Article Text

Abstract
Background The British Athletics Muscle Injury Classification describes acute muscle injuries and their anatomical site within muscle based on MRI parameters of injury extent. It grades injuries from 0 to 4 and classifies location based on a myofascial (a), musculotendinous (b) or intratendinous (c) description. This is a retrospective cohort study that assessed time to return to full training (TRFT) and injury recurrence in the different British Athletics classifications for hamstring injuries sustained by elite track and field (T&F) athletes over a 4-year period.
Methods The electronic medical records (EMRs) of 230 elite British T&F athletes were reviewed. Athletes who sustained an acute hamstring injury, with MRI investigation within 7 days of injury, were included. MRI were graded by two musculoskeletal radiologists using the British Athletics Muscle Injury Classification. The EMRs were reviewed by 2 sports physicians, blinded to the new classification; TRFT and injury recurrence were recorded.
Results There were 65 hamstring injuries in 44 athletes (24±4.4 years; 28 male, 16 female). TRFT differed among grades (p<0.001). Grade 3 injuries and ‘c’ injuries took significantly longer and grade 0 injuries took less TRFT. There were 12 re-injuries; the injury recurrence rate was significantly higher in intratendinous (c) injuries (p<0.001). There was no difference in re-injury rate between number grades 1–3, hamstring muscle affected, location (proximal vs central vs distal), age or sex.
Conclusions This study describes the clinical application of the British Athletics Muscle Injury Classification. Different categories of hamstring injuries had different TRFT and recurrence rate. Hamstring injuries that extend into the tendon (‘c’) are more prone to re-injury and delay TRFT.
- Hamstring
- Muscle
- Tendon
- Injury
Statistics from Altmetric.com
Introduction
Hamstring injuries are common in track and field,1 football,2 rugby3 and other sports requiring sprinting, acceleration and kicking. They result in significant time loss from sport, but despite recent efforts in the area of prevention and management, hamstring injury and re-injury rates remain high.1 ,2 ,4 The categorisation of hamstring injuries has an important role to play in identifying those injuries that may require specific prevention or management strategies or have different time to return to play (TRTP) or re-injury rates. The ideal features of such a system are reliability and reproducibility, effective prognostication and relevance to clinical management. Classification refers to the categorisation of injury based on key descriptive features and grading provides an indication of severity or extent of injury.
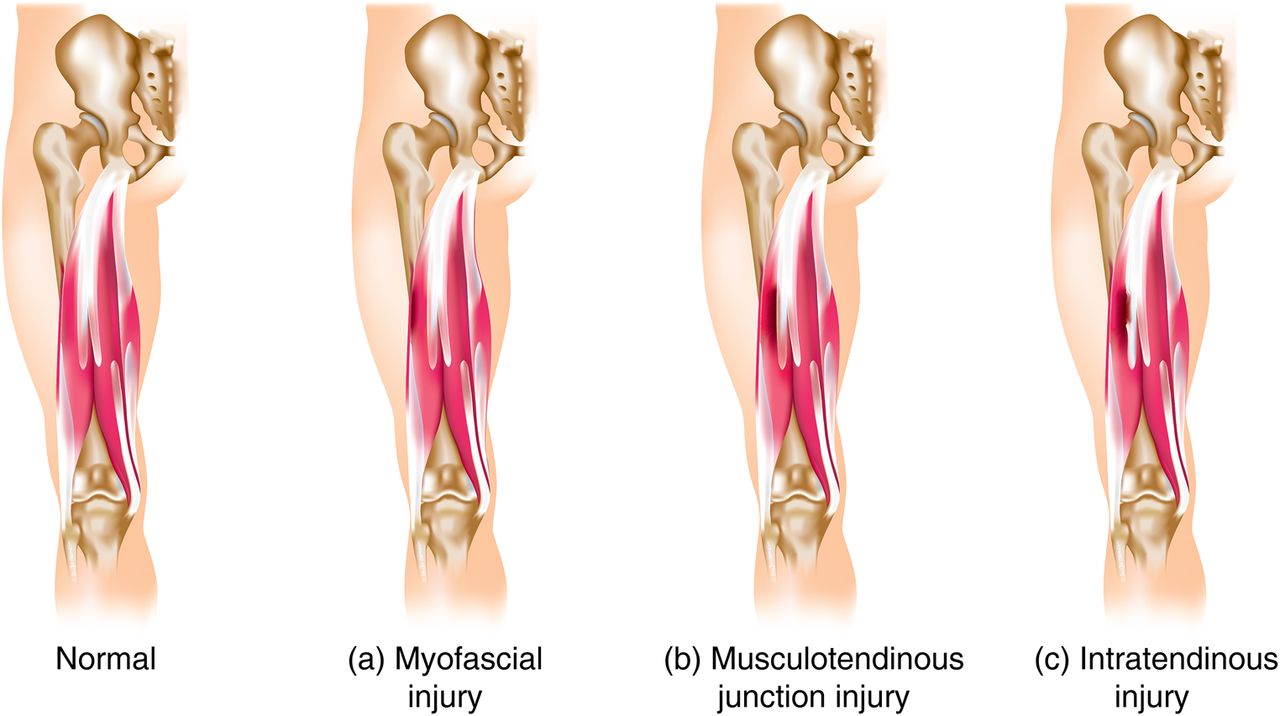
The British Athletics Muscle Injury Classification has classification as well as grading elements. Injuries are classified (a, b or c) according to their anatomical site within the muscle and graded (0–4) based on MRI indicators of injury extent5 (figure 1 and table 1). The most unique feature of this system is the categorical classification and therefore the overarching term for this system is the British Athletics Muscle Injury Classification. Injuries are classified as ‘a’: myofascial; ‘b’: musculartendinous/musculotendinous junction or ‘c’: intratendinous. The grading of injuries from 1 to 4 is based on the MRI measurements of cross-sectional area (CSA) and length of injury within the muscle or tendon. The British Athletics classification system has been demonstrated to have excellent interobserver reliability rates (κ IRR 0.80 and 0.88)6 and MRI parameters in hamstring injury have previously also been shown to demonstrate excellent reliability.7
Summary of British Athletics Muscle Injury Classification (* if any characteristics of a higher grade injury are present the injury is graded at the highest grade)
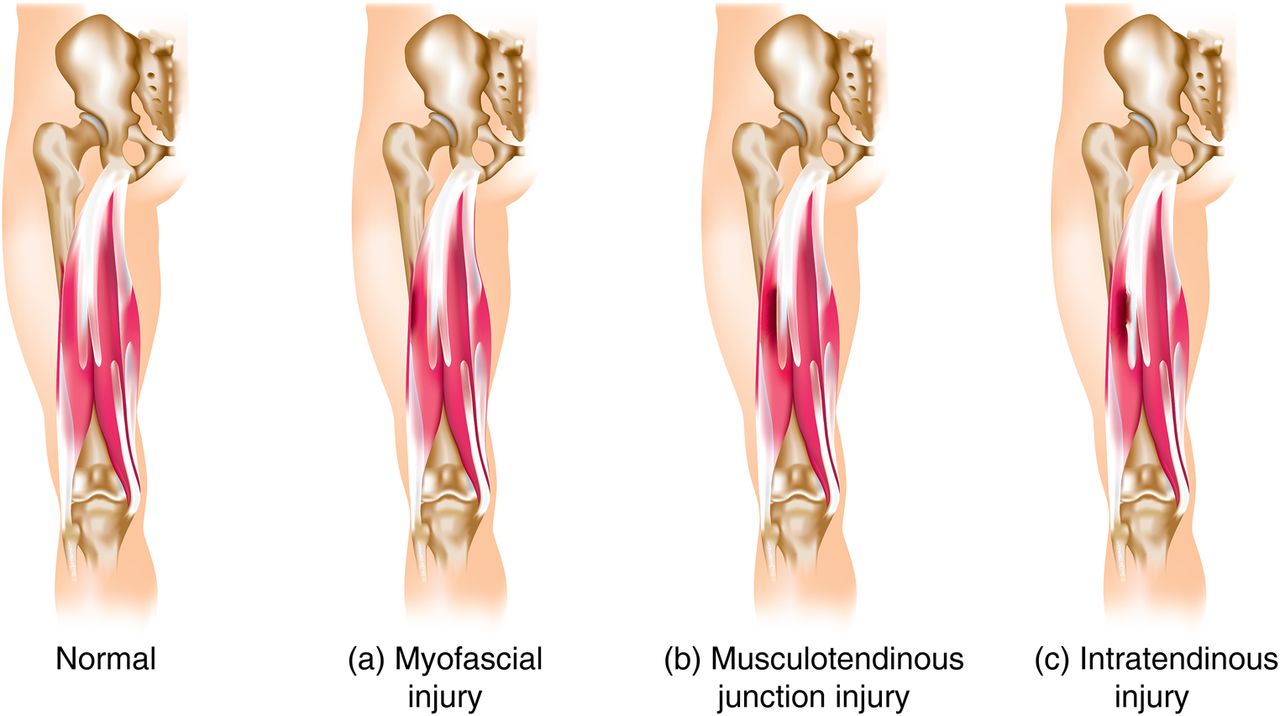
Overview of British Muscle Injury Classification by anatomical site in biceps femoris muscle injury.
Recent research has identified a number of prognostic factors that may influence TRTP. In particular, hamstring injuries that extend into a hamstring tendon have been associated with increased re-injury rate and a longer TRTP.8–10 The length and CSA of high signal change on MRI have been associated with RTP in some studies, although not in a recent study in recreational athletes.11 Unfortunately, this study did not assess intratendon involvement in injuries. Clinical markers such as self-predicted time to TRTP, passive straight leg raise deficit and time to pain-free walking have also been associated with TRTP.11 ,12
Hamstring re-injury rates have been reported between 14% and 63%,13 and consistently around 15–20%. Re-injury is important for athletes, coaches and clinicians in elite sport, as these injuries require the athlete to spend additional time in rehabilitation. It is the aim of the integrated high performance team to enable rapid, yet sustained and consistent return to training and competition. A classification system that could indicate the risk of hamstring re-injury would be of great importance in the elite sport environment. There is inconsistent evidence that size of injury on MRI influences re-injury rates.14–17
The aim of this study was to perform a retrospective review of time to return to full training (TRFT) and re-injury rates for the different injury classifications in the British Athletics Muscle Injury Classification in elite British track and field athletes who sustained a hamstring injury from 2010 to 2014.
Methods
The British Athletics Medical team provided full-time medical care to 230 track and field athletes between 2010 and February 2014, and recorded all injury episodes on a smartabase (profiler) electronic medical record (EMR) system. Injuries were eligible for inclusion in the study if the athlete had reported, between September 2010 and February 2014, an acute injury to the posterior thigh that was subsequently assessed and if the athlete was referred for MRI within 7 days of the injury. The athlete's gender, age, athletic discipline and date of injury was recorded.
A retrospective review of each injury's MRI was independently performed by two specialist musculoskeletal radiologists to classify the injury using the British Athletics classification (table 1). MRI were performed on either a 1.5 T or 3 T MRI scanner at one of four imaging centres in the UK. All MRI included a combination of axial, sagittal and coronal T1-weighted, T2-weighted fat suppressed/proton density-weighted fat suppressed or short τ inversion recovery sequences. The two musculoskeletal radiologists, neither of whom had previously reported the scan, independently reviewed the MRI and reported the British Athletics classification, by recording their findings on MRI proforma (see online supplementary appendix 1). Any discrepancies were discussed and consensus reached as to the appropriate classification.6
A retrospective review of the athlete's EMR was also performed to ascertain TRFT. The TRFT analysis was performed by two sports physicians who independently reviewed the clinical record and noted when a physiotherapist or doctor had changed the athlete's performance status to ‘Fit to Compete’ and confirmed the ability to complete unrestricted training sprint efforts at full pace in spikes. This performance status is formally recorded in each clinical record and includes several categories of readiness to train and compete, charting progression through rehabilitation to return to competition.18 The ethos of the British Athletics team's rehabilitation process is an integrated approach between the medical team and the coach.18 Rehabilitation was provided by full time British Athletics doctors and physiotherapists with a team philosophy of progressive, functional and strength-based rehabilitation, including lengthening loading exercise, and early return to dynamic loading activity, including running, limited by pain. There were no formal TRFT criteria before transition to coach-led sessions as this process was gradual and integrated rather than distinctive. Any discrepancies or gaps in the clinical record were discussed in detail between the clinicians and consensus reached as to the appropriate TRFT. This discussion included review of the athlete's racing schedule from a complete electronic database of race performances (http://www.thepowerof10.info). The clinicians were blinded to the injury's new British Athletics Muscle Injury Classification.
The medical records of these athletes were further evaluated to record injury recurrence to the same hamstring muscle during rehabilitation or within 3 months of return to full training. A recurrence was recorded if the athlete sustained an acute, sudden exacerbation of hamstring pain during exercise, followed by worsening of functional and clinical tests, and requiring cessation of current activity and subsequent modification of rehabilitation or training for greater than 48 h.
The relationships between dependent (TRFT and recurrence) and explanatory (British Athletics Muscle Injury Classification, grade and location of the injury, and muscle injured) variables were tested by Kruskal Wallis, Fisher's exact or r test. If athletes suffered a recurrence during rehabilitation (exacerbation), this injury was excluded from the TRFT analysis. The relationships between TRFT, and the grade and sites (a–c) of the injuries, were examined using linear regression analysis controlled for age and gender. Log transformation of the dependent variable was carried out to normalise data for linear regression. The relationships between recurrence, and the grade and sites of the injuries, were examined using binary logistic regression controlled for gender and age. Age was included as a continuous variable. p Values <0.05 were reported as significant. Statistical analysis was carried out using SPSS 22 (IBM Corporation, New York, USA).
Results
Characteristics of the athletes and the injuries
There were 65 hamstring injuries in 44 athletes, including 31 sprinters, 8 vertical/horizontal jumpers, 3 middle distance athletes, 1 thrower and 1 endurance runner. The study population consisted of 28 males (63.6%) and 16 females (36.4%), and the mean age was 23.8 (SD=4.3, range 18–39) years. Fourteen of the athletes suffered two or more separate injuries. There were 8 injuries in the proximal third, 18 in the central third and 18 in the distal third. The most commonly injured muscle was the long head of biceps femoris (n=28). Other injuries were to the semitendinosus,4 semimembranosus,7 biceps femoris short head1 or multiple muscles.4 (table 2).
Characteristics of the study participants and the hamstring injuries
British Athletics Muscle Injury Classification of injuries sustained
The classifications for the injuries and the mean TRFT and recurrence rates are presented in table 3. There were six injuries that occurred during rehabilitation and prior to return to full training; these injuries have been excluded from the mean TRFT. Even though the grading system is not perfectly ordinal, in this sample of athletes, the categorisation (0–3c) was positively correlated with increasing TRFT (r=0.772, p<0.001, n=59) as is suggested by the mean TRFT per classification (figure 2). Grade 0 injuries were associated with a shorter TRFT than any of the other injury grades (linear regression, p values <0.001).
Mean (SD; range) TRFT in days and injury recurrence rate in different British Athletics classifications, n=65

Mean±SD time (days) to return to full training (BA, British Athletics; TRFT, time to return to full training).
Analysis of British Athletics classification and TRFT
There was a significant difference within the British Athletics Muscle Injury Classifications 1a–3c for TRFT (Kruskal Wallis χ2=16.732, p=0.010). Separate linear regression analysis of grade and site demonstrated that grade 3 severity (p<0.001) and intratendinous (c) site (p=0.008) were associated with an increase in the TRFT. No significant differences in TRFT were found between grades 1 and 2 (t=−1.138, p=0.263) or between classifications (a) and (b) (t=−0.240, p=0.812).
Analysis of British Athletics classification and recurrence
There was a significant difference within the British Athletics classifications 1a-3c with respect to injury recurrence (Fisher's exact test, two-tailed p=0.005, n=44). This variable had two categories (yes/no) and included all recurrences. Separate binary logistic analysis of grade and site suggested that grade was not associated with recurrence (p=0.133–0.968) but that intratendon injuries (c) were associated with a higher risk of recurrence (p=0.002). This significantly increased repeat injury rate was 63% in 2c injuries and 57% in 3c injuries. In comparison, the repeat injury rate in 2b injuries was only 6% (p<0.001) and there were no recurrences in any myofascial (a) injury class (figure 3).

{kind=link}
{kind=link}
{kind=link}
Re-injury Rates (%) in British Athletics Muscle injury groups myofascial (A), musculotendinous (B) and intratendinous (C).
Additional analysis (location, specific muscle)
There was no difference in TRFT (Kruskal Wallis χ2=4.235, p=0.120, n=44) or re-injury (Fisher's exact test, two-tailed p=0.269, n=44) in proximal versus central versus distal injuries. Although six of the eight proximal injuries involved the tendon (75%), these injuries did not demonstrate poorer prognosis compared with the same classification of injury distally or centrally. There was also no difference in TRFT (Kruskal Wallis χ2=1.618, p=0.655, n=40) or recurrence rate (Fisher's exact test, two-tailed p=0.077, n=40) with regard to the specific hamstring muscle involved (biceps femoris long head vs semitendinosus vs semimembranosus vs biceps femoris short head). Neither gender nor age was associated with TRFT or recurrent injury.
Discussion
The British Athletics Muscle Injury Classification has been proposed as a reproducible diagnostic framework that may assist clinicians with categorisation of hamstring injuries, prognostication and clinical management.5 A recent study has demonstrated its reproducibility and reliability.6 This current clinical study provides supportive evidence for aspects of the new classification and its ability to provide relevant information for clinicians in daily practice in track and field.
Most importantly, injuries that extend into the tendon have been demonstrated to be associated with a substantial increased risk of recurrence of injury and an increased TRFT. This study also demonstrated a significant increase in TRFT in the more extensive grade of tendon injury, 3c relative to 2c injuries. Tendon healing occurs in a very different way to muscle repair. Muscle injury induces a satellite cell response and early scaffold on which muscle regeneration can occur enabling early return of muscular function.19 ,20 Tendon repair initiates an inflammatory response characterised by extracellular matrix deposition and a functionally limited scar that requires collagen synthesis and remodelling for return of tensile strength.21 The tendon remodelling phase, which occurs from around 6 weeks after injury, replaces the early type III collagen and extracellular matrix with longitudinally orientated type I collagen.21 ,22 This is necessary to restore the tendon stiffness and function required for athletic activity such as sprinting. It is therefore not surprising that return to sprinting takes longer after intratendinous hamstring injuries. Clinical rehabilitation and monitoring is limited in its ability to replicate the tensile and elastic demands required in tendons during sprinting, and the increased injury recurrence rate in the 2c and 3c classifications is likely to be as a result of athletes returning to sprinting before adequate tendon healing has occurred. A prospective study with controlled rehabilitation parameters is recommended to further assess these intratendon injuries.
This study has added to the literature that demonstrates the positive prognostic indicator of MRI negative in an athlete presenting with an acute hamstring injury.16 ,23 ,24 The British Athletics Muscle Injury Classification describes these grade 0a injuries as microscopic muscle injury or neural (spinal or peripheral) irritation. These injuries usually returned to full training within 13 days, with a very low re-injury rate. No further investigation regarding these injuries, such as clinical or imaging findings of neural involvement or more detailed MRI, was performed as part of this study, but this is a potential area for future research.
Muscle is encapsulated by epimysial connective tissue that is, connected to the deep fascia by fascial expansions. It has been demonstrated to be highly innervated, and the interface between the deep fascia and epimysium includes a layer of hyaluronic acid that enables gliding between these connective tissues.25–27 This work did not demonstrate any significant difference in TRFT or recurrence between myofascial (a) and muscle-tendon junction injuries (b). Although the number of injuries in the myofascial groups in this study was small and further work is required to confirm these findings, it is not unexpected that they would have similar rehabilitation duration of 2–4 weeks. A future area of investigation should assess whether these peripheral myofascial injuries have different mechanistic aetiology or demonstrate differences in clinical examination to warrant separate classification.
This study did not find any difference in TRFT or recurrent injury between proximal, central and distal injury, when controlled for the classification of the injury. However, injuries in the proximal third involved the tendon in 75% of cases. Previous studies have demonstrated a poorer prognosis for proximal injuries,8 but it may be the involvement of the tendon that is, the most important factor rather than the position, proximal or distal, within the muscle. Although there was a consistent trend for an increase in TRFT in grade 2 relative to grade 1, this was not significant in this study when these groups were directly compared. However, the number of injuries in the classes 1a, 1b and 2a was small, and a larger study is required to further assess the relevance of differentiating between these small and moderately sized injuries based on the extent of findings on MRI, for which there is conflicting evidence in the literature.28
There are some elements of the study design that warrant discussion. This study is limited in that it includes a retrospective review of clinical notes. While these notes were generally comprehensive, there were seven injuries that required discussion between the sports physicians to determine TRFT when clinical entries had not been entered every day. The clinical notes did mandate a comment on whether the athlete had returned to full training after each clinical entry, which assisted this review. While the retrospective design meant that the treating clinicians were unaware of the precise British Athletics Muscle Injury Classification when making decisions about rehabilitation progression and return to full training, obviously the variables that compose the British Athletics classification (such as MRI-negative and intratendon involvement) were available to the clinicians and may be a potential source of bias.
Owing to the reality of clinical services in elite track and field, some of the return to full training and competition decisions were made in the context of an upcoming competition such as the World Championships or Olympic Games. As such, athletes with these injuries often had accelerated TRFT whereas injuries that occurred at the end of the season had less competition time pressure. TRFT was used as return to competition is not always a reliable outcome measure in track and field, as athletes may only participate in a small number of competitions throughout the year. However, this may limit the application of the results of this study to other sports.
The British Athletics Muscle Injury Classification appropriately categorises intratendon injuries that appear to require longer to return to full training and are more likely to suffer a recurrence. The numerical grading appears to provide useful guidance on time to return to full training in track and field in MRI negative and extensive injuries, although further prospective work is required on larger cohorts and in different sports to evaluate the importance for TRFT estimation of differentiating between small and moderate sized injuries. However, any diagnostic imaging-based classification is clearly only a starting point on which patient relevant and clinical factors must be added. In conclusion, hamstring intratendon injuries appear to be critically important to recognise in track and field athletes, and seem less likely to respond favourably to accelerated rehabilitation without respect for full healing timeframes, due to a demonstrated high risk of repeat injury. Targeted prevention and management strategies should be focused on this type of hamstring injury.
What are the new findings?
The British Athletics Muscle Injury Classification categorises hamstring injuries based on their anatomical site within the muscle and the extent of injury as seen on MRI.
Injuries that extend into the tendon (‘c’) are associated with longer time to return to full training and have a significantly increased recurrence rate.
MRI appears clinically useful in categorising the type of hamstring injury in elite track and field athletes.
How it might impact on clinical practice?
The British Athletics Muscle Injury Classification warrants consideration for clinicians managing elite track and field athletes.
The recognition and categorisation of intratendon injuries is important; these injuries have a high risk of recurrence.
Acknowledgments
The authors would like to acknowledge the support and clinical expertise of the members of the British Athletics Medical team, past and present, for their contribution to this paper in many ways, but particularly the recording of clinical notes and progression of rehabilitation. The authors also acknowledge the support of Sybermedica, who provided complimentary access to their PACSMail image transfer network during the course of this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Twitter Follow Noel Pollock at @drnoelpollock / Robin Chakraverty @robchakraverty
Contributors NP was involved in study design and lead author. RC was responsible for study design, drafting and sports medicine expertise. SLJJ was involved in radiological expertise and drafting. JC was responsible for review of MRI scans and classification using British Athletics Muscle Injury Classification. AP was involved in review of MRI scans and classification using British Athletics Muscle Injury Classification. AS was responsible for statistical expertise and drafting.
Competing interests None declared.
Ethics approval Ethical approval was granted by Queen Mary University of London ethics panel.
Provenance and peer review Not commissioned; externally peer reviewed.