Article Text

Abstract
Background Low back pain (LBP) is highly prevalent in cricketers, particularly in adolescent fast bowlers. Numerous modifiable risk factors for and interventions to address LBP in cricketers have been proposed in the literature.
Aim Summarise and critique studies evaluating LBP risk factors in cricketers, and evaluate the effectiveness of interventions designed to prevent or treat such LBP.
Study design Systematic literature review.
Methods MEDLINE, ISI Web of Knowledge, CINAHL, SportDiscus and the Cochrane Library were searched from inception using key terms relating to risk factors and interventions in LBP in cricketers. Quality of included studies was assessed using the Downs and Black Quality Index, data were extracted to complete the effect size and OR calculations and evidence levels were established using van Tulder's criteria.
Results 12 studies (6 of high quality) investigating the factors associated with LBP in cricketers and 5 low-quality studies evaluating the interventions for the treatment/prevention of LBP in cricketers were identified. Moderate evidence indicates the presence of acute MRI bone stress as a risk factor for developing lumbar stress fractures. Additionally, moderate evidence indicates increased shoulder counter rotation (associated with mixed bowling actions) and decreased anterior abdominal fascial slide may be associated with LBP in cricketers.
Conclusions Screening for bone stress on MRI should be considered by clinicians managing developing cricketers to identify the risk of lumbar stress fracture development. Numerous associative factors were outlined, although causality needs establishing to further guide interventions in cricketers with LBP. Intervention studies were of insufficient quality to generate concrete conclusions and these research failings require rapid attention.
- Cricket
- Back injuries
Statistics from Altmetric.com
Introduction
Low back pain (LBP) is highly prevalent in cricketers with back and trunk injury prevalence identified as 14% over a 10-year period.1 It is estimated that 4.1% of fast bowlers are likely to be unavailable for selection because of a trunk or back injury at any given time.2 LBP in cricketers also appears to be increasing over time, highlighting the importance of understanding causative factors and most effective treatment and prevention strategies.3
LBP is prevalent in both adults and adolescent cricketers. Alarmingly, one study reported that 22% of adolescent fast bowlers developed a pars interarticularis lumbar 4 (L4) stress lesion over a 4-year period, whereas swimmers at a comparable performance level developed none.4 Additionally, in asymptomatic adolescent fast bowlers, the prevalence of pars interarticularis abnormality and lumbar disc degeneration has been reported to be 33% and 35%, respectively, compared to lumbar spondylosis of 3.5% in the general adolescent population.5 ,6 LBP in adolescence is a significant risk factor for LBP in adulthood, with greater chronicity increasing the risk.7 Therefore, identifying modifiable risk factors and effective interventions is important to both sports and general medicine.
A number of modifiable LBP risk factors in cricketers have been proposed. The most common is the bowling action, with a mixed action proposed to increase LBP risk.8 Specifically, excessive shoulder counter-rotation and hyperextension occurring during the mixed action are thought to increase the stress on the intervertebral disc.8 ,9 Indeed, the ‘crunch factor’ has been defined as the instantaneous product of lateral flexion and axial rotational velocity of the lumbar spine and, although initially described in golfers, it has been suggested that it is implicated in the development of contralateral lumbar spine injuries in fast bowlers.10 Additionally, increased risk of pars interarticularis failure has been attributed to the rapid cycle between flexion and extension.9 Other sports-specific factors proposed to increase LBP risk in cricketers include muscle asymmetry, core stability deficiencies, bowling workload, postural defects and impact forces.3 ,11–14 These proposed mechanisms require further study in order to reliably guide injury prevention measures.
The multifactorial aetiology of LBP in cricketers has led to multiple remedial and preventive interventions being proposed, including avoidance of the mixed bowling action.8 Further, the England Cricket Board (ECB) has produced directives on fast bowling for under 19s and coaches’ safety guidelines,15 ,16 although some literature suggests that more than 12% of young bowlers exceed recommended limits.17 In Australia, a “Bowling Prehab” programme has been developed to encompass technical, physical and workload aspects of preparation, with bowling restrictions for under 16s.18 The growing evidence underpinning these remedial and preventive interventions may offer useful guidance to clinicians, coaches and policy-makers dealing with the increasing incidence of cricket-related LBP.
The aim of this systematic review was to better understand the risk factors associated with LBP development in cricketers, in order to guide and improve injury prevention and treatment strategies, and inform future research in this area. This systematic review will (1) summarise and critique research evaluating risk factors for the development of LBP and (2) evaluate the effectiveness of interventions targeting the treatment and prevention of LBP in cricketers.
Methods
Literature search
ISI Web of Knowledge, MEDLINE, CINAHL, SportsDiscus and the Cochrane Library were searched from inception to 20 November 2012. Separate Medical Subject Heading (MeSH) terms were used for factors theoretically involved in LBP development and interventions for the treatment and prevention of LBP in cricketers (appendix table 1; box 1). The PRISMA statement was followed.19
Inclusion and exclusion criteria
Inclusion/exclusion criteria for studies on factors influencing low back pain (LBP) in cricketers (2A)
-
Inclusion criteria:
-
Cricketers (batsmen/bowlers/wicketkeepers)
-
Any standard of cricket
-
Any age
-
Male or female
-
English language only
-
LBP-relevant outcome measure
-
Intrinsic factors (ie, bowling technique/physiology characteristics) linked to LBP
Exclusion criteria:
-
Extrinsic factors linked to LBP such as occupational workload aside from cricket
-
Studies without an LBP-relevant outcome measure
-
Patents
-
Conference/congress proceedings/letters
-
Magazines
-
Books
-
Government documents
-
Reviews
-
Theses
-
Editorials
Inclusion/exclusion criteria for intervention studies (2B)
-
Inclusion criteria:
-
Cricketers (batsmen/bowlers/wicketkeepers)
-
Any standard of cricket
-
Any age
-
Male or female
-
Intervention studies aimed at treating and/or preventing LBP
-
English language only
Exclusion criteria
-
Patents
-
Conference/congress proceedings
-
Observational studies
-
Magazines
-
Books
-
Government documents
-
Reviews
-
Theses
-
Editorials
Quality assessment
The modified Downs and Black's tool was applied to studies evaluating the possible risk factors/factors associated with LBP in cricketers by SM and SR.20 ,21 The full version of the Downs and Black's tool was used to evaluate the intervention study quality, as most were non-randomised controlled trials.22 Question 27 was modified to “Did the study have sufficient power?” with one point awarded if a significant difference was found or a sample size calculation was completed. Studies evaluating possible risk factors/factors associated with LBP with a score above 10 and interventional studies with a score over 20 were considered high quality.21
Data extraction and analysis
Means and SDs of continuous data were extracted to allow effect size calculations, and ORs were calculated when events in two groups were compared. Review manager was used to calculate and present this in forest plots. Effect sizes were classified as strong (>1.20), medium (0.60–1.19) or weak (<0.60).21 ORs were categorised as very strong (>10), strong (4–10), medium (2.5–3.9) or weak (1.0–2.49).23 A statistical trend was defined if the p value was <0.10 for either effect size or OR calculations. If insufficient data was present in manuscripts, authors were contacted for additional data. Study design, participants’ characteristics and outcome measures were also extracted from the papers.
Definitions for levels of evidence were guided by recommendations made by Tulder et al.24 Specifically, strong evidence was defined as consistent findings among multiple high-quality studies; moderate evidence as consistent findings among multiple low-quality studies, or one high-quality study; limited evidence as findings from one low-quality study and conflicting evidence defined as inconsistent findings among multiple studies.
Results
Results of literature search
A summary of the literature searches is shown in figure 1. Full text articles were excluded that were purely observational, for example, if they examined prevalence rates only or did not distinguish an LBP group or link to LBP. Intervention studies were excluded if they did not evaluate the effect of the intervention on LBP.

Summary of literature search with returns for each search shown using a bracket for each search: factors influencing LBP in cricketers and interventions in cricketers with LBP.
Quality assessment
Appendix table 2 summarises the quality assessment of the articles included. Only five studies evaluating potential risk factors involved in LBP were considered high quality (scoring >10).12 ,25 ,27–29 No high-quality studies evaluating interventions in cricketers with LBP were identified (ie, all scored less than 20), despite one being a randomised controlled trial.34
Methodological characteristics
Appendix table 3 summarises study designs, participants’ characteristics and outcome measures. Mean age of the participants varied from 13.7 to 22.5.29 ,28 Outcome measures varied greatly between studies, and only one intervention study evaluated change in pain.35
Risk factors
Figures 2⇓⇓–5 show the effect size/OR and CI results for risk factors involed in LBP. Data for one study were unavailable despite contacting the corresponding author.33 Burnett et al's25 data are not presented as the sequence of events remains unclear. Owing to study heterogeneity, statistical pooling was deemed inappropriate.
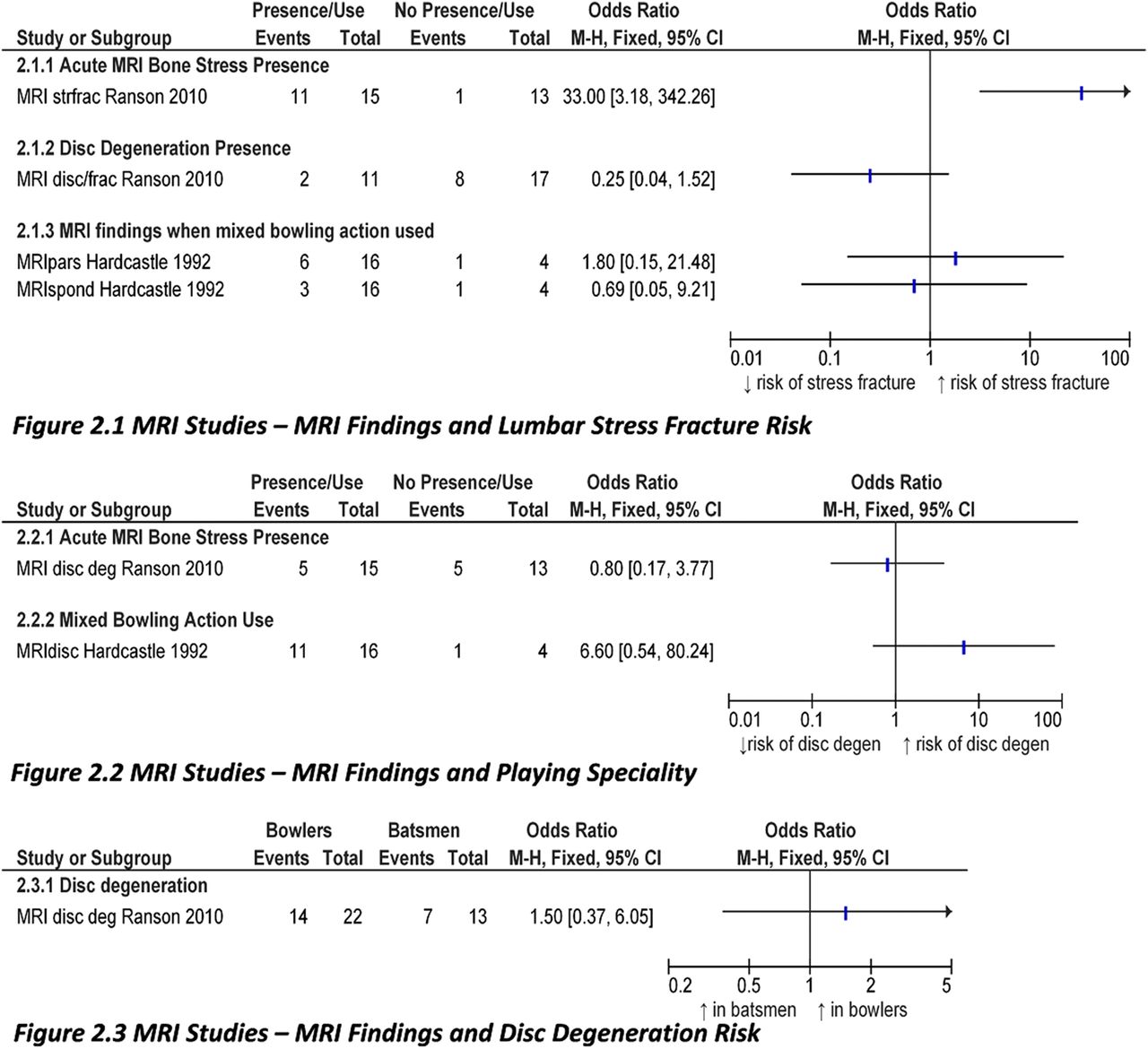
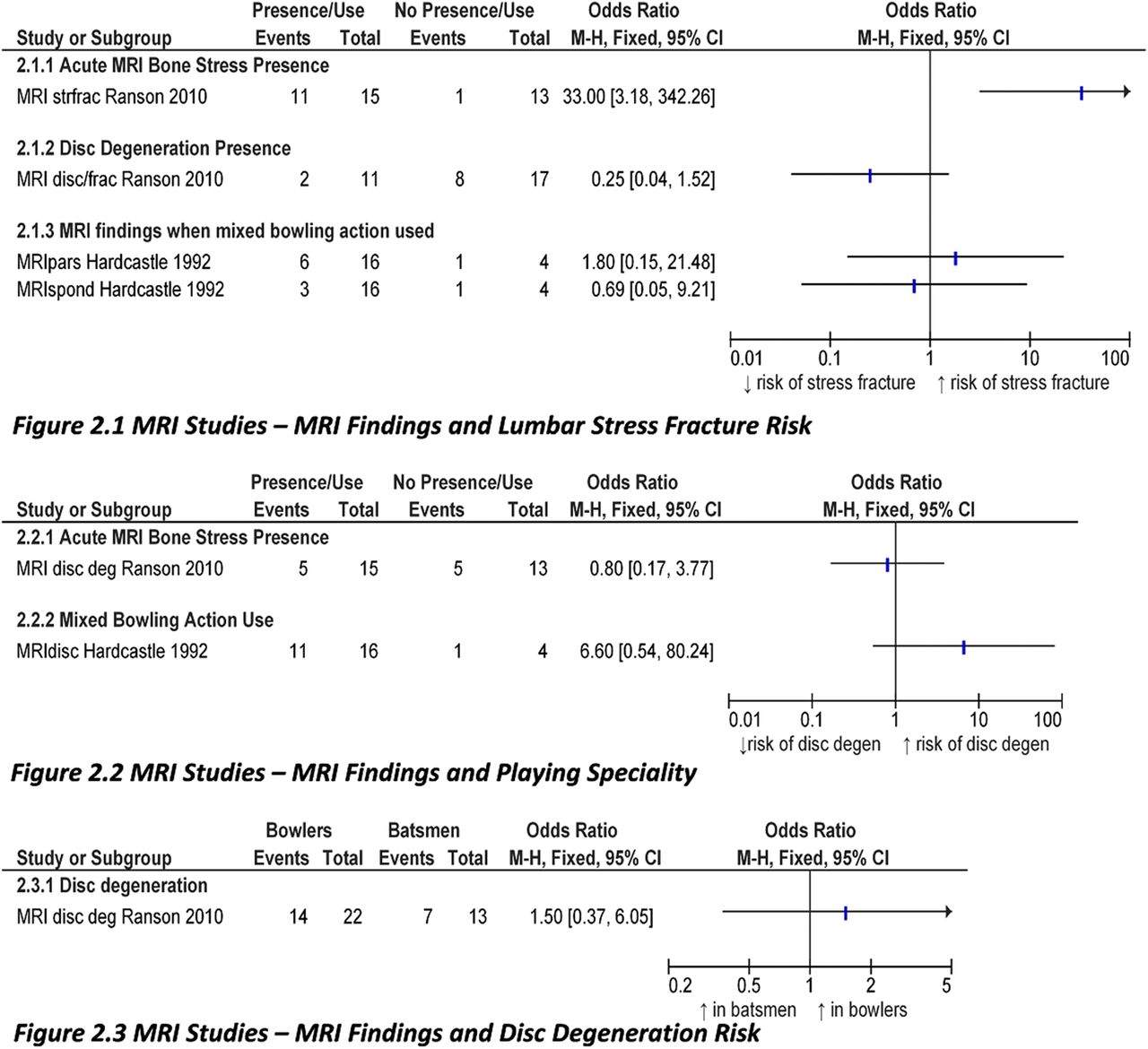
MRI studies analysis—frac, fracture; Strfrac, stress fracture.
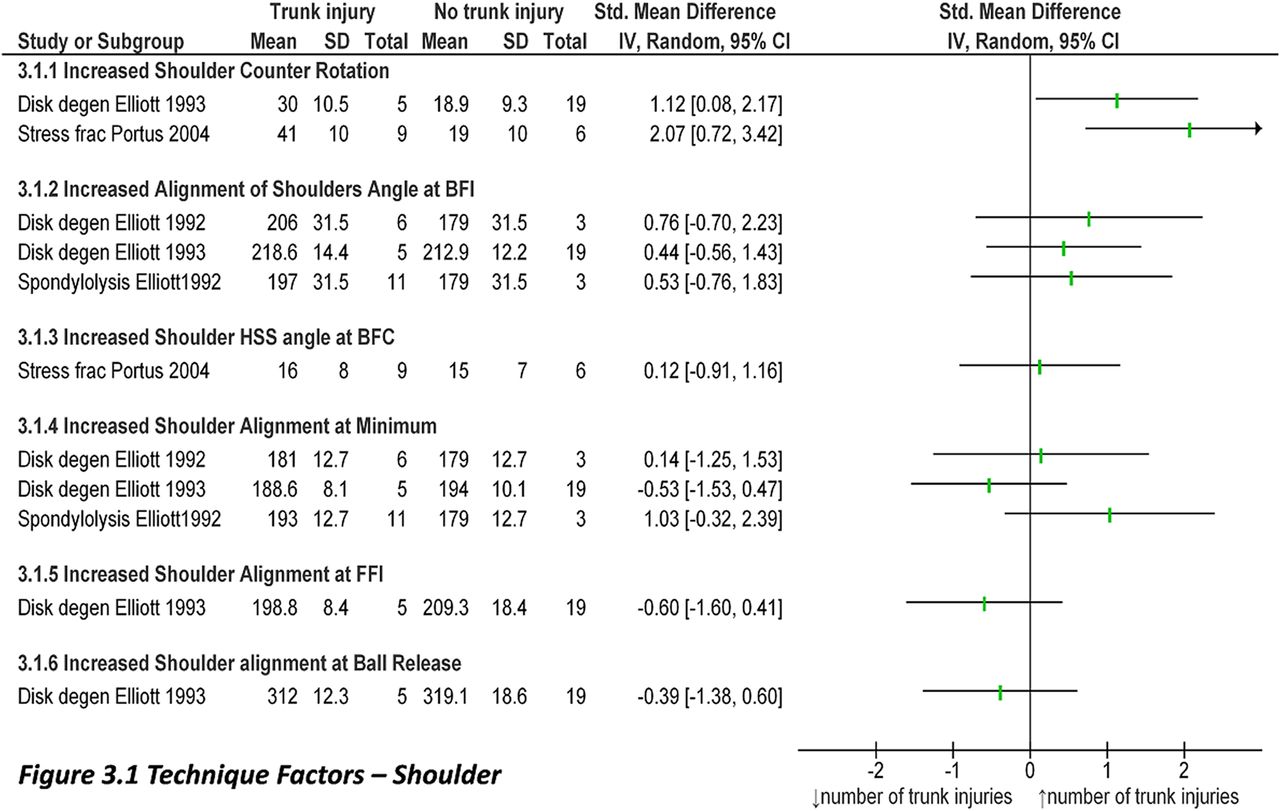
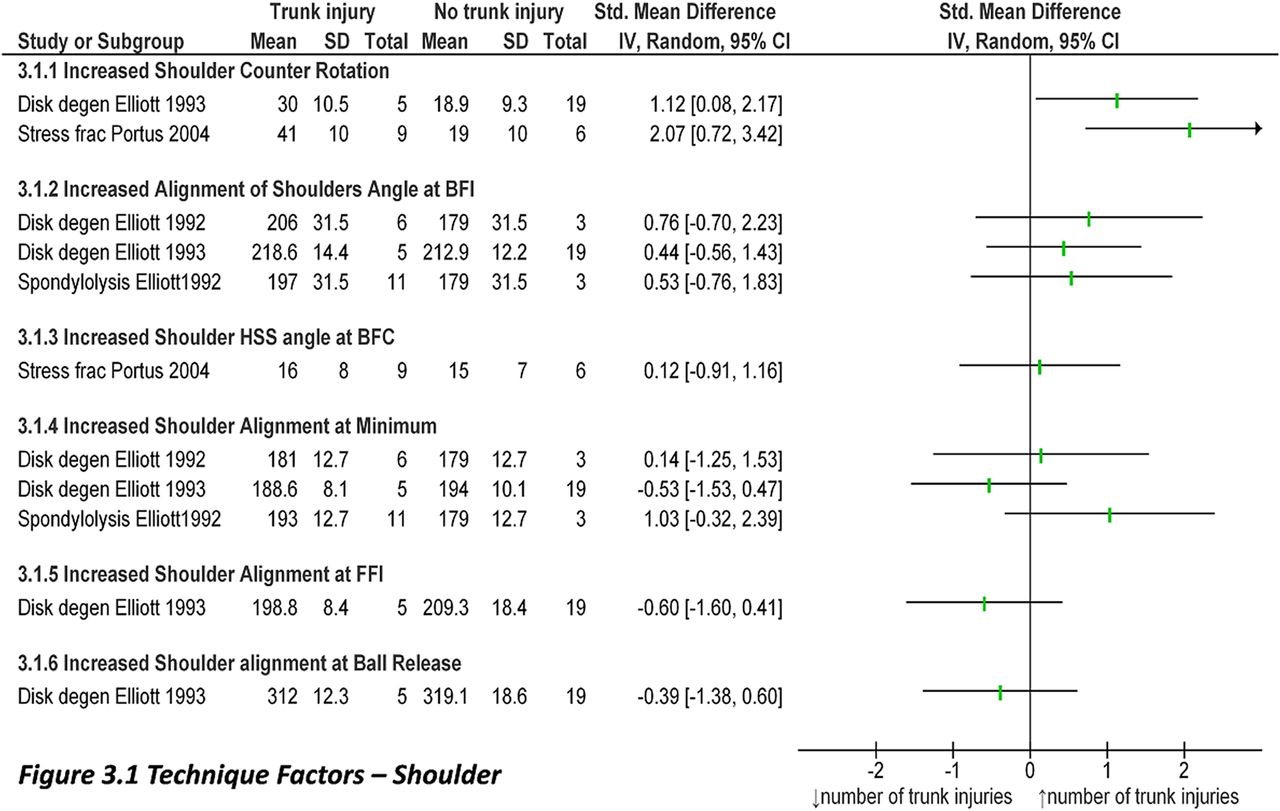
Technique factors analysis—BFC, back foot contact; BFI, back foot impact; Degen, degeneration; ext, extension; FFC, front foot contact; FFI, front foot impact; flex, flexion; frac, fracture; HSS angle, hip shoulder separation angle; LBP, low back pain; lum, lumbar; #, fracture.
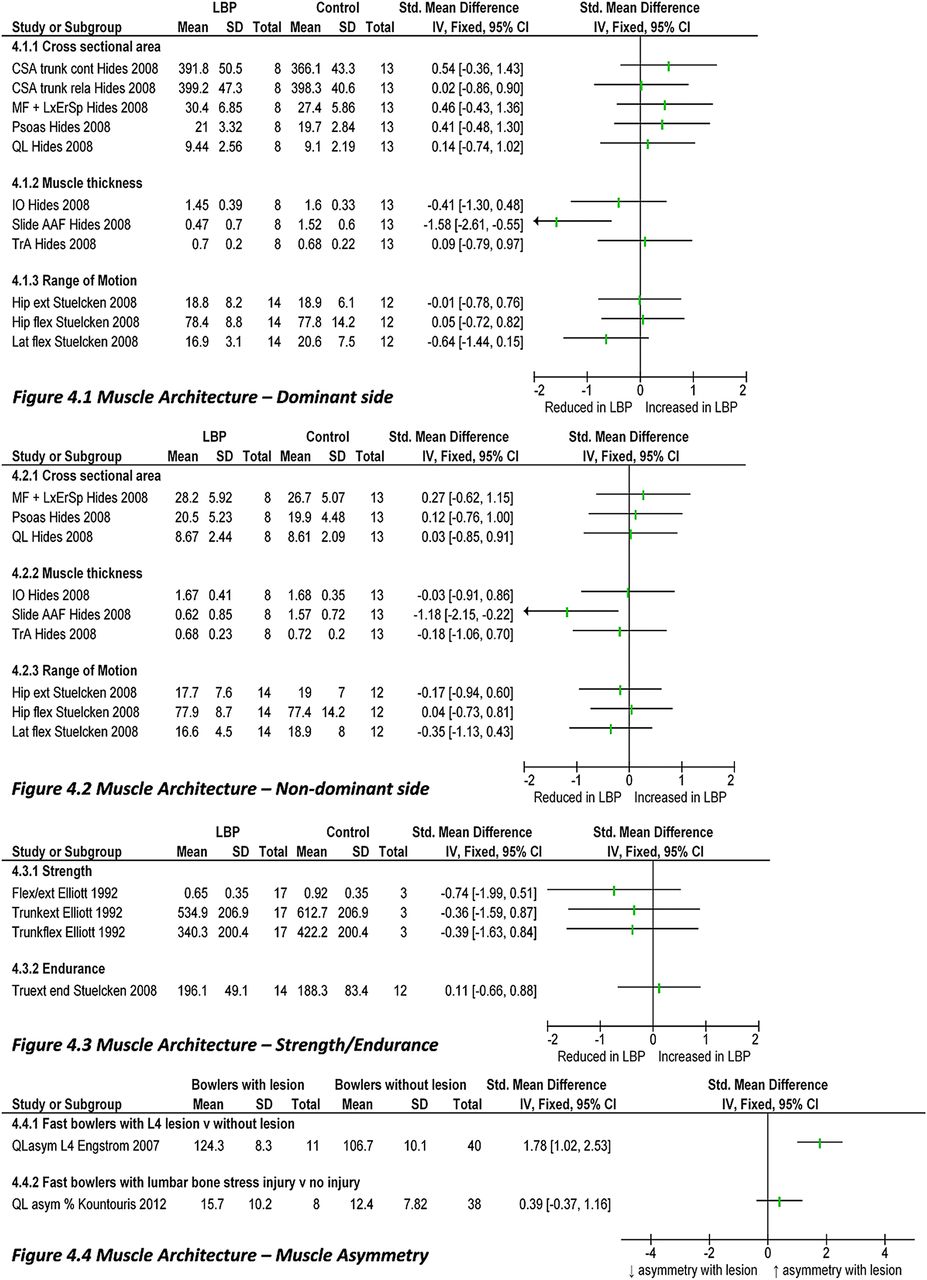
Muscle architecture analysis—AAF, anterior abdominal fascia; CSA, cross-sectional area; IO, internal oblique; Lat, lateral; LxErSp, lumbar erector spinae; MF, multifidus muscle; QL, quadratus lumborum; QL asym, quadratus lumborum asymmetry.

Cricketers’ characteristics analysis.
MRI studies
Moderate evidence suggests a very strong association between acute stress changes on MRI and increased risk of lumbar stress fracture, with an OR of 33 (3.18 to 342.26, figure 2.1.1).27 Limited evidence from one low-quality study indicates that a mixed bowling action is strongly associated with an increased risk of disc deneration (6.60, 0.54 to 80.24, figure 2.2.2).31
Technique factors
Moderate evidence from one high-quality study indicates that increased shoulder counter rotation has a medium association with increased disc degeneration (1.12, 0.08 to 2.17, figure 3.1.1).29 There is limited evidence that increased shoulder counter rotation has a strong association with increased stress fracture prevalence (2.07, 0.72 to 3.42, figure 3.1.1).32
Limited evidence suggests that an increased knee angle at front foot contact (FFC) has a medium association with stress fractures (1.14, 0.00 to 2.28, appendix figure 3.3.1).32 There is also limited evidence that an increased knee angle at ball release has a strong association with both side strains (1.33, 0.08 to 2.58) and stress fractures (1.23, 0.08 to 2.39) (appendix figure 3.3.3).32 There is also limited evidence that a larger minimum knee angle at ball release, that is, relative knee extension, has a strong association with side strains (1.60, 0.29 to 2.92) and a medium association with back sprains (1.14, 0.05 to 2.22, appendix figure 3.3.2).32
Moderate evidence from one high-quality study suggests a strong association between increased stride length to height ratio and disc degeneration (4.83, 3.04 to 6.62, appendix figure 3.7.2).29 There is also moderate evidence of a strong association between increased release height to percentage of height ratio and decreased disc degeneration (−4.83, −6.62 to −3.04, appendix figure 3.8.1).29 Limited evidence suggests a strong association between increased range of lateral flexion of the thorax segment in relation to the pelvis segment during delivery stride and a history of LBP (1.21, 0.36 to 2.06, appendix figure 3.9.9).30
Muscle architecture
Moderate evidence from one high-quality study suggests that increased quadratus lumborum (QL) asymmetry at L4 is associated with the development of an L4 pars lesion, with a strong effect size (1.78, 1.02 to 2.53, figure 4.4.1).12 However moderate evidence also suggests no effect of QL asymmetry percentage on lumbar bone stress injury (0.39, −0.37 to 1.16, figure 4.4.2).26 Additionally, limited evidence suggests that increased lateral slide of the anterior abdominal fascia has a strong association with reduced LBP on the dominant side (−1.58, −2.61 to −0.55, figure 4.1.2) and a medium association on the non-dominant side (−1.18, −2.15 to −0.22, figure 4.2.2).11
Cricketers’ characteristics
Limited evidence suggests increased head displacement from the vertical, measured from a photograph, has a strong association with decreased prevalence of spondylolysis (−1.56, −3.01 to −0.11, appendix figure 5.3.3).13
Coaching interventions/rehabilitation exercises
Appendix figure 6 shows the results of the intervention study with effect size calculations only possible for one low-quality study.35 Despite a reduction in pain visual analogue scale of 20 mm following a 13-week stabilisation programme, the effect size was not statistically significant. The same study also reported decreased asymmetry at L2/3/4/5 of the multifidus muscle cross-sectional area following stabilisation training, although adequate data to complete statistical analysis were not available.35 Additionally, Hides et al36 reported the same stabilisation training increased in the amount of slide of the anterior abdominal fascia in the LBP group.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Coaching interventions in cricketers with low back pain—visual analogue scale pain scores following intervention.
From other intervention studies with inadequate data, Ranson et al37 reported shoulder counter-rotation (p=0.001) could be decreased with coaching over 2 years, while Elliott and Khangure's38 4-year follow-up study reported continuation of a mixed bowling action increased disc degeneration compared to bowlers who successfully changed to a side-on/front-on technique (p=0.002).Wallis et al34 reported that there was no maintained change in technique after training with a harness over 8 weeks, or for coaching.
Discussion
High-quality research evaluating possible risk factors for the development of, and the effectiveness of treatment and prevention interventions for, LBP in cricketers is currently limited. Importantly, no high-quality intervention studies, and only three studies investigating risk factors with a prospective cohort design currently exists.12 ,27 ,26 Despite these limitations, the available research findings synthesised and critiqued in this review can be used to provide guidance to clinicians, coaches and policy-makers dealing with the increasing incidence of cricket-related LBP, and to improve the quality of future research.
Key quality assessment findings and methodological considerations
Six high-quality studies evaluating factors associated with LBP were identified, with four of these possessing elements of a prospective design.12 ,25–27 Therefore, owing to the paucity of high-quality prospective findings at present, there is limited information about risk factors for LBP in cricketers. All five intervention studies were low quality, with only one being a randomised control trial,34 and the remaining studies possessing inadequate control groups.35–38 Therefore, conclusions that could be drawn from currently available research on interventions are somewhat limited.
Sample sizes in all the studies were generally small as might be expected given the difficulty in accessing large cohorts, with most studies containing sample sizes of less than 30—often from only one squad or team—and with no power calculation reported.11 ,13 ,25 ,27–31 35–38 Confounding variables were neither fully described for any studies, nor were they adjusted for (appendix table 2). Only one study considered that the cricketers included played other competitive sports, which is important as other sports are known to be strongly associated with trunk injuries.12 ,39 Little information was provided on LBP history and other injuries. Additionally no intervention studies evaluated potential adverse effects caused by the intervention (eg, other injuries).34–38 This is a vital consideration for coaches and medical staff before choosing to implement any new intervention programme and must be addressed in future research. Control groups were either absent or insufficient for the intervention being investigated. Outcome measures were often described but with no indication of their reliability, somewhat reducing the confidence in conclusions drawn from the data.13 ,25 ,28–33 Nevertheless, significant findings were observed within the studies.
Risk factors for LBP in cricketers
One risk factor identified from prospective data was the presence of acute bone stress on MRI, indicating the potential of MRI as a screening tool. Specifically, 11 of 15 players demonstrating signs of bone stress, classified using the Hollenberg et al40 scale, developed a partial or complete spinal stress fracture within an average of 10 weeks of MRI, and four asymptomatic adolescent fast bowlers with radiological evidence of bone stress at baseline in Kountouris et al's26 recent study all went on to develop a symptomatic bone stress injury during the cricket season. Additionally, conference proceedings published in 2008 by Ranson et al41 showed that 70% of the asymptomatic bowlers who had acute stress changes on MRI went on to suffer an acute lumbar stress injury within one season. These findings should be considered when screening or assessing the meaning of MRI scans in young cricketers and particular attention should be paid to early bone stress signs by responsible clinicians. Importantly, the four players who did not develop a stress fracture in Hollenberg et al's40 study only bowled two to four more weeks and then had a 6–12 weeks rest period, suggesting time off may be an effective preventive strategy.
There is conflicting evidence shown in figure 4.4 on the effect increased QL asymmetry has on the development of lumbar bone stress injuries. Engstrom et al12 showed that QL asymmetry was associated with an L4 lesion whereas Kountouris et al26 did not. It may be that the different criteria resulted in the differences noted, as Engstrom included results over four seasons compared to Kountouris including results after only one season.12 ,26 However, conference proceedings by Ranson et al41 also showed no link between QL asymmetry and lumbar spine injury. Interestingly, a recent observational study by Crewe et al examining both biomechanics and QL asymmsetry suggests that those bowlers who experience large lumbopelvic lateral flexion loads during bowling may develop greater QL asymmetry. This position is also associated with an increased risk of lumbar spondylolysis and therefore identifying asymmetry on MRI may be a warning of an increased risk of injury rather than a risk factor itself.42 Further research is needed in this area.
Increased shoulder counter rotation appears to be associated with both disc degeneration and stress fracture development, known to be associated with a mixed bowling action.8 In addition, Burnett et al's25 study indicated an OR of 16 for greater disc degeneration prevalence when a mixed bowling action continued over a period of 3 years. Theoretically, large shoulder counter-rotation, along with increased range of lateral flexion of the thorax in relation to the pelvis during the delivery stride is likely to increase spinal stress,43 leading to disc herniation and/or pars interarticularis failure.8 Consideration of shoulder counter rotation as a covariate in prospective analyses of risk factors for LBP would be useful.
Increased stride length to height ratio, and relative knee extension at ball release were found to be present in cricketers with trunk injuries. It is suggested that both factors may impair the dissipation of impact forces.33 Specifically, if the knee is more flexed there will also be a decreased release height which is seen in non-injured bowlers; it may well be that by bending the knee more at ball release, the ground reaction forces are dissipated better through the body resulting in less impact through the spine.33 Considering this, coaching bowlers to reduce stride length during their run up and increasing knee flexion at ball release may provide potential treatment and prevention strategies for LBP in cricketers. Further research to evaluate this possibility is needed. Posture also requires further study, given the strong association seen between increased head displacement from vertical and the decreased prevalence of spondylolysis. These factors could be studied further using simple video analysis in coaching and or sports medicine consultations.
Limited evidence suggests a strong association between reduced lateral slide of the anterior abdominal fascia and LBP.11 Anterior abdominal slide occurs during concentric contraction of the transversus abdominis muscle bilaterally in a ‘drawing-in’ action of the abdominal wall in normal pain-free elite cricketers.44 Therefore, reduced lateral anterior abdominal slide seen in cricketers with LBP may reflect an inability to draw in the transversus abdominis muscle appropriately, which is known to be related to lumbopelvic pain.44 Importantly, improved ability to ‘draw-in’ the transversus abdominis muscle and increase anterior abdominal slide has been reported to reduce and maintain reduction of LBP in the general population.45
Consistent with studies on the general adolescent population,46 findings from Elliot et al13 suggest that as age increases the prevalence of spondylolysis and disc degeneration also increases in adolescent cricketers. However, it seems that cricketers are starting at a higher prevalence level than other sportsmen at comparable performance levels. For example, when compared to adolescent swimmers, young fast bowlers show an increased prevalence, indicating skills required in the game (eg, bowling) may accelerate the normal aging process of disc degeneration.4–6 Future research could therefore address whether this process is accelerated and whether the increased prevalence seen in adolescence continues for an adult cricketing population.
Interventions for LBP in cricketers
As noted above, reduced anterior abdominal fascia lateral slide is associated with LBP.11 ,12 Two studies investigated a 13-week abdominal stabilisation training programme to improve anterior abdominal fascia slide and decrease asymmetry of the multifidus muscles.35 ,36 Unfortunately, it is difficult to draw conclusions from these studies as they included both very low participant numbers (6–7) and no control groups. However, graphically there is some indication from effect size calculations that LBP may be reduced as a result of the programme (appendix figure 6.1).35 Additionally, the stabilisation programme was also found to increase in anterior abdominal fascia slide, a factor found to be reduced in cricketers with LBP.11 ,35 ,36 Importantly, similar programmes in high-risk sporting populations, such as golf and gymnastics, have indicated improvements in LBP.39 ,47 ,48 For example, a study in 51 top level young gymnasts (age 11–16) reported a 12-week training programme based on specific segmental muscles of the lumbar spine reduced the number of days on which LBP was reported.48 These findings encourage larger randomised controlled trials following CONSORT guidelines to evaluate the effectiveness of stabilisation training in cricketers with LBP to enable clear clinical recommendations to be made.49 It must also be considered that results from these stabilisation studies may be confounded by cointervention.11 ,12 Specifically, the stabilisation training programme involved the removal of weights training for 6 weeks and then gradual reintroduction for 7 weeks. It may be that a lack of weights training decreased LBP rather than the stabilisation programme, a factor that should be considered in the design of any follow-up study.36
Three intervention studies evaluated forms of coaching to encourage bowlers not to use the mixed bowling action and move towards a safer bowling action, such as a more side-on technique, to prevent LBP developing.34 ,37 ,38 Findings indicate limited evidence that shoulder counter rotation can be decreased by coaching, and that a ‘safe’ action results in reduced lumbar disc degeneration.38 Considering the link between increased shoulder counter rotation and LBP in cricketers, these findings indicate that retraining programmes may be effective in the treatment or prevention of LBP. Further research is needed to establish if such changes can prevent or effectively treat LBP. Importantly, studies involving coaching over a 2-year to 3-year period showed a reduction in the use of a mixed bowling action;37 ,38 however, the study that provided 8 weeks of coaching did not.34 This highlights that effective retraining may take a long period of time, although the optimal time period still needs to be established. Additionally, moderate evidence also indicates that the use of a bowling harness may not assist bowling action changes.34
Clinical implications and key areas for future research
Current interventions evaluated, including core strengthening and bowling retraining, appear promising and should be considered in clinical practice as a means to both prevent and treat LBP. However, further evaluation is needed before their importance in the development of injury prevention and treatment programmes for cricketers with LBP can be established. Additionally, the review suggests that relative knee extension at FFC during bowling is associated with an increased prevalence of trunk injuries, suggesting that increasing knee flexion during the bowling action could prevent trunk injuries. Interestingly, however, in Ranson et al's37 study, players were coached towards less back and front foot knee flexion, possibly because of the suggestion that a straight front leg will increase ball speed owing to more efficient transfer of kinetic energy.32 ,50 Therefore, in this case, injury risk may be over-ruled by performance. Further research to identify if relative knee extension is a true risk factor for LBP development is needed to improve coaching guidelines.
The potential for MRI as a screening tool to prevent the occurrence, or worsening, of LBP, and specifically highly debilitating stress fractures is highlighted.5 Importantly, a scan in the middle of season and appropriate response (eg, rest) may prevent months of lost playing time. This may be especially important in international cricketers as the ‘off-season’ grows ever shorter with autumn, winter and spring tours. However, the expensive nature of completing MRI scans must be considered, particularly for amateur cricketers. In fact, the high cost of completing an MRI scan highlights the need to identify more clinically applicable risk factor screening tests in future research.
Another area requiring strong consideration in future research is the age which cricketers should begin to receive intervention for treatment or prevention of LBP, especially considering the high prevalence of lumbar spine injuries in adolescence.4 ,34–38 Additionally, directives and guidelines currently in place, such as “Bowling Prehab”, ECB coaches’ safety pack and ECB under 19 guidelines, require scientific validation, especially, as they appear to be often ignored.15–18
Conclusion
Acute bone stress on MRI scans was the main risk factor identified for LBP in cricketers, specifically associated with an increased prevalence of lumbar stress fractures. This highlights the potential benefit of MRI as a screening tool, although cost must be considered. Additionally, the most effective prevention programmes for individuals with acute bone stress require further evaluation, although reduced workload/rest may be effective. Although moderate evidence indicates increased shoulder counter rotation, and its relationship with a mixed bowling action is associated with increased prevalence of LBP, prospective research is needed to establish conclusively whether this is a true risk factor. Evaluating the link of bowling action and other proposed risk factors with LBP development in cricketers is needed to understand more about causality and identify more inexpensive screening tools.
Limited evidence indicates that reduced anterior abdominal fascia slide may be associated with LBP. Additionally, one low-quality study indicates that pain may be reduced, and anterior abdominal fascia slide increased following a stabilisation programme, indicating that such a programme may be considered in a clinical setting. However, larger high-quality randomised controlled trials to follow-up are required before clear conclusions can be made. Currently available low-quality coaching intervention studies suggest that bowling technical changes can be made over a long period of time (2–3 years). However, associated reductions in pain or improvements to function are yet to be evaluated, indicating the need for higher quality randomised controlled trials in this area.
This review has yielded real insight concerning LBP in cricket. Common methodological faults and the retrospective nature of most current research raise questions regarding concerted action at a cricketing management level to answer. Considering the high risk of LBP and potential long-term ramifications in young cricketers, national and world cricketing bodies should consider commissioning and resourcing significant high-quality prospective research to answer the many questions raised in this review. There is clearly the potential for a step change in the understanding, prevention and management of a major sports-specific problem of significant importance to both sports and general medicine.
What are the new findings?
-
There are a limited number of high-quality studies investigating both factors associated with low back pain in cricketers and studies evaluating interventions for the treatment/prevention of low back pain in cricketers.
-
Screening for bone stress on MRI should be considered to identify lumbar stress fracture development.
-
Numerous associative factors have been outlined for low back pain in cricketers, but further research is required to establish causality.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors SM, CJB and DM contributed to formulation of the idea. SM and CJB acquired the data and did initial analysis which SR and DM then contributed to SM, in particular, but all authors contributed to drafting and revision of the final paper, and approved the final version. DM gave final approval for the version to be submitted.
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.