–109 In the younger athlete with suspected slipped capital femoral epiphysis (SCFE), the clinician should monitor for the presence of a Drehmann sign with passive hip flexion. The Drehmann sign is a characteristic clinical feature in SCFE, indicating obligatory hip external rotation and abduction with hip flexion. This sign has been suggested to be clinically valuable when examining for the existence of FAI in patients with SCFE.110
Additionally, since the greatest strain on the labrum is in hip flexion and adduction,17 assessment of hip joint mobility is suggested. Hip anteroposterior glide (motions of hip flexion and internal rotation; figure 7) and lateral glide (hip adduction) are of primary importance for assessment.111 ,112

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Hip anteroposterior glide.
Functional limitations can be correlated with hip ROM limitations. Hip flexion ROM was shown to explain up to 95% of variance in the star excursion balance test (SEBT) performance.113 SEBT, a PPM discussed later, has demonstrated discriminatory ability to predict future lower extremity injury.114
Muscle performance testing
Hip muscle performance deficits have been demonstrated in patients with symptomatic abnormal pathology of FAI,115 as well as osteoarthritis.116 Therefore, a comprehensive muscle performance assessment of the hip should be performed when examining for ALT. Of particular importance is the assessment of the gluteal muscles.3 Gluteus medius minimus and maximus weakness during hip extension, as well as weakness of the iliopsoas during flexion resulted in an increase in the anterior hip joint force.3 Theoretically, these hip muscle deficits and subsequent increases in the anterior hip joint forces could lead to ALT.3
Patients with symptomatic FAI have considerable hip-muscle weakness and demonstrate an impaired ability to produce maximal hip strength when compared with healthy controls.115 Gluteus medius and maximus muscle weakness116–118 and atrophy116 ,119 ,120 have been correlated with hip joint osteoarthritis. Although the gluteus medius does increase compression forces on the hip, it also stabilises the contralateral pelvis as a result of this compression.121 In a patient with gluteus medius weakness, demonstrating a Trendelenberg gait pattern, increased compressive forces will be encountered in the involved hip as a result of the increased length of the lever arm this muscle has to function across.122
Special tests
At this point in the examination (after the red flags and potential contribution from the lumbar spine and pelvic girdle have been excluded), it is advised that the examination focus on ALT confirmatory tests. Caution is suggested though, since the majority of these individual tests have limited ability to confirm pathologies of the hip.9 ,10 ,123 Hip ALT tests are generally more SN than SP, thus providing more clinical utility as screening tests than confirmatory tests.9 In addition, the prevalence of disease in a population can markedly affect screening test performance; in low-prevalence settings, even very good tests with high SN may provide only limited post-test probabilities for ruling out a diagnosis.95 The vast majority of studies that have investigated ALT tests were performed on cohorts with a high suspicion of ALT, most likely artificially increasing the post-test utility (especially SN).
Suggested testing for ALT is listed in table 2. The majority of these tests attempt to replicate the primary mechanism of ALT (flexion and twisting).24 ,25 The test with the strongest diagnostic accuracy (Thomas test) replicates the position of greatest force on the hip joint capsule (extension),3 as well as the position where the majority of ALT are located (anteriorly).124 Additionally, as previously mentioned, iliopsoas muscle pathology has more recently been discerned as a potential contributor to ALT. While this test is traditionally used to expose iliopsoas muscle tightness, reproduction of the patient's painful click or groin pain is considered as a positive test for ALT, loose bodies or arthritic changes of the hip.2 Therefore, the Thomas test can be utilised to indicate intra-articular pathology instead of the traditional interpretation of hip flexor flexibility.
Other tests meeting eligibility for meta-analysis were the flexion-adduction-internal rotation (FADDIR) test and the flexion-internal rotation test.9 Both these tests replicate motions of the hip most likely to create a mechanical abutment of the femoral head against the acetabulum, or FAI.24 ,25 The FADDIR test has been investigated for FAI as well as ALT, whereas the flexion-internal rotation test has predominantly been specified as an ALT assessment. Since both these tests demonstrate much stronger SN than SP, their clinical utility as screening tests overshadows their utility as confirmatory tests for ALT. Therefore, a negative result with either of these tests provides greater value than a positive result. When diagnosing a condition such as ALT, this is not dependable clinical practice.
Several other tests have been described for the assessment of ALT, including the scour test,125 internal rotation with overpressure test,125 resisted SLR test,125 internal rotation-flexion-axial compression test4 and the posteroinferior labrum test.126 All these tests generally demonstrate greater SN than SP. Additionally, none of these tests demonstrate likelihood ratios of value to alter the post-test probability of ALT diagnosis greater than to a small degree.127 For specific detail on the diagnostic accuracy of these additional tests, the reader is referred elsewhere.9 ,10 ,123
Palpation
The clinician should palpate the relevant lumbar spine, pelvis and hip structures when assessing for ALT. Although pain referral for ALT is typically to the groin, and to a lesser degree the buttock and lateral trochanter,31 these areas of the hip are typically not tender to palpation unless there is also extra-articular involvement. Owing to the recent findings implicating the psoas major as a potential contributor to ALT pathology,27 ,28 palpation of this structure for concordant pain is merited.
Physical performance measures
As with the other components of the examination process, PPMs have limitations. Presently, studies that have investigated the criterion validity of PPMs are underwhelming since most have compared PPM with other more widely used means of testing (self-report measures and special tests). The correlation between these different types of testing is not always favourable. Furthermore, some of these comparisons are against tests that have no proven validity. Therefore, while many of the PPMs investigated have proven to be highly reliable when used for patients with knee or ankle pathology, the validity is still questioned.128
As with PPMs in other areas of the body, the selection and utilisation of these tests should be from the least challenging to the most challenging to the patient. Some lower level tests, such as squatting for depth, can easily be integrated in earlier parts of the examination process, namely observation.
A recent systematic review129 supports the use of the single-leg stance, single-leg squat and SEBT for patients with hip pathology. Patients with FAI had decreased mean peak squat depth compared with controls, suggesting that maximal squat depth is a valid measure of assessment for FAI.130 SEBT, a purported measure of balance, ROM and muscle performance113 ,114 ,131 recruited the gluteus medius at 49% of maximal volitional isometric contraction with a medial reach.132 The single-leg squat also demonstrated a relationship to hip abductor function.133 Dysfunction in any of these PPMs should alert the clinician to perform measures previously discussed (motion tests, muscle performance tests and so on).
Normative and discriminatory values for involved to non-involved lower extremities on various hop, speed and agility tests have been reported.134 Most of these tests are reported for either normative values or in knee and ankle pathologies. The reliability of these measures specifically for hip dysfunction has not been established.
The ‘Sport Test’ has been advocated to objectively assess a patient's readiness to return to sport following hip arthroscopy. Rather than measuring isolated movements, it analyses an individual's coordinated movement patterns and power of an involved extremity. The Sport Test includes single knee bends, side-to-side lateral movement, diagonal side-to-side movement and forward box lunges. Patients must score 17/20 or higher to pass each of the four components of the test.135 Although the application of this test on those with ALT has not been investigated, it would be within reason to assume that this test could ideally function as an advanced assessment of sport-related ability for these patients since it replicates most components of sporting activity. Determination of return to sport prediction and diagnostic accuracy is a limitation of these tests though.
Conclusion
Although the prevalence of ALT is much higher than originally thought, identification of this complex, multifactorial condition requires a dedicated examination of patient history, pertinent objective findings, adequate special clinical tests and imaging confirmation. The potential relationship of ALT with FAI must be considered as should those associated with degenerative processes. No single patient history or clinical examination findings are ‘stand-alone’ in their ability to diagnosis ALT, whereas the benefits of CT, MRI-A and US can provide great promise when complemented with clinical findings. Measurement of functional status or recovery is also a composite construct and is best performed using both self-report and PPMs. Future studies should investigate the benefits of clustering clinical findings and investigating the diagnostic accuracy of tests and measures in situations of more accurate prevalence. Indeed, although each component of the examination for ALT is wrought in imperfection, utilisation of a comprehensive, systematic approach as described will minimise these shortcomings.
What are new findings?
-
The prevalence of acetabular labral tears (ALT) is higher than originally believed, yet the examination for its existence is still lacking in significant diagnostic accuracy.
-
Owing to the multifactorial nature of an ALT, the examination process requires a committed and comprehensive examination approach (eg, subjective history, self-report measures, objective examination, diagnostic imaging, muscle and joint performance measures, special testing, etc).
-
Reliance on a single component of the described examination is not sensible clinical practice.
References
Footnotes
-
Contributors All authors provided substantial contributions to the conception and design, acquisition of data or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content and final approval of the version to be published.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com