Article Text

Abstract
Objective To evaluate the time course of the recovery of transverse strain in the Achilles and patellar tendon following a bout of resistance exercise.
Methods Seventeen healthy adults underwent sonographic examination of the right patellar (n=9) and Achilles (n=8) tendons immediately prior to and following 90 repetitions of weight-bearing quadriceps and gastrocnemius-resistance exercise performed against an effective resistance of 175% and 250% body weight, respectively. Sagittal tendon thickness was determined 20 mm from the enthesis and transverse strain, as defined by the stretch ratio, was repeatedly monitored over a 24 h recovery period.
Results Resistance exercise resulted in an immediate decrease in Achilles (t7=10.6, p<0.01) and patellar (t8=8.9, p<0.01) tendon thickness, resulting in an average transverse stretch ratio of 0.86±0.04 and 0.82±0.05, which was not significantly different between tendons. The magnitude of the immediate transverse strain response, however, was reduced with advancing age (r=0.63, p<0.01). Recovery in transverse strain was prolonged compared with the duration of loading and exponential in nature. The average primary recovery time was not significantly different between the Achilles (6.5±3.2 h) and patellar (7.1±3.2 h) tendons. Body weight accounted for 62% and 64% of the variation in recovery time, respectively.
Conclusions Despite structural and biochemical differences between the Achilles and patellar tendon, the mechanisms underlying transverse creep recovery in vivo appear similar and are highly time dependent. These novel findings have important implications concerning the time required for the mechanical recovery of high-stress tendons following an acute bout of exercise.
Statistics from Altmetric.com
Introduction
Little is known about the adaptive response of human patellar tendon to loading. Originally considered metabolically inert, recent studies have shown acute loading of human tendon results in increased intratendinous glucose uptake, oxygen consumption, blood flow and collagen turnover in peritendinous tissues and the expression of certain genes, growth factors and mediators of inflammation.1–6 However, the effect of loading on the mechanical properties of tendon is less clear. While most studies have observed that habitually active individuals possess larger tendons (20–36%) than their untrained counterparts,7–9 prospective studies have shown that exercise training either increases,10–12 decreases13 ,14 or has no effect on measures of tendon stiffness and modulus in vivo.15–17 These studies have, however, typically evaluated the effect of exercise training on the ‘elastic’ properties of tendon (ie, stiffness and modulus), and have largely overlooked the ‘viscous’ component of tendon behaviour. Like many human tissues, tendons are known to exhibit viscoelastic behaviour and sustained static or cyclic loading has been shown to result in increasing strain or creep in tendon.18
With the advent of high-resolution ultrasound systems, recent in vivo studies have noted an immediate decrease in the thickness of human tendon after bouts of cyclic resistance exercise and following activities involving prolonged walking and running.19–24 Equating to transverse strains (TSs) of around 10–20% in vivo, this acute change in thickness has been hypothesised to reflect fluid movement associated with load-induced alignment of the solid phase of the tendon matrix and is consistent with creep behaviour reported with ex vivo testing of animal soft tissues, albeit in a transverse rather than in an axial direction.18 ,25–27 While the creep response in soft tissues has been associated with reduced muscular activity and electromechanical delay and has been implicated in the development of overuse injuries,14 surprisingly little is known about the time course of the creep recovery of soft tissues following exercise. Of the few studies undertaken to date, most have investigated the axial creep recovery of the intervertebral disc in vitro and have observed that full recovery of the disc occurs only when the unloaded recovery time is one to several orders of magnitude longer than loading.26 ,28 ,29
To the best of our knowledge, however, no study has evaluated the postexercise recovery of human tendon in vivo. Characterising postload recovery is not only important for understanding the unloaded tendon but is also critical to understanding tendon behaviour under subsequent loadings. The aim of this study, therefore, was to characterise and compare the time course of the postexercise recovery in TS in the Achilles and patellar tendon in vivo. These tendons are thought to function as elastic-energy-storage springs during locomotion and in addition to experiencing relatively high stress levels during activities of daily living are prone to chronic ‘overuse’ injury and degenerative change.30 ,31 We hypothesised that, as with other human soft tissues, full recovery of the Achilles and patellar tendons would occur within 24 h following exercise and that recovery times would not differ between tendons.
Methods
Subjects
Seventeen healthy adults were recruited from university faculty to participate in this repeated measures study, which received approval from the institutional review board. Study exclusion criteria included a medical history of diabetes, inflammatory joint disease, familial hypercholesterolaemia or lower limb tendon pathology. No participants were excluded. All participants were non-medicated, non-smokers and recreationally active based on self-report and presented to the laboratory having abstained from physical activity in the previous 24 h. Participant numbers were based on previously published data for human Achilles tendon19 and were sufficient to detect a 10% difference in the immediate TS response of the two tendons (α=0.05, β=0.20). Body height was measured to the nearest millimetre using a stadiometer and weight was recorded to the nearest gram using clinical scales. Body mass index (BMI) was calculated by dividing body weight (kg) by the square of body height (m).
Sonographic imaging
Sonographic examination of the Achilles and patellar tendons was undertaken by an experienced operator using a 10 MHz linear array transducer (Echoblaster 128, UAB Telemed, Vilnius, Lithuania) and standardised protocol. The accuracy and precision of the ultrasound system was evaluated by undertaking repeated measurements of a standard calibration phantom (040GSE, CIRS, Norfolk, Virginia, USA), consisting of a number of Nylon monofilaments of varying diameters (0.1–8 mm) and depths embedded within a tissue-mimicking material (attenuation: 0.5±0.05 dB/cm-MHz). The 95% limits of agreement for repeated measures of 27 separate calibration monofilaments were ±100 µm, with a root mean square (RMS) error of 184 µm.
In accordance with recommendations, longitudinal sonograms of each tendon were acquired perpendicular to the point of maximum tendon width to encompass the superior aspect of the calcaneus and distal Achilles tendon and the inferior aspect of the patella and proximal patellar tendon (figure 1).32 Sagittal images of the Achilles tendon were acquired with the participant prone and the ankle passively positioned at 90°,33 while sagittal plane images of the patellar tendon were acquired with the participants supine with their leg passively positioned at right angles (90°) to their thigh.32 Sonographic images were taken immediately prior to and following completion of 90 repetitions of resistance exercise and repeated during recovery at 3, 6, 12 and 24 h postexercise for the Achilles tendon and at 3, 6 and 24 h postexercise for the patellar tendon.

Tendon thickness was measured from sagittal sonograms at standard reference sites and with the aid of a greyscale profile. Achilles tendon thickness was determined 20 mm superior to its calcaneal (C) insertion (a). Patellar tendon thickness was measured 20 mm distal to the inferior pole (P) of the patella (b).
Exercise protocol
Following pre-exercise sonograms, participants randomly completed closed kinetic chain resistance exercises involving the Quadriceps (n=9) or Gastrocnemius (n=8) muscle groups. Quadriceps exercises consisted of 90 repetitions of double-leg squat exercises in which participants moved from standing erect, to a position of 90° of knee flexion and then back again.34 Ankle exercises consisted of 90 repetitions of double-leg calf raises in which participants moved their foot from full ankle plantarflexion to full dorsiflexion and then back again with their knee in an extended position.35 Quadriceps exercises were performed against an effective resistance of 175% body weight and ankle exercises against an effective resistance of 250% body weight, so as to induce tensile loads similar to that experienced during gait.34–36
Data reduction and statistical analysis
Sonographic images were analysed using MATLAB software (MathWorks Inc, Natick, Massachusetts, USA). Patellar tendon thickness was determined at a standard site, 20 mm distal to its attachment at the inferior pole of the patellar,32 while Achilles tendon thickness was determined 20 mm proximal to its calcaneal insertion. The anterior and posterior edges of the tendons were identified with the aid of a grey-scale profile, and manually digitised (figure 1). The stretch ratio (λ), the ratio of postexercise to pre-exercise tendon thickness, was subsequently calculated as a measure of TS. The stretch ratio is commonly used in the analysis of materials that exhibit large deformations and approximates to engineering strain (ɛ) by; ɛ=1−λ. The coefficient of variation for repeated measures of tendon thickness was 2.3% and 2.6% for the Achilles and patellar tendons, respectively.
Although biexponential models have been used to describe the two phase recovery behaviour of collagenous tissues such as intervertebral disc,26 ,28 a single-term exponential recovery function can also be used to successfully model creep recovery in other human soft tissues.37 Hence, the recovery in TS following exercise was modelled for each participant using a single-term exponential function; TS(t) = λo + λe(−βt), where constants λo, λ and β represent the initial stretch ratio, the range and the rate of recovery, respectively, and were estimated using non-linear regression and minimising RMS error. The time for the tendon to return to 63% of pre-exercise dimensions, the so-called primary recovery time, was estimated as the inverse of the β term for each participant.
The Statistical Package for the Social Sciences (SPSS Inc, Chicago, Illinois, USA) was used for all statistical procedures. As outcome variables were determined to be normally distributed, means and SDs have been used as summary statistics. Between-group differences in body anthropometry were investigated using independent t tests. Differences in tendon thickness immediately pre-exercise and postexercise were investigated using paired t tests. Differences in the TS response and recovery time between the Achilles and patellar tendons were investigated using independent t tests. Relationships between variables were investigated using Pearson product–moment correlations. An α level of 0.01 was used.
Results
Anthropometric characteristics of participants are summarised in table 1. There was no statistically significant difference in average age, height or weight of participants performing the two exercise protocols.
Demographic characteristics of participants completing Achilles and patellar tendon exercises
The average thickness of the Achilles and patellar tendons prior to exercise was 4.0±0.4 and 3.2±1.2 mm, respectively. While the Achilles tendon was, on average, 27% thicker than the patellar tendon at baseline, this difference was not statistically significant.
Resistance exercise resulted in a significant and immediate decrease in the sagittal thickness of the Achilles (t7=10.6, p<0.001) and patellar (t8=8.9, p<0.001) tendons of all participants, resulting in an average stretch ratio of 0.86±0.04 and 0.82±0.05, respectively. This difference in TS response between the two tendons was not statistically significant. Similarly, there was no significant correlation between anthropometric measures (height, weight and BMI) and transverse stretch ratio (r=0.22–0.39). However, participant age was moderately correlated with the magnitude of the immediate TS response in the Achilles and patellar tendons (r=0.63, p<0.01), such that older age was characterised by a diminished TS response (figure 2).

Effect of age on the immediate transverse strain of the Achilles (▪) and patellar (°) tendons in response to exercise.
Although tendon dimensions returned to pre-exercise levels for both tendons within 24 h, recovery in TS was exponential in nature (figure 3). The R2 goodness-of-fit for the overall model was 0.99 for both the Achilles and patellar tendons, with the R2 fit for individual TS–recovery curves exceeding 0.93 in all cases. The average primary recovery time was 6.5±3.2 h for the Achilles tendon and 7.1±3.2 h for the patellar tendon and was not significantly different between tendons. Recovery was, however, dependent on body weight (p<0.01), with greater body weight associated with prolonged primary recovery in TS (figure 4). This relationship was also exponential in nature, with body weight accounting for 62% and 64% of the variation in primary recovery time of the patellar and Achilles tendons, respectively.
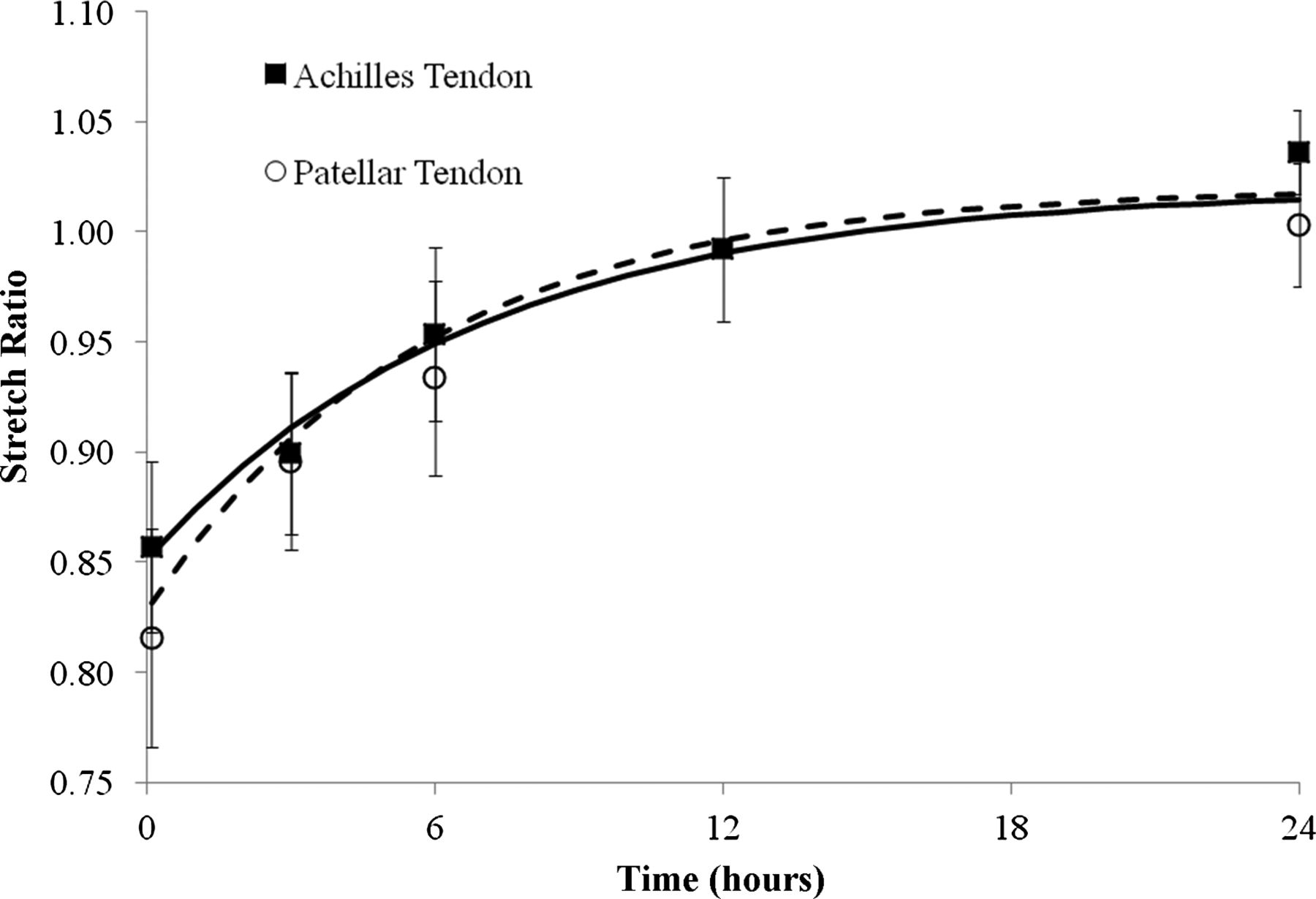
Recovery curves for the acute transverse strain of the Achilles (▪) and patellar (°) tendons following resistance exercise.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between body weight and the primary recovery time of the Achilles (▪) and patellar (°) tendons following resistance exercise.
Discussion
The Achilles and patellar tendons are widely regarded to function as springs, storing and elastically returning strain energy during locomotion, which is thought to improve the efficiency of gait and protect against muscle damage during rapid and forceful lengthening. Although these tendons are exposed to high levels of stress during life and are prone to chronic ‘overuse’ injury,31 little is known regarding their acute response to exercise or the time course of their recovery postexercise. The findings of the current study indicate that resistance exercise results in an immediate but transient decrease (14–18%) in the thickness of the Achilles and patellar tendons, that is, recoverable within 24 h.
Acute reductions in tendon thickness have been previously, though not exclusively,38 ,39 observed following intense or prolonged exercise in vivo.19–24 Hypothesised to largely reflect the movement of fluid associated with load-induced alignment of the solid phase of the tendon matrix, the findings of the current study are consistent with in vitro observations in animal models in which static and cyclic loading have been shown to result in reduced tendon thickness, rapid unbinding and extrusion of intratendinous fluid and visible loss of water and glycosaminoglycans.40–42 These observations are also consistent with axial creep behaviour, manifest as an increase in axial length with cyclic load, reported with mechanical testing of both animal18 ,25–27 and human soft tissues in vitro,27 ,28 and following loading of human tendon, ligament and intervertebral disc in vivo.43–45
Axial creep in tendon has been suggested to alter the potential of muscle to generate force, via both direct mechanical and neuromuscular effects, and thereby increase the risk of injury.46 ,47 Although the mechanisms underpinning the creep response of soft tissues are poorly understood, Vresilovic et al48 proposed that, for the intervertebral disc, the magnitude of dynamic creep was dependent on the quantity of fluid within the fluid-flow pathway, and demonstrated marked changes in creep of the disc with manipulation of tissue hydration. While comparable effects of hydration have been observed on the relaxation behaviour of tendon in vitro,49 in the current study exercise induced a similar magnitude of TS in both the Achilles (1−λ, 0.14) and patellar (1−λ, 0.18) tendons, suggesting that the pathway and unbound fluid content of the two tendons are likely comparable. In support, Maynard et al50 demonstrated that the water content of the rabbit Achilles tendon (59% wet weight) did not differ from that of the patellar tendon (63% wet weight), despite obvious differences in the ultrastructure of the two tendons and subtle differences in cellular properties and responsiveness, collagen crimp, interstitial space and glycosaminoglycan concentration.51–54
A novel finding of the current study was that the magnitude of the TS response of the two tendons following exercise was moderately correlated with age. Older age was associated with a reduced TS response. Based on the regression equation, each decade of life was associated with a ≈2.5% reduction in the TS response of the Achilles and patellar tendons. Changes in the composition of tendon, including increased collagen cross linking, altered fibril morphology, decreased glycosaminoglycan concentration and lower water content are known to occur with aging.55–58 Given that load-induced fluid movement has been hypothesised to play a key role in tendon homeostasis and that tendinopathy is characterised by a reduced TS response to exercise,59 ,60 it is possible that diminished load-induced fluid movement with aging, as evidenced by a lower TS response to exercise, may in part account for the impaired ability of tendon in the elderly to adapt to training and the greater incidence of tendon degeneration and rupture with advancing age.61 ,62 However, age accounted for only 40% of the variation in the TS response of tendon to exercise, suggesting that other, as yet unidentified, factors also influence the transverse creep response of tendon to exercise.
Recovery of TS, as defined by the stretch ratio, in the Achilles and patellar tendons in the current study followed an exponential pattern and was several orders of magnitude longer (hours) than the duration of the exercise (minutes). The average time for primary recovery of the Achilles and patellar tendons following exercise was 6.5±3.2 h and 7.1±3.2 h, respectively. This finding is consistent with in vitro studies on the axial creep of skin and disc tissues,28 ,63 and similarly slow recovery rates, albeit in axial strain, have been reported in vivo for other biological tissues following mechanical loading in animal models. Gedalia et al64 observed that feline lumbar structures recovered by only 37% with rest lasting more than twice the duration of creep loading (2 h). Similarly, Solomonow et al26 observed that 50 min of cyclic load induced axial creep in the feline lumbar spine that required more than 7 h to recover (>90%).
The primary recovery time of the Achilles and patellar tendons in the current study was, in part, dependent on the participant's body weight. Greater mass was associated with a prolonged primary recovery in transverse tendon strain (figure 4). Although delayed physiological recovery in markers of skeletal muscle metabolism and perfusion have been observed following exercise in the obese,65 in vitro studies on the mechanical behaviour of the human vertebral disc have also demonstrated that the creep recovery is influenced by the magnitude and duration of the applied load.28 In the current study, exercises were performed against a percentage of body weight. Consequently, it is unknown if the relationship between body weight and the recovery of transverse strain in the Achilles and patellar tendons reflects physiological processes associated with greater mass or merely greater mechanical loading of the tendon during exercise. Further research, specifically evaluating the creep recovery of tendon to a varied strain stimulus seems warranted.
The present experimental setup did not allow for a mechanistic explanation for the observed recovery in TS following exercise. However, previous in vivo studies in humans have shown that a single bout of loading initiates a cascade of physiological events postexercise, including increased intratendinous blood volume and glucose uptake and the expression of certain genes, growth factors and mediators of inflammation.1 ,5 ,6 ,66 Although markers of collagen metabolism peak after the primary recovery times noted in this study,67 the time course of postexercise circulatory and inflammatory responses appear similar to the recovery in transverse tendon strain. For instance, intratendinous blood volume in the Achilles tendon has been shown to increase immediately following a series of isometric muscle contractions and remain elevated for at least 20 min after exercise.66 Similarly, cyclic loading of ligament and tendon in animal models has been shown to increase the mRNA expression of inflammatory mediators immediately postexercise,68 which return to basal levels in paratendonous tissues within 6–12 h of exercise.69 ,70 It is possible, therefore, that a reactive hyperaemia and/or inflammatory processes may collectively or individually drive imbibition of fluid in tendon and thereby the recovery of tendon dimensions. As such, tendon recovery may reflect active rather than passive processes. However, the time constants for the overall recovery of the patellar and Achilles tendons in the current study (≈6–7 h) are comparable to those reported for recovery of axial strain of the intervertebral disc when studied in vitro (≈8 h),28 suggesting that recovery in transverse tendon strain in vivo may be governed by passive osmotic and ionic forces.
This study evaluated the recovery of transverse tendon strain following resistance exercise protocols that involved periodic concentric and eccentric modes of muscle contraction. While there is some evidence that aerobic exercise may elicit greater tendon hypertrophy than resistance exercise over a 12-week period,62 the time course of tendon recovery observed in the current study may not be transferable to other types and modes of exercise. There is evidence, for instance, that both the mode (eccentric/concentric) and duration of muscle contraction may influence blood flow and the magnitude of creep in tendon.19 ,66 Nonetheless, the findings of the current study demonstrate that short periods of resistance exercise, involving cyclic concentric and eccentric contraction, induce substantial TSs in healthy human Achilles and patellar tendons. While the time course of the recovery of tendon dimensions is considerably longer than the loading duration, with a primary recovery time of around 7 h, the optimal schedule of activity and rest ratios in these high-stress elastic-storage tendons is still unknown, and requires attention in light of the knowledge gained through this study.
Conclusion
In vivo recovery of TS in the Achilles and patellar tendons following resistance exercise of the quadriceps and gastrocnemius muscle groups is considerably longer than the loading duration, with primary recovery in both tendons requiring around 7 h. These findings suggest that, despite their structural differences, the mechanisms underlying Achilles and patellar tendon mechanics in vivo are similar and highly time-dependent. Although further work is required, these findings highlight, for the first time, the duration of recovery required for high-stress tendons to return to pre-exercise dimensions following an acute bout of exercise.
What are the new findings?
-
Despite marked differences in tendon ultrastructure, acute mechanical loading of the Achilles and patellar tendon via resistance exercise results in an immediate though similar decrease in tendon thickness in vivo.
-
Although the acute response to exercise was moderated by age in both tendons, the time course of the recovery of transverse strain (TS) in the Achilles and patellar tendons was considerably longer than the loading duration.
-
Primary recovery requires approximate 7 h for both tendons, but is influenced in part by bodyweight. Complete recovery requires 24 h.
How might it impact clinical practice in the near future?
-
Decreases in tendon thickness following exercise reflect load-induced collagen alignment and convective fluid movement in tendon, which likely plays an important role in tendon homeostasis and adaptation. This is the first study to document the acute TS response and recovery in both the Achilles and patellar tendons following exercise. Despite structural differences between tendons, short periods of resistance exercise induced similar TSs in healthy human Achilles and patellar tendon. These required considerable time to recover. Primary recovery (63%) required about 7 h in healthy tendons, while full recovery required 24 h. While this information could be used clinically to guide physical activity to rest ratios in healthy adults, optimal ratios of activity to rest in high-stress tendons remains unknown, and requires further attention in light of the knowledge gained through this study.
Acknowledgments
The authors would like to thank the research assistant on this study, Dr Nicole Grigg, for her assistance with data collection.
References
Footnotes
-
Contributors SCW is responsible for the overall content of the manuscript as guarantor and made substantial contributions to the project conception and design, data and statistical analysis and interpretation of data; drafting, revision and the final approval of the manuscript. JES contributed to the study conception and design, analysis and interpretation of data, revision and the final approval of the manuscript. SLH contributed to the study design, analysis and interpretation of data, revision and the final approval of the manuscript. SL contributed to the study design, analysis and interpretation of data, revision and the final approval of the manuscript. CP contributed to study conception and design, analysis and interpretation of data, revision and the final approval of the manuscript. JLC contributed to the study conception and design, analysis and interpretation of data, revision and the final approval of the manuscript.
-
Funding This research was funded by an Australian Research Council Linkage Grant (LP_0989716).
-
Competing interests SCW is funded through a Smart Futures Fellowship, Department of Employment, Economic Development and Innovation, Queensland Government.
-
Patient consent Obtained.
-
Ethics approval The study was approved by the regional ethics committee. QUT UHREC (Approval Number: 1000000857).
-
Provenance and peer review Not commissioned; externally peer reviewed.