Article Text

Abstract
A systematic review of rugby union and league injuries among players under the age of 21 years was carried out to calculate probabilities of match injury for a player over a season and a pooled estimate of match injury incidence where studies were sufficiently similar. The probability of a player being injured over a season ranged from 6% to 90% for rugby union and 68% to 96% for rugby league. The pooled injury incidence estimate for rugby union was 26.7/1000 player-hours for injuries irrespective of need for medical attention or time-loss and 10.3/1000 player-hours for injuries requiring at least 7 days absence from games; equivalent to a 28.4% and 12.1% risk of being injured over a season. Study heterogeneity contributed to a wide variation in injury incidence. Public injury surveillance and prevention systems have been successful in reducing injury rates in other countries. No such system exists in the UK.
- Rugby
- Concussion
- Sporting injuries
- Adolescent
- Child
Statistics from Altmetric.com
Introduction
Rugby is one of the most widely played sports and the third most popular team contact sport worldwide.1 ,2 This sport is increasing in popularity internationally, with 100 countries now occupying a rugby union world ranking and rugby union ‘sevens’ (abbreviated form of 15-a-side rugby union) returning to the Olympic Games in 2016.3 ,4 Rugby union is also a popular competitive school sport and is compulsory in the curriculum of many schools internationally.5–7 While rugby league lags behind rugby union in global popularity,8 ,9 it draws higher numbers of spectators to the stadia and the TV screens than its counterpart in national competitions, such as the Australian championships.10 Professional rugby clubs advocate rugby as a means of tackling childhood obesity,11 which according to the 2009 national survey for England affected between 14% and 20% of 2–15 year-olds.12 While the link between inactivity and childhood obesity has been demonstrated in the past,13 there are no studies showing the weight benefits or social benefits of rugby in children and adolescents.
Several studies have highlighted safety issues due to the physical, high-impact nature of the game14 ,15 and since the game became professional in 1995 the increase in the number of injuries has fuelled concern among parents and health professionals.16–18 Currently, 602 564 male and 129 121 female teenage players are registered with the England Rugby Football Union. According to the International Rugby Board, there are 87 162 teenage male players in Australia and 204 119 male and female teenage rugby players in South Africa.3
Lee et al studied the consequences of injuries sustained in a cohort of Scottish rugby players in the 1993–1994 season 4 years after they had occurred. In players under the age of 20 years, interference in studies (23%), rugby-related injuries (19%) and disillusionment with the game (20%) were the most cited reasons for players giving up the sport.19 The significant impact of injuries on player's well-being and development calls for the institution of measures to help reduce the risk and occurrence of rugby-related injuries.
Our aim was to present the broad spectrum of data on rugby injuries for children and adolescents and calculate the risk of getting injured over a season. Two previous systematic reviews analysed studies on rugby union injuries among young rugby players.14 ,20 Our study expands on this work to include an additional 19 studies providing more detailed and extensive data on injury incidence, nature of injury, and phase and position of play. In addition, we transformed exposure data to calculate the probability or risk of being injured over a typical season when playing rugby and calculated pooled estimates of injury incidence from studies with similar injury definitions. As previous reviews focused mainly on rugby union, we decided not to exclude rugby league or rugby ‘sevens’.
Definition and rules
There are two major variants of rugby: rugby union and rugby league. Rugby union is usually played between two competing sides of 15 players (8 ‘forwards’ and 7 ‘backs’), while a rugby league team has only 13 players. The objective in both is to get the ball over the opposition's goal line by carrying, passing, kicking and grounding the ball.21 ,22
Laws of the game vary between both codes. Some laws of the game are similar for both codes, such as the fact that the ball must not be passed forward or the move known as a tackle, an action where opposition players are allowed to hold and bring the ball carrier to the ground. Differences appear in the concepts of scrum, ruck and maul. Scrums, which involves players pushing against each other trying to get possession of the ball, occurs after an infringement in rugby union or when the ball has gone out of play in rugby league. Scrums carry a far higher injury risk in rugby union as they are no longer contested in rugby league.23 Rucks, which eventuate if “one or more players from each team, who are on their feet and in physical contact, close around the ball on the ground,” and mauls, which occur if at least one opponent holds the ball carrier and one or more teammates bind on the ball carrier, are no longer played in rugby league.21 ,22
Other differences appear in game duration. For example, the UK RFU (Rugby Football Union) stipulates that youth rugby be played in 35 min halves in boys and girls under the age of 19 years in line with the International Rugby Board (IRB) rules but for players under the age of 14 years, a game should consist of two halves of 25 min.24 In Australia however, the duration of an under-19 (U19) match can be up to 90 min.25 The duration of an over-13 rugby league match is 80 min.22 In Australia, a U9 match lasts for 30 min, while a U12 match lasts for 40 min.26
Methods
To identify relevant studies, we conducted a systematic review of the literature, which was followed by an analysis of the injury data. The review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) Statement.27
Eligibility criteria
We searched for any primary research studies which reported data on rugby injury in children and adolescents under 21 years of age.
Information sources
We searched PubMed, EMBASE and SPORTDiscus in April 2014. We hand-searched for references from key systematic reviews and prior work on rugby.
Search
We did not impose any date or other restrictions on our searches. We used the following search strategy for PubMed and adapted it for EMBASE: ((rugby[tiab]) AND ((injury OR injur* OR accident OR accident* OR concussion OR concuss* OR fracture OR sprain OR strain OR contusion OR bruise OR dislocation OR dis-location OR haematoma OR hematoma OR laceration OR cut OR break OR broken))) AND (child OR child* OR adolescent OR adolesc* OR pediatric OR paediatric OR youth OR young OR boy OR girl OR teenage OR teen* OR minor OR school OR college OR university OR student OR pupil).
Study selection
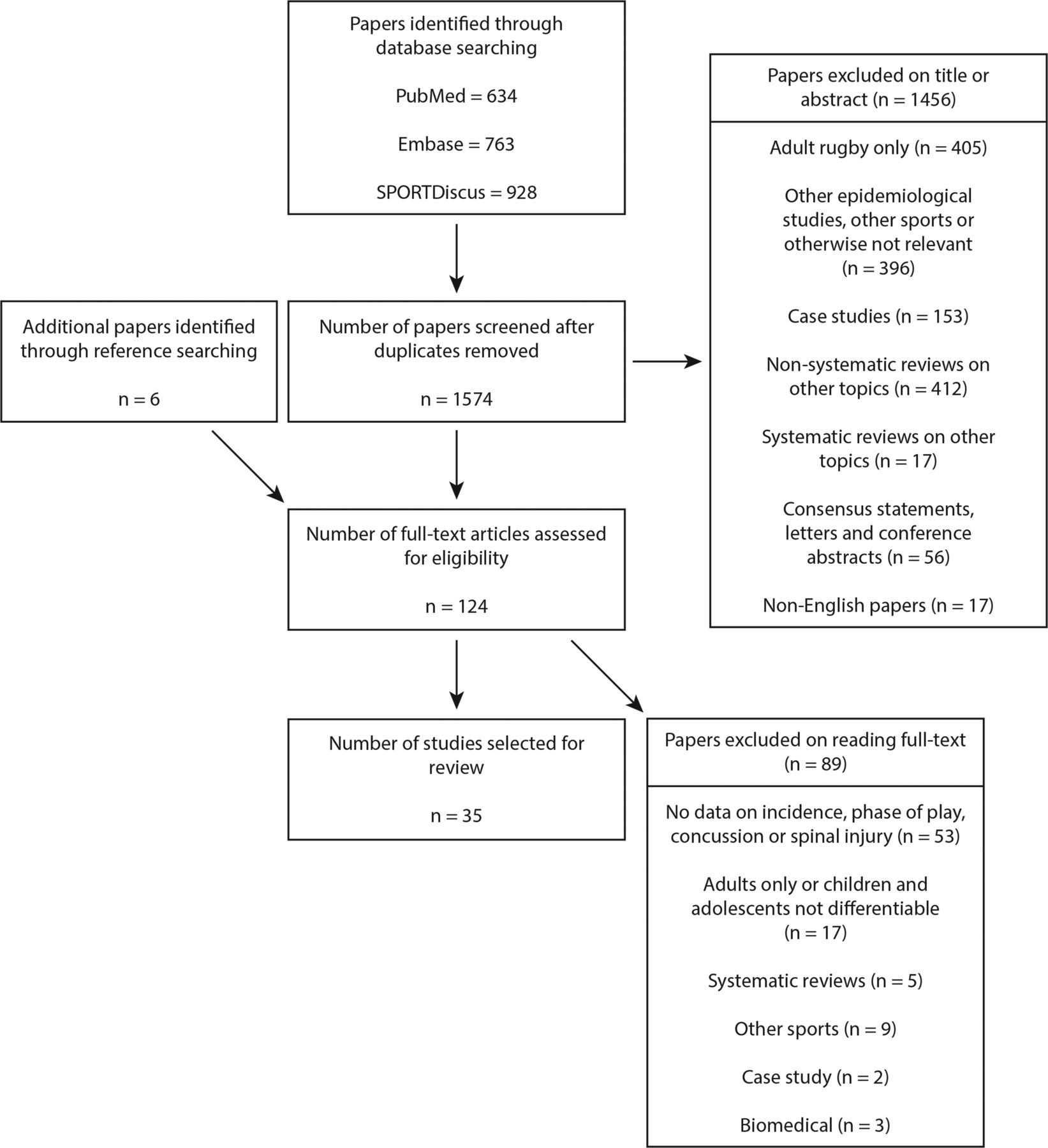
The studies retrieved by our search were initially screened by title and abstract by one reviewer (GK) looking for studies on child or adolescent rugby injury with a second reviewer (AF) double-checking studies rejected at this stage. Studies marked as being potentially useful were then screened again by title and abstract by three reviewers (AF, RO-A and SS) collaboratively where studies potentially containing information fitting our inclusion criteria or being of further use in locating such studies were selected for interrogation of their full text. The full text of these remaining studies was then retrieved either electronically online or if necessary via the Queen Mary University of London facility using the British Library, leading to our final selection of studies for the systematic review. Our inclusion criteria were primary research studies on child or adolescent rugby with data on incidence of injury, type of injury, or phase or position of play associated with injury (see figure 1).

{kind=link}
PRISMA flow chart of literature retrieval and selection.
Data collection process
The selected studies were then investigated further against our study selection criteria by three reviewers (AF, RO-A and SS) collaboratively. Data were extracted from our final group of studies on the topics of incidence (SS), phase and position of play (AF), nature of injury (AF) and concussion (RO-A).
Transforming exposure data to probabilities
Where match injury incidence was given per 1000 player-hours, we used the methods developed by Parekh et al6 to calculate post hoc probabilities of injury over a season for a player with three assumptions: first, that game duration was between 30 and 70 min based on regulations by the IRB and national bodies;21 ,24 ,26 ,28–31 second, that the number of games played per season was 153 ,6 ,32 ,33 and third, that injuries were independent events.
Pooled injury incidence estimates
Where study homogeneity allowed, in terms of injury definitions and reporting of injury incidence as per 1000 player-hours, we calculated a pooled estimate of rugby union match injury incidence (there were not enough studies on rugby league to justify calculating pooled injury incidence estimates). To do this we meta-analysed log incidence rate using the metan command in Stata V.12 (SE of log incidence rate was calculated as square-root of 1/n, where n was observed number of injuries), with random effects to model between study variability. We also report the metan calculated ‘I2’ statistic which varies between 0% and 100% depending on the amount of variation in the pooled incidence estimate due to study heterogeneity. We also report the 95% prediction interval for the pooled incidence rate—that is, a 95% range for the incidence rate that might underlie the observed rate in any given study, taking account of the heterogeneity between studies. We converted the pooled incidences into probabilities of injury over a season using the conservative estimate of 50 min match duration over a 15 game season.
Results
Of 1580 studies found via our publication database and hand searching (minus duplicates) we selected 35 to be included in our final review. Details of exclusions and reason for exclusion are given in the flow diagram below.
Study characteristics
A total of 35 studies were included in this review (see online supplementary table S1): ten from Australia,34–43 five from England,44–48 five from New Zealand,32 ,49–52 four from South Africa,33 ,53–55 three from Scotland,16 ,56 ,57 two from Ireland,58 ,59 two from the USA,60 ,61 two from Canada,62 ,63 one from Great Britain with Ireland18 and one conducted internationally.64
Twenty-six studies were on rugby union,16 ,18 ,32–35 ,39–50 ,53–58 ,61 ,64 three were on rugby league,37 ,38 ,52 two on rugby union and rugby league36 ,51 and four studies did not specify.59 ,60 ,62 ,63 There was no study on rugby ‘sevens’.
Twenty-six studies were on males only,16 ,18 ,32–35 ,37–44 ,46–51 ,53–56 ,58 ,64 seven were on males and females36 ,45 ,57 ,59 ,60 ,62 ,63 and two studies did not specify.52 ,61
Data sources
Most studies, 28 in total, collected data prospectively from matches or training over the course of a season or seasons or during tournaments.16 ,32–35 ,37–54 ,56 ,57 ,60 ,61 ,64 Four studies analysed hospital data which had either been collected previously by emergency department-based injury surveillance systems in Canada62 ,63 and Australia36 or in one study by spinal injury units in the UK.18 Three studies collected data retrospectively from rugby players using surveys or questionnaires.55 ,58 ,59
Definition of injury
In 2007, the IRB provided its own standard definition of injury as “any physical complaint, which was caused by a transfer of energy that exceeded the body’s ability to maintain its structural and/or functional integrity, that was sustained by a player during a rugby match or rugby training, irrespective of the need for medical attention or time-loss from rugby activities. An injury that results in a player receiving medical attention is referred to as a ‘medical-attention’ injury and an injury that results in a player being unable to take full part in future rugby training or match play as a ‘time-loss’ injury.”65 A similar definition was used by Gissane et al66 for rugby league.
In comparison with the IRB injury definitions: 8 studies reported injuries “irrespective of the need for medical attention or time-loss from rugby activities”;34 ,35 ,37 ,40 ,41 ,49–51 3 studies reported injuries using ‘medical-attention’ injury definitions;45 ,52 ,54 14 studies used ‘time-loss’ injury definitions;16 ,33 ,38 ,42 ,44 ,46–48 ,53 ,56 ,57 ,59 ,61 ,64 3 studies used ‘time-loss’ and ‘medical attention’ injury definitions32 ,39 ,60; 3 studies gave no definition for injuries reported;43 ,55 ,58 and in the 4 studies which used hospital data this was not applicable.18 ,36 ,62 ,63
Incidence of injury
We report results where studies gave data on matches and training separately. Altogether, 22 studies reported incidence of injury for matches (see table 1) and 8 studies gave training injury incidences (see table 2). There was heterogeneity in the way incidence of injury was reported. Nineteen of 35 studies reported injuries per 1000 player-hours, 2 studies as injuries per 100 or per 1000 player-games or player-practices; 1 as per 1000 match-exposures or practice-exposures; 1 as per 1000 athletic-exposures; 1 as per 1000 player-seasons and 1 study reported a period prevalence per 1000 playing-hours.
Matches only
Training only
There were 16 studies where match injury incidence was measured per 1000 player-hours; for rugby union, the range was from 3.7 injuries per 1000 player-hours (where the injury was severe enough to prevent a player from playing for at least 7 days) for the U10–U13 age group33 to 129.8 injuries per 1000 player-hours (where any physical complaint caused by rugby was counted) for 14–18 year-olds.50 Only two studies reported match injury incidence per 1000 player-hours for rugby league, 56.8 injuries per 1000 player-hours (where the injury was severe enough that the player missed the next game) among 17–19-year-olds38 and 217.9 injuries per 1000 player-hours (where any pain or disability suffered by a player during a match that required advice and/or treatment was counted) for the U16–U18 age group.52 Five studies gave training injury incidence as per 1000 player-hours with a range from 0.55 injuries per 1000 player-hours (where the injury was severe enough to prevent the player from playing for at least 7 days)53 to 22.4 injuries per 1000 player-hours (where any physical complaint caused by rugby during a match was counted)50 for rugby union, and 56.2 injuries per 1000 player-hours (any pain or disability suffered by a player during a rugby league training session which leads to the player stopping training) for rugby league.37
Probability of injury
Sixteen studies reported match injury rates as per 1000 player-hours. The probability of a player getting injured over a season was between 9% for the U9–U12 age group44 and 98% for the U18 age group.52
Pooled injury incidence
We calculated a pooled estimate of injury incidence of 26.7 (95% CI 13.2 to 54.1) per 1000 player-hours for injuries irrespective of the need for medical attention or time loss from rugby activities from five studies34 ,35 ,49–51 and of 10.3 (95% CI 6 to 17.7) per 1000 player-hours for injuries requiring at least 7 days absence from games, from eight studies.33 ,44 ,48 ,49 ,51 ,53 ,57 ,64 These incidences convert to a 28.4% (15.2% to 49.1%) and 12.1% (7.2% to 19.8%) risk respectively of a child or adolescent rugby player being injured over a season of 15 games of 50 min duration. There was a high degree of heterogeneity detected between the studies under each definition of injury, I2=99.6% in the former and 98.3% in the latter. The 95% predicted interval for the studies where injuries were recorded requiring 7 days away from play was (1.49, 70.82), for studies where injuries were recorded irrespective of need for medical attention or time away from play it was (1.65, 433.26; online supplementary web detail—forest plots).
Types of injury
Concussion was reported by 21 studies and ranged from 2.2% to 24.6% of all injuries recorded (see table 3). Ligament injuries, sprains and strains combined were reported in 11 studies and ranged from 15.7% to 47.2% of all injuries recorded. Fractures were reported in 14 studies and ranged from 3% to 27% of all reported injuries, while laceration, contusion and haematoma combined were reported in 12 studies and ranged from 2.7% to 46% of all injuries recorded. Finally, between 0.5% and 10.8% of all injuries were dislocations and subluxations. The incidence rates for fractures ranged from 0.8/1000 player-hours49 to 11.3/1000 player-hours53 and for concussion from 0.6/1000 player-hours49 to 11.8/1000 player-hours (see table 4).50
Percentage of all injuries by nature of injury and number of studies providing data
Incidence rates per 1000 player hours and probability of injury (%) in a season of 15 games of 70 min duration by nature of injuries (rugby union only)
Severity of injury
In our review, we identified 14 studies which used a ‘time-loss’ injury definition, with seven42 ,44 ,46 ,48 ,56 ,57 ,64 of those providing detailed data on the severity of injury which is defined by the number of days absent from the game.
Moderate injuries (which required a player being absent from playing for 8–28 days) ranged from 21.2% to 68%, while severe injuries (which required a player being absent from playing for more than 28 days) ranged from 5.8% to 32%.42 ,44 ,48 ,64 Palmer-Green et al46 reported that injured players in school had a mean absence from playing of 27 days compared with 33 days for players at academies. In two studies, 9%56 and 13%57 of players were absent from playing rugby for more than 84 days after being injured.
Phase of play
Eleven studies (see table 5), all of which were on rugby union, reported injuries according to phase of play (mechanism). Overall, tackle, which includes tackling and being tackled, accounted for the majority of injuries, with two studies stating that almost half of all injuries were sustained because of tackles (39.6–64%). Being tackled was generally found to account for more injuries (16.5–65%) than active tackling (18.5–40%). Ruck and maul accounted for the third highest rates of injuries (8.3–31.5%) after tackling and being tackled. With one exception, scrums accounted for the fourth highest rates (2–36%).
Percentage of all injuries occurring by phase of play and numbers of studies providing data (rugby union only)
Position of play
Thirteen studies provided data for position of play,32 ,33 ,35 ,39–42 ,48 ,49 ,52 ,53 ,57 ,64 but only seven of those33 ,35 ,40 ,41 ,48 ,49 ,53 provided comparable data on rugby union (see table 6). Injury rates were similar for forward and back positions accounting for between 43.8–56.3% and 43.6–56.3% of all injuries, respectively.
Percentage of all injuries by position of play (rugby union only)
Site of injury
Twelve studies reported data on the site of match injuries. Injuries to the head and neck ranged from 4.6% to 41.2% and to the trunk, from 6.5% to 12.5%. Injuries to the upper limb and lower limb ranged from 19.3% to 38.4% and from 3.4% to 46.8%, respectively.34 ,38–41 ,43–45 ,52 ,56 ,57 ,64
Discussion
Summary of evidence
Our meta-analysis of the studies shows that 28% of child and adolescent rugby players involved in a rugby match playing season are likely to sustain an injury irrespective of need for medical attention or time loss from rugby activities. About 12% are likely to sustain an injury severe enough to require at least 7 days absence from play. The most frequently reported types of injury were sprains, strains, as well as soft tissue injuries although more severe injuries such as concussion and fractures were also commonly reported. The most frequent phase of play cited was the tackle with players being tackled, most at risk of injury while the risk of injury was similar for the playing positions of forwards and backs.
A meta-analysis of injuries in senior men's professional rugby union found an overall match incidence of injury of 81/1000 player-hours under a ‘time-loss’ definition of injury, three times the rate we found under the most conservative definition of injury where injuries were recorded irrespective of time loss or medical attention (26.7 injuries per 1000 player-hours).67 Similar to our findings they found little difference in the incidence of injury between forward and back playing positions, and that muscle/tendon and joint (non-bone)/ligament injuries were the most common injuries.
In his systematic review of paediatric rugby injuries, McIntosh14 concluded that the immediate research priority should be the establishment of prospective standardised injury surveillance projects in youth rugby. We found only two studies which used data collected routinely at hospital emergency departments by injury surveillance systems, from Canada62 and Australia.36 Since there are no such systems in operation in UK hospitals, there are no studies from the UK. A well-established school-based sport injury surveillance system exists in the USA, the high school reporting injuries online system (RIO, Reporting Information Online) but rugby is not one of the sports routinely collected although it is an increasingly popular sport in the USA.68 Also in the USA, the National Collegiate Athletic Association Injury Surveillance System has collected data on rugby since 2005, but only from college and university sport.69 Neither system collects data on children younger than high school age.70
The injury prevention system RugbySmart introduced in New Zealand in 2001 has a focus on reducing spinal injury by educating coaches and officials about player conditioning, safe techniques in contact phases of the game and injury management. Injury claims to the national body of monitoring, prevention and compensation of injury, the Accident Compensation Corporation (ACC), have since declined.71 ,72 Following the success of New Zealand's injury prevention programme, South Africa has launched the BokSmart initiative, which is modelled on the RugbySmart programme. Rugby ready (IRB), Smart Rugby (Australia), Tackling Safety (England) and Rugby RIO High School (USA) are other examples of injury prevention systems.69 ,73 However, injury surveillance systems need to be put in place to monitor the effectiveness of these interventions.
Limitations
The way injury incidence is measured and reported, as per 1000 player-hours, per 1000 athlete-exposures or as injuries per 1000 matches, can result in different findings and different conclusions being drawn, for example over which position is most at risk of injury.74 ,75 Brooks and Fuller74 in their review of methodological considerations in reporting sports studies conclude that comparison of injury incidence between studies where injury definitions are not the same is meaningless. Studies which adopt a medical attention definition have the potential to record higher numbers of injuries, although, such data may be less reliable and may not contain as many injuries of significant clinical importance and interest.20 ,76 For instance, in one study, 79.1% of injuries for which medical attention was sought did not result in a player having to abstain from playing for a certain period of time.50 Counting any physical complaint for which advice was sought could be an explanation for the relatively high incidence rates found in two studies.50 ,52 Thus, the variations in injury definitions may be a cause for the wide ranges reported for nature of injury, phase and position of play. Reporting any injuries without restrictions, as done by Durie and Munroe,49 may for example have resulted in a much lower share of fractures than a definition of injuries severe enough to prevent a player from playing rugby for at least 7 days.53 Another factor which may have contributed to the variation in injury incidence is the issue of who made the injury diagnosis. Similar assumptions have been highlighted by Finch et al77 in their study stating that differences in expertise and knowledge can result in different outcomes of diagnosis. A wide range of personnel, including doctors, nurses, trainers or players self-reporting, were involved in the reporting process among the studies we included in our review.
The combination of match with training injuries in one measure can be misleading especially when attempting between study comparisons.74 Consequently, we only reported injury incidences from studies where these were given for matches and training separately. Match injury rates were consistently higher than training injury rates across all studies where both were included. Our study found injury rates similar to other systematic reviews. Owing to a larger pool of studies, we were able to create more clearly defined subgroups for our analyses, thus providing more accurate injury rate estimates than other studies had done so previously.14 ,20
To make studies and injury surveillance comparable, an international consensus on the definition of injury in regard to injury collection has to be developed and established. A time-loss injury definition is definitely preferable to a medical attention definition, but not less difficult to develop. Whether only injuries that require a player to be taken out of the game or those which result in a player having to stop playing for a certain amount of days should be used, is to be decided by an international consensus.
Furthermore, the large variation seen in site of injury sustained during rugby perhaps highlights that several factors most likely contribute to the injury sustained; namely nature of pitch, speed and body weight of players.20 All studies included in our review found the tackle to be the most common phase of play to be injured, which is consistent with the findings of previous reviews into rugby injury.14 ,20
Conclusions
We found 28% of all child and adolescent rugby players are likely to sustain an injury during a season. Routine injury and sport injury surveillance needs to be improved radically in hospital emergency departments and at schools in the UK to cope with the epidemiological challenges presented by rugby and other sport injury in children and adolescents. The increasing popularity of rugby should accelerate the implementation of injury surveillance systems. Furthermore, injury prevention systems have been established in other countries and have been successful in reducing the number of injuries. A similar system needs to be put in place in the UK.
What is already known?
Playing rugby is a major cause of injury in children and adolescents.
Compared with other sports, rugby has one of the highest incidence rates of match injuries.
There is evidence that injuries to professional and amateur players have increased significantly since the introduction of professionalism in rugby union in 1995.
What does this study add?
Studies show that 28% of rugby playing children and adolescents are likely to sustain an injury over the course of a typical season and that around 12% are likely to sustain an injury severe enough to require at least 7 days absence from play.
Injury rates were similar for forward and back positions.
Being tackled was the phase of play where most injuries occurred.
The most common injury categories are concussion, fractures, ligament and soft tissue injuries.
Acknowledgments
Thanks are due to Dr Nikesh Parekh for background research on rugby injury in children and on the rules of the game.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
- Data supplement 2 - Online table
Footnotes
Contributors AMP conceived the study and obtained funding. AMP, GK, AF, SS and RO-A designed the study and had full access to all of the data in the study. GK, AF, SS and RO-A analysed the data and take responsibility for the accuracy of the data analysis. GK and AF drafted the manuscript with contributions from SS and RO-A. GK, AMP and AF monitored the study through to completion, critically revised the manuscript and approved the final version for publication.
Funding AF and GK are employed under a grant awarded to the Centre for Trauma Sciences project by the Barts Charity.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.