Article Text

Abstract
Background/aim The international governing body for competitive rowing recently mandated the inclusion of 12-lead ECG during preparticipation screening. We therefore sought to describe normative ECG characteristics and to examine the prevalence of abnormal ECG findings as defined by contemporary athlete ECG interpretation criteria among competitive rowers.
Methods Competitive rowers (n=330, 56% male) underwent standard 12-lead ECG at the time of collegiate preparticipation screening. ECGs were analysed quantitatively to develop a sport-specific normative database and then for the presence of abnormalities in accordance with the 2010 European Society of Cardiology (ESC) recommendations and 2013 ‘Seattle Criteria.’
Results 94% of rowers had one or more training-related ECG patterns including sinus bradycardia (51%), sinus arrhythmia (55%), and incomplete right bundle branch block (42%). Males were more likely than females to have isolated voltage criteria for left ventricular hypertrophy (LVH) (51% vs 8%, p<0.001) and early repolarisation pattern (76% vs 23%, p<0.001). Application of the 2010 ESC criteria, compared to the Seattle criteria, resulted in the classification of a significantly greater number of abnormal ECGs (47% vs 4%; p<0.001). The detection of true pathology, accomplished by both interpretation criteria, was confined to a single case of ventricular pre-excitation.
Conclusions Training-related ECG patterns with several gender-based differences are common among competitive rowers. The diagnostic accuracy and down-stream clinical implications of ECG-inclusive preparticipation screening among rowers will be dictated by the choice and future refinement of ECG interpretation criteria.
- Rowing
- Cardiology physiology
Statistics from Altmetric.com
Introduction
Occult cardiovascular disease is the leading cause of sudden death among competitive athletes.1 ,2 The majority of cardiovascular disorders responsible for sudden death during sport may be identified by abnormal findings on the 12-lead ECG.3 ,4 ECG is therefore commonly employed during the diagnostic evaluation of symptomatic athletes and is increasingly used during preparticipation screening. Fédération Internationale des Sociétés d'Aviron (FISA), the international governing body for competitive rowing, recently mandated ECG-inclusive preparticipation screening prior to international regattas.5
The heart adapts to repeated bouts of intense exercise. Exercise-induced cardiac remodelling including changes in chamber size,6 ,7 wall thickness6 ,7 and function8 ,9 have been documented in competitive rowers. Several large cross-sectional studies have described corollary ECG findings in trained athletes,10–13 and have led to the concept of ‘training-related ECG patterns.’ However, rowers constitute a minority of the athletes represented in these studies and have only been specifically examined in small cohorts.14–16 As such, there are relatively limited data defining the sport-specific spectrum of ECG findings among competitive rowers.
We therefore performed a comprehensive analysis of ECG findings in a sizable cohort of competitive rowers with two distinct yet complementary goals. First, we sought to develop a normative database of ECG patterns in this population. Second, we aimed to examine the prevalence of abnormal ECG findings as defined by contemporary criteria that have been developed for ECG interpretation in athletes.17 ,18
Methods
Study design
We utilised a cross-sectional and longitudinal study design to examine the ECG characteristics and clinical follow-up of collegiate rowers at Harvard University. The Harvard University crew is a competitive programme that routinely attracts international calibre man and woman rowers from across the world. Participants were enrolled over consecutive years (2006–2013) during preparticipation screening sessions conducted within the Harvard Athlete Initiative (HAI). The HAI is a research collaboration designed to facilitate the study of cardiovascular health and physiology in student athletes. Participants consisted of newly matriculated male and female rowers ≥18 years of age. Demographic information including age, self-reported ethnicity, country of origin, preseason training volume, height and body mass were obtained for each participant. Next, each rower underwent standardised, non-investigational screening medical history and physical examination based on current American College of Cardiology and American Heart Association recommendations,19 and were administered a 12-lead ECG as previously reported.20 ECG was performed using standard 12-lead placement and equipment (MAC 5500; GE Healthcare, Milwaukee, Wisconsin, USA) following >5 min of supine rest. Written informed consent was obtained from participants before enrolment.
Quantitative ECG analysis
ECGs were interpreted by two independent reviewers, both cardiologists, blinded to all participant characteristics. Ambiguous cases were adjudicated by consensus by the two reviewers. Quantitative measurements including heart rate, PR interval, QT interval, corrected QT interval calculated by the Bazett formula, QRS duration, R wave axis, P wave axis and T wave axis were calculated automatically and confirmed by visual inspection. QRS wave amplitudes and the magnitude of early repolarisation (ERP) were measured manually using calipres. Voltage criteria for left ventricle hypertrophy (LVH) was quantified as a dichotomous variable using both the Sokolow Lyon criteria (S in V1+R in V5 or V6 ≥35 mm)21 and the Cornell criteria (S in V3+R in aVL ≥28 mm for men, and S in V3+R in aVL ≥20 mm for women).22 ERP within a single lead was defined as elevation of the J point of at least 0.1 mV. The presence of ERP was assessed in each of the 12 individual ECG leads and then by territory as follows: anterior (V1 to V4), inferior (II, III, aVF), lateral (V5 to V6, I, aVL)). ERP was considered present in a territory if ≥2 leads in a specific territory met criteria for ERP. The QRS transition zone was defined as the precordial lead at which the QRS complex changes from predominately negative to positive (R/S ratio becomes >1).
Classification of abnormal ECGs
Participant ECGs were then evaluated for the presence of ‘abnormal’ patterns as defined by the 2010 European Society of Cardiology (ESC) criteria and 2013 ‘Seattle criteria’ (tables 3 and 4).17 ,18 Both of these criteria differentiate ECG changes into two groups: benign ‘training–related’ changes and ‘abnormal’ patterns suggestive of underlying pathology.
Clinical and longitudinal follow up
ECG abnormalities requiring clinical follow-up were referred for comprehensive non-investigational testing as appropriate. This follow-up was designed to definitively confirm or exclude pathology as individualised based on specific ECG findings. All participants cleared for rowing participation were followed prospectively for the occurrence of adverse cardiac events from the time of enrolment through college graduation. Thus, our follow-up period captured each individual's participation in organised intercollegiate rowing, the critical time period during which sport-related adverse outcomes would be most likely to occur. Because enrolment occurred over eight consecutive years, follow-up duration was variable. No participants were lost to clinical follow-up.
Statistical analysis
Continuous variables are presented as mean±SD. The significance of differences between genders and ECG interpretation criteria were assessed using two-tailed unpaired t test for normally distributed continuous data, and Fischer's exact test for dichotomous variables. A two-tailed p<0.05 was defined as statistically significant throughout. SPSS V.21.0 (IBM Corp.) and Prism 6.0 (GraphPad Software Inc.) were used for graphic representation and data analyses, respectively.
Results
Study population
Characteristics of the study cohort are shown in table 1. The study group was comprised of 330 rowers (56% male, 18.9±0.8 years old). The majority of participants were Caucasian (91%) and only a small minority were of Afro-Caribbean descent (2%). Seventy-seven per cent of participants came from the USA. Among the 23% of participants who came from outside of the USA, the majority hailed from the UK (25%), Canada (20%) or Australia (15%).
Participant characteristics
Standard ECG measurements
Group mean values and SDs for each conventional ECG measurement are shown in table 2. Males had a more vertical QRS axis than females (74±23 vs 67±21°, p<0.001). Similarly, males had a significantly longer QRS duration than females (p<0.001), with 9% of males and less then 1% of females demonstrating QRS duration of greater than 110 ms (figure 1). No participants demonstrated a QRS duration in excess of 130 ms. Males had greater precordial QRS voltages than females with average summed voltage in lead V1 and lead V5 of 34 mm for males and 25 mm for females (p<0.001). Females had a significantly longer corrected QT interval (QTc) than males (416±21 vs 408 ±19 ms, p<0.001; figure 2). No rowers had a QTc that was less than 360 ms or that exceeded 500 ms.
Quantitative ECG measurements
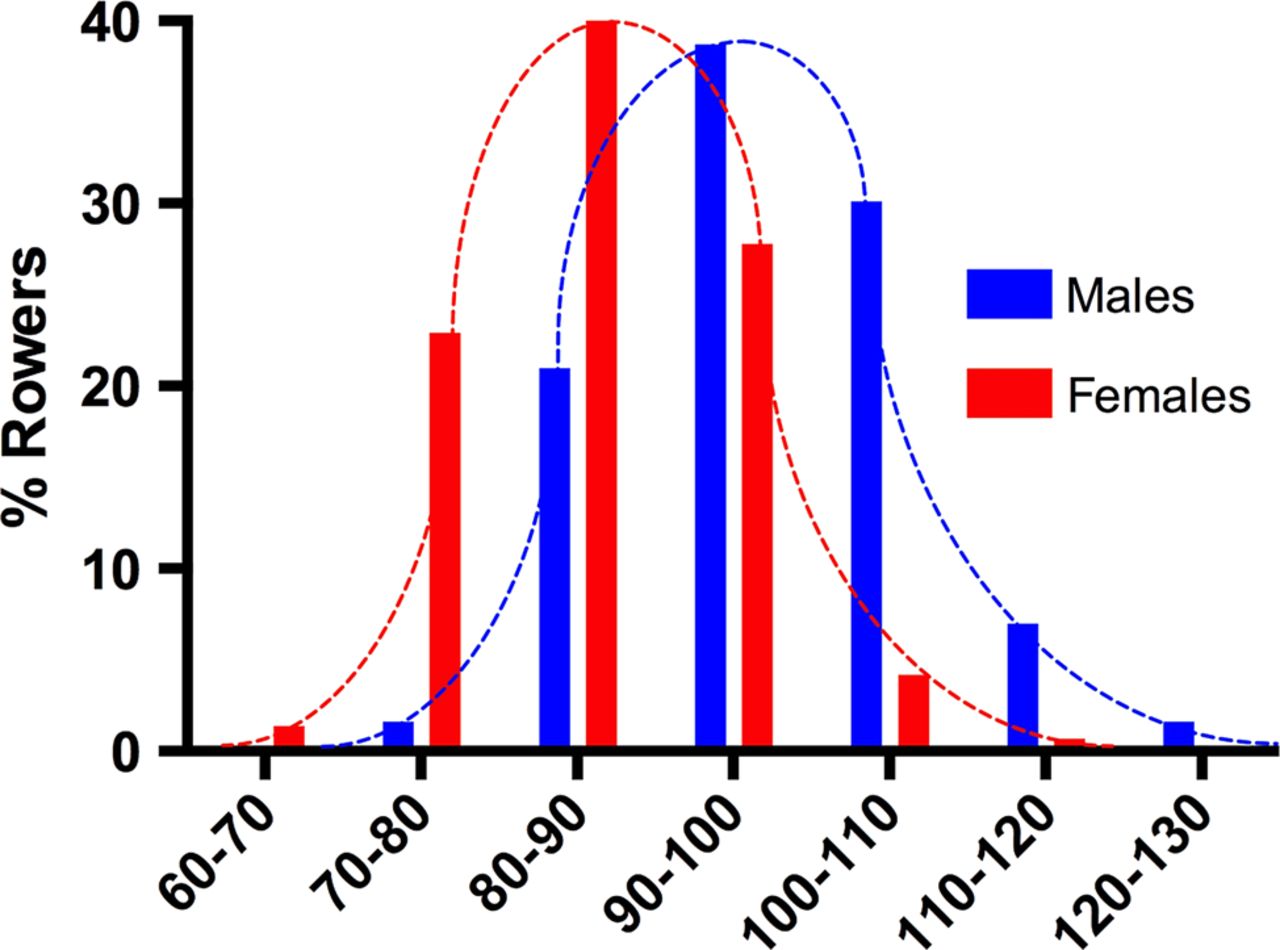
Distribution of QRS duration as a function of gender. Men had a wider QRS than did women. No women had a QRS duration greater than 120 ms, and no men had a QRS duration greater than 130 ms.

Distribution of corrected QT interval (QTc) as a function of gender. Men had a shorter corrected QT (QTc) interval than did women. Short QTc intervals were more common using the recommended ESC criteria limit (n=23) than the Seattle criteria limit of 320 ms, which classified no QTc intervals as short. Long QTc intervals were also more common using the ESC limits (n=12) versus the Seattle limits (n=1). Under the ESC criteria, more males had either a short or long QTc than did females (p=0.03).
Training-related ECG findings
The prevalence of ‘training-related’ changes as defined by the 2010 ESC and/or the 2013 Seattle criteria are shown in table 3. The vast majority of rowers had at least one training-related change on their ECG (n=310/330, 94%) with 74% (n=244/330) demonstrating two or more such changes. Males and females were equally likely to have at least one training-related ECG finding, but males were more likely than females to have two or more of these findings (85% vs 59%, p<0.001).
Prevalence of ‘training-related’ ECG findings
Sinus bradycardia and sinus arrhythmia were present in over half of participants (51% and 55% respectively). Incomplete right bundle branch block (RBBB) without TW inversions (TWI) past lead V2 was found in 42% of rowers, and males and females were equally likely to have this pattern. LVH as defined by voltage criteria occurred in 28% of participants using the Sokolow-Lyon and 14% using the Cornell criteria and was more common among men than women using either scoring system. ERP was present on 53% (n=174/ 330) of rower ECGs (table 3) and was more prevalent among males (76%) than females (23%, p<0.001). The overall increased ERP prevalence among males was driven by a higher prevalence of anterior lead ERP in isolation and in combination with lateral or inferior lead ERP (figure 3). The prevalence of lateral and/or inferior ERP in the absence of anterior ERP was similar among both males and females (5%).

Prevalence and lead distribution territory of early repolarisation (ERP). ERP was more common among males due to a higher prevalence of anterior ERP (males vs females: anterior: 48% vs 10%, p<0.001; anterior+lateral: 13% vs 3%, p=0.001; anterior+inferior: 5% vs 0%, p=0.006). Isolated lateral and/or inferior ERP was occurred with similar frequency (∼5%) in both genders.
Abnormal ECG findings
Application of the 2010 ESC criteria lead to an abnormal ECG classification rate of 47% (n=154/330) while application of the Seattle criteria lead to an abnormal classification rate of 4% (12/330, p<0.001; table 4). These markedly different rates of abnormal ECGs were explained by several key discrepancies regarding trait definition between the two sets of criteria. Specifically, abnormal TWI, largely accounted for by isolated TWI in both leads V1 and V2, was the most frequent reason for an abnormal classification based on the 2010 ESC criteria (58%, n=89/154, figure 4). Rowers with precordial TWI past lead V1 were more likely to have a later transition zone (ie, after lead V4) than rowers without precordial TWI (27% vs 16%, p=0.02). There were no significant differences in athlete demographics (age, height, weight and race) between those with TWI and those without TWI. The relatively higher frequency of abnormal ECG classification based on the 2010 ESC criteria were also accounted for by higher prevalences of QTc intervals outside the normal range (23%, n=35/154) and LAE (24%, n=37/154). Men and woman were equally likely to have an abnormal ECG under the ESC and Seattle criteria.
Prevalence of Abnormal ECG Findings
{kind=link}
{kind=link}
{kind=link}
{kind=link}
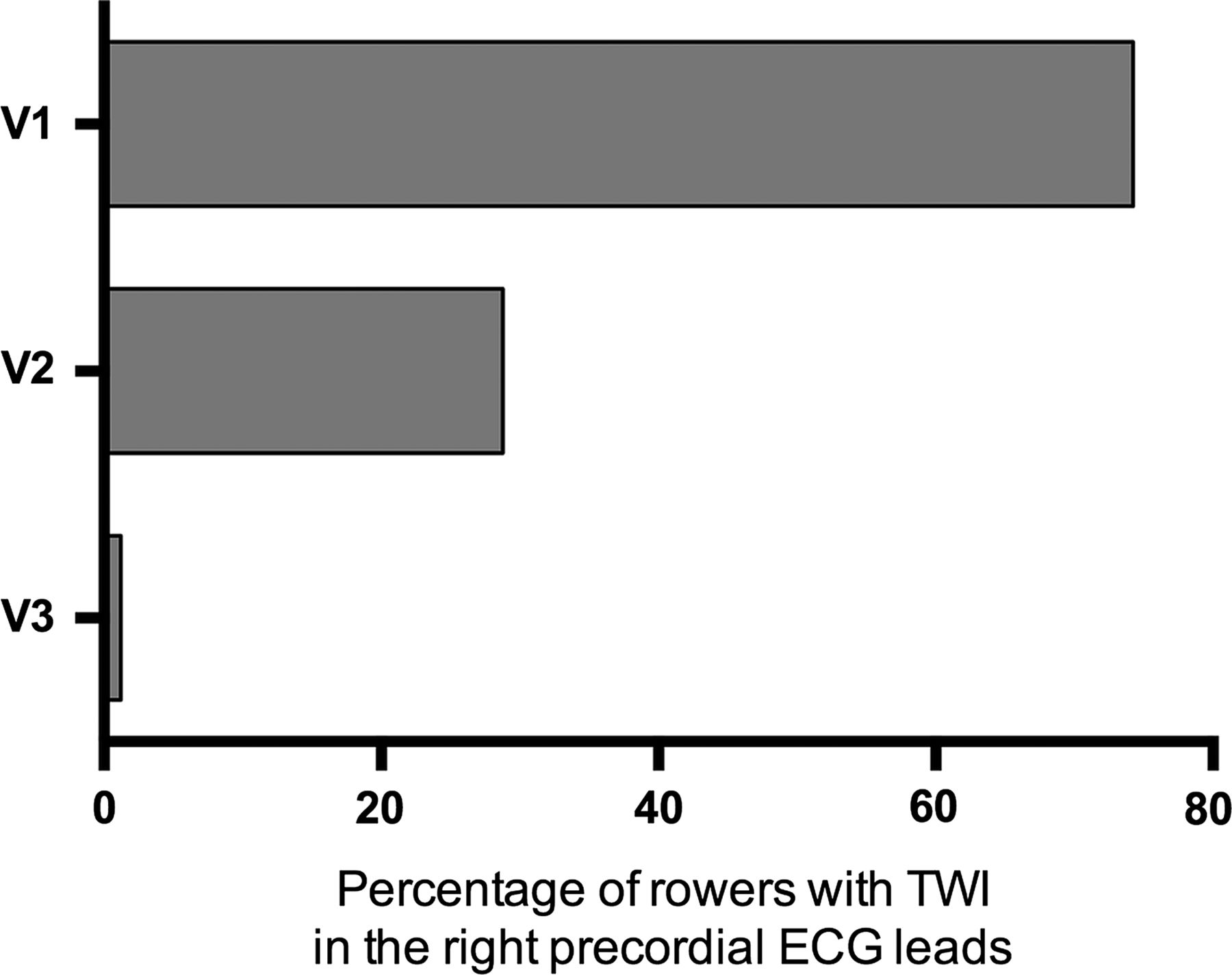
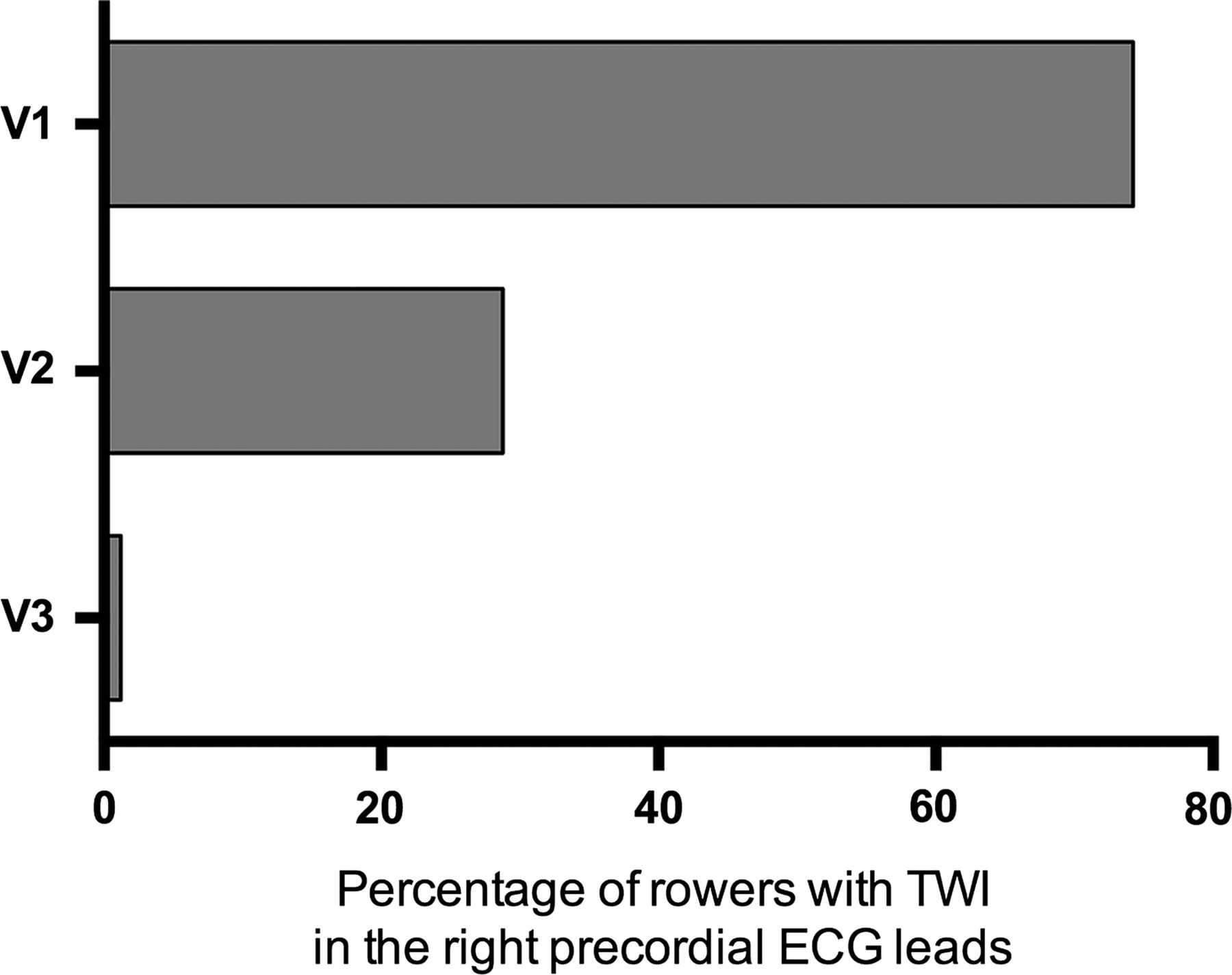
Prevalence of right precordial T-Wave inversions. Precordial T wave inversions (TWI) of ≥2 mm in depth were present in 74% of participants in lead V1, 28% in lead V2, and 1% in lead V3.
Clinical and longitudinal follow-up
No participants were found to have structural heart disease following non-investigational postscreening clinical evaluation. One female rower with a prolonged QTc interval demonstrated normalisation on serial repeat ECGs and physiological QT interval shortening during graded exercise testing. One male rower with a short PR interval was found to have pre-excitation (presence of a delta wave with concomitant QRS prolongation), which resolved abruptly at a submaximal heart rate during graded exercise testing. Thus, no participants were restricted from sport participation. Therefore, all rowers with an abnormal ECG under either set of criteria, with the exception of the participant with pre-excitation who was conservatively managed, were considered to have false positive ECG results yielding a false positive rate of 46% using the ESC criteria and 3% using the Seattle criteria. Over an average of 3.0±1.1 years of clinical follow-up, no adverse cardiac events were observed.
Discussion
This study presents the first comprehensive assessment of ECG characteristics in male and female competitive rowers. Our findings are summarised as follows. First, rowers demonstrated a prevalence of ‘training-related’ ECG findings that exceeded those observed in other sporting disciplines.10 ,13 ,20 The absolute prevalence of these benign adaptations varied by gender, with male rowers more likely than females to have voltage criteria for LVH and anterior lead ERP. Second, our data demonstrate that the application of two contemporary criteria for ECG evaluation in athletes result in markedly different rates of abnormal ECGs. Specifically, the 2010 ESC criteria produced a rate of abnormal ECGs of 47% while the 2013 Seattle criteria yielded 4% abnormal ECGs. This finding emphasises the central role of ECG interpretation criteria in determining the accuracy and downstream clinical implications of ECG-inclusive preparticipation screening among competitive rowers.
ECG-inclusive preparticipation screening, as recommended by numerous sport governing bodies,23 ,24 was recently mandated by FISA for all rowers participating in international regattas.5 This directive stems from the fact that sudden death during sport is most commonly caused by occult cardiac disease that can be detected by ECG.2 ,3 Clinically effective ECG interpretation in athletes requires an understanding of the fact that routine exercise results in a number of cardiovascular adaptations that may manifest on ECG. Exercise-induced cardiac remodelling is sport specific and thus ECG interpretation may best be accomplished with the use of sport specific reference databases.25 To the best of our knowledge, no prior studies have evaluated normative ECG data and the yield of contemporary ECG screening criteria in competitive rowers.
The majority of rowers included in this analysis (94%) demonstrated one or more ‘training-related’ ECG findings. Consistent with recently published data derived from a cohort of mixed-sport endurance athletes,13 the most common training-related changes among rowers included sinus bradycardia, sinus arrhythmia, incomplete RBBB, LVH by voltage criteria, and ERP. The present data set, the first of its size comprised exclusively of rowers, advances our understanding of ECG characteristics among this population in several ways. First, we observed a higher prevalence of sinus arrhythmia (55%) than those reported in a prior study of mixed-sport endurance athletes.13 This is likely explained by the fact that our cohort was confined to rowers and perhaps in part due to the lack of a standardised definition for this common benign arrhythmia. Second, we present the first comprehensive description and clinical correlates of ERP in rowers, an ECG pattern that has recently been implicated as a risk factor for sudden death in the general population.26 Specifically, we found that while ERP in the anterior ECG leads was the most common pattern, ERP in lateral and inferior leads occurred in approximately 25% of rowers. Among a sizable cohort of athletes free of adverse events, the finding of ERP in these non-anterior leads provides further assurance that this pattern is largely a benign adaptation among competitive rowers.27–29 In aggregate, these findings confirm a relatively high prevalence of training-related ECG patterns among rowers and emphasise the importance of recognising these benign findings during the clinical use of ECG.
The most novel finding from this study pertains to the performance of contemporary ECG interpretation criteria. Specifically, application of the 2010 ESC and 2013 Seattle criteria in rowers resulted in widely different rates of abnormal ECGs (47% vs 4%). This discrepancy was largely accounted for by differences in the proposed definitions of several ECG parameters. Abnormal TWI, as defined by the 2010 ESC criteria, was the most common reason for abnormal ECG classification in this study. Importantly, the majority of abnormal TWI based on the 2010 ESC definition were characterised by consecutive TWI confined to leads V1 and V2, which we observed in 27% of our participants. This prevalence is higher than that previously described in a mixed-sport cohort of endurance athletes (10%),13 and in other heterogeneous athlete cohorts (2–5%).12 ,30 ,31 While the precise underlying mechanism of TWI remains incompletely understood, we suspect that the high prevalence of early precordial TWI in rowers may reflect a higher degree of physiological right ventricular remodelling as compared to the other athlete groups.7 ,32
The second most common reason for criteria-specific differential ECG classification was variability in the definition of LAE. The 2010 ESC criteria defines LAE based on consideration of lead V1 findings alone while the 2013 Seattle criteria requires abnormal p-wave morphology in the limb leads (leads I/II) and precordial leads (lead V1). Finally, the limits of the normal QTc range under the 2010 ESC criteria are narrower than those proposed by the 2013 Seattle criteria. Thus, application of the 2010 ESC criteria resulted in mildly prolonged or shortened QTc intervals in a sizable number of rowers that were deemed normal based on the definition proposed by the 2013 Seattle recommendations. There were important gender-based differences in the detection of ECG abnormalities using the ESC criteria, with females having a higher prevalence of LAE and males having a higher prevalence of abnormal QTc, though the overall rate of detection of abnormal ECGs by either criteria were not different based on gender.
There are direct clinical implications that arise from this study. For the first time, quantification of standard ECG parameters and the prevalence of specific ECG patterns have been performed in a sizable cohort comprised solely of rowers. Thus, data presented here may serve as a normative database for use in clinical practice. Our findings emphasise the high prevalence of ‘training-related’ ECG changes in this population and underscore the importance of their recognition among practitioners who utilise ECG in the care of rowers. Second, findings from our comparative assessment of the 2010 ESC and 2013 Seattle interpretation criteria highlight the formidable impact of ECG interpretation schemas when applied in clinical practice. Application of the 2010 ESC criteria led to a 47% abnormality rate which is substantially higher than values previously reported in more heterogeneous groups of athletes.13 ,33–35 This observation indicates that athlete type, a broad term that captures sport specific physiology, age and ethnic distribution, is an important determinant of ECG interpretation criteria performance. Additional single sport cohorts, moving beyond the dichotomous segregation of endurance versus strength-based disciplines, will be needed to facilitate the most meaningful cross-disciplinary comparisons. Finally, as clinicians around the world prepare to conform to recent FISA recommendations for ECG-inclusive preparticipation screening, our data provide a useful framework for predicting the clinical implications of this undertaking. Our observations may prove valuable during the process of ECG interpretation criteria selection, the allocation of resources required for postscreening clinical follow-up, and future efforts aimed at improving the accuracy (ie, improved specificity) of screening practices. Although the 2013 Seattle criteria performed relatively well in this population of competitive rowers, future refinements including reclassification of isolated LAE and TWI prior to the precordial QRS transition zone as normal athlete variants may prove valuable.35
Limitations
There are several limitations of the present study. First, we evaluated rowers enrolled in a single competitive USA collegiate programme at the start of an intensive training cycle. Thus, ECG characteristics among rowers from alternative venues, at different stages of training, or at different competitive levels may differ. However, our cohort contained considerable representation from some of the most dominant rowing countries and many of our participants performed at an international calibre level, thereby suggesting broad generalisability of our results. Second, this study was not designed to determine the cardiac structural and functional correlates of the observed ECG patterns beyond a basic assessment aimed at excluding or confirming the presence of occult pathology. Future work will be required to clarify underlying mechanisms responsible for the observed ‘training-related’ and ‘training-unrelated’ ECG patterns. Finally, we observed only one case of pathology in a population to which it is possible that preparticipation screening had been applied prior to college. We studied rowers over a limited duration of follow-up for clinical events and thus cannot comment on the long-term implications of the observed ECG characteristics. However, the timeframe captured in our clinical follow-up represents a critical time period during which the risk of sport-related adverse cardiovascular events is substantial.1
Conclusions
Among competitive rowers, the prevalence of benign, ‘training-related’ ECG patterns exceeds those seen among athletes participating in other sporting disciplines. In addition, the frequency of abnormal ECG findings varies widely when applying different contemporary athlete ECG interpretation criteria. The relatively favourable performance of the Seattle criteria, particularly if several key refinements can be implemented in the near future, suggests that this framework may be the optimal criteria for use when ECG screening is implemented for rowers under new FISA regulations.
What are the new findings?
-
Training-related ECG changes were present in almost all (94%) of the competitive rowers studied in this cohort.
-
Rowers have a higher frequency of T-wave inversions isolated to lead V1 and V2 than has previously been reported in other athlete groups.
-
Application of the European Society of Cardiology 2010 recommendations for athlete ECG interpretation in this rower cohort resulted in a much higher rate of abnormal ECG classification than did the 2013 ‘Seattle Criteria’ (47% vs 4%).
How might it impact on clinical practice in the near future?
-
This is the first sport-specific reference database for normal ECG findings in competitive rowers, and will be useful in clinical ECG interpretation.
-
ECG screening will newly be applied to large numbers of rowers due to Fédération Internationale des Sociétés d'Aviron (FISA)'s recent mandate to include ECGs in the preparticipation evaluation, and our results suggest that the two contemporary guidelines for athlete ECG interpretation will perform very differently in this group of athletes, a finding that may prove valuable during the process of ECG interpretation criteria selection.
-
Reclassification of common ECG findings in rowers such as T wave inversion prior to the precordial QRS transition zone and isolated left atrial enlargement as normal athlete variants may further improve the specificity of screening practices.
Acknowledgments
The authors wish to thank Harvard crew coaches Charlie Butt, Linda Muri, William Manning, and Billy Boyce and for their on-going partnership. The authors acknowledge the late Harry Parker for his steadfast support of the Harvard Athlete Initiative and his firm belief in the value of sport science. The authors wish to thank Ms. Deborah McDonald for clerical oversight. This study was funded, in part by a research grant from the American Heart Association FTF2220328 (ALB).
References
Footnotes
-
Contributors MMW and ALB were responsible for study design, data acquisition, data analysis and manuscript preparation. JD assisted with study design, data acquisition, data analysis and manuscript preparation. FW, BB and AE assisted with data acquisition and manuscript preparation. KEA, GDL, AMH and RBW assisted with study design and manuscript preparation.
-
Competing interests None.
-
Ethics approval Harvard University Institutional Review Board, Partners Healthcare Human Research Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All published and unpublished data are available for peer review by correspondence with the authors.