Article Text

Abstract
Background Interventions to promote physical activity (PA) among older adults can positively impact PA behaviour and other health outcomes. Measurement of PA must be valid and reliable; however, the degree to which studies employ valid and reliable measures of PA is unclear. The purpose of this systematic review was to evaluate the measurement tools used in interventions to increase PA among older adults (65+ years), including both self-report measures and objective measures. In addition, the implications of these different measurement tools on study results were evaluated and discussed.
Methods Four electronic research databases (MEDLINE, PsychINFO, Web of Science and EBSCO) were used to identify published intervention studies measuring the PA behaviour of adults over 65 years of age. Studies were eligible if: (1) PA was an outcome; (2) there was a comparison group and (3) the manuscript was published in English. Data describing measurement methods and properties were extracted and reviewed.
Results Of the 44 studies included in this systematic review, 32 used self-report measures, 9 used objective measures and 3 used both measures. 29% of studies used a PA measure that had neither established validity nor reliability, and only 63% of measures in the interventions had established both validity and reliability. Only 57% of measures had population-specific reliability and 66% had population-specific validity.
Conclusions A majority of intervention studies to help increase older adult PA used self-report measures, even though many have little evidence of validity and reliability. We recommend that future researchers utilise valid and reliable measures of PA with well-established evidence of psychometric properties such as hip-accelerometers and the Community Health Activities Model Program for Seniors (CHAMPS) Physical Activity Questionnaire for Older Adults.
- Physical activity
- Intervention
- Old
- Aging
- Review
Statistics from Altmetric.com
Introduction
Regular physical activity (PA) is essential for healthy ageing. Increasing PA among older adults (aged 65+ years) is a modifiable behaviour with substantial benefits on a number of different health risks.1 While older adults are encouraged to engage in 150 min/week of PA, many have a sedentary lifestyle.2 ,3 This has led to a number of interventions aimed at promoting PA for older adults (aged 65+ years).4 Generally, reviews of interventions to promote older adult PA have been positive and indicate moderate increase in PA behaviour.5–9
There is a need for validated measures of PA specific to the older adult population.10 The investigation of the relationship between PA and health outcomes requires measurements of PA that are valid and reliable.11 However, measurement of PA is difficult since it is a multidimensional construct, and thus cannot be fully captured by one method. Numerous self-report measures and objective measures are currently used to quantify PA.12 ,13 The benefits and limitations of both self-report and objective measures have been widely investigated and discussed,14 but there is yet consensus to be reached on a single best approach to measure PA.15 Briefly, self-report methods are easy to administer and inexpensive, but they are considered less accurate and are vulnerable to recall bias, which has led to various amounts of overestimation and underestimation of PA.16 ,17 Other limitations of self-report methods in studies on older adults include reporting error from anxiety, depression or cognitive impairments,18 and many different self-report methods do not include low intensity activities.19 Conversely, objective methods are considered to provide a more accurate and reliable measure of PA by eliminating recall bias; however, objective methods are more costly and require skilful administration and data interpretation.20
Little is known about how objective measures and self-report methods are used in interventions to increase older adult PA. Instruments devised to measure PA that lack established validity and reliability lead to inconsistent and false-negative results in epidemiological studies.21 Thus, lack of understanding of PA measurement may lead to incorrect conclusions about the efficacy of an intervention.22 Investigating the types of measures employed in interventions for older adults is, therefore, necessary to determine if measurement is being performed adroitly, so that sound inferences can be made from these studies.
The purpose of this study was twofold. The primary objective was to systematically review the different types of measurement used in interventions to increase older adult PA. Additionally, this review investigated the extent to which validity and reliability information on measures of PA were being used correctly.
Methods
Aim and objectives
This systematic review investigated the different types of PA measurement currently being used in interventions for older adults (aged 65+ years). This review also sought to determine the degree to which these interventions were employing measurement principles correctly.
Summary of the search strategy
Systematic literature searches were performed using the electronic research databases. Additionally, the references of relevant reviews of older adult PA were reviewed for any articles to ensure a complete collection of the literature.
Databases
The following databases were initially searched between 9 and 16 February 2014: MEDLINE, EBSCO, Web of Science and PsychINFO. All articles were initially scanned for inclusion between 23 February and 20 March 2014.
Search terms
Title searches were made using combinations of the following search terms: PA level terms (physical activity, exercise); older adult terms (older adults, ageing, aged, seniors, elders, elderly, 65 years and over); intervention terms (intervention, trial, program, efficacy, effectiveness). For example, MEDLINE searches were used as follows:
Physical Activity and Older Adults and Intervention
Physical Activity and Older Adults and Trial
Physical Activity and Older Adults and Program
Physical Activity and Older Adults and Efficacy
Physical Activity and Older Adults and Effectiveness
Exercise and Older Adults and Intervention
Exercise and Older Adults and Trial
Exercise and Older Adults and Program
Exercise and Older Adults and Efficacy
Exercise and Older Adults and Effectiveness
This process was repeated until all search term combinations were performed.
Filtering
The first author (RF) initially screened and identified studies based on the study title and abstract. Articles that mentioned PA in either the title or abstract were initially included. Duplicates and articles failing to meet inclusion criteria were manually removed. The remaining studies were thoroughly reviewed to determine if they met eligibility criteria. Eligible studies meeting criteria were coded.
Study criteria
Types of study
Controlled as well as uncontrolled intervention trials, whether randomised or not, were identified and included in this review. Studies needed to have utilised a control or comparison group in order to be included. Articles were excluded if they were: (1) non-peer reviewed articles; (2) non-English language publications and (3) unpublished theses.
Types of participants
All studies in which the participants were clearly described as being ≥65 years of age were included. No restrictions were made about the study sample aside from the age restriction.
Types of Intervention
Interventions to increase PA or exercise were included. Studies not designed to increase PA or exercise were not included.
Types of outcome measures
Studies were required to have measured PA at baseline and follow-up, with the purpose of assessing change. Studies not including information on changes in PA were not included. These inclusion and exclusion criteria were determined in order to investigate the quality of measurement in older adult interventions that were specifically designed to increase PA.
Data collection
Data were extracted systematically using a specifically designed data extraction form. Data were extracted from selected articles regarding: (1) use of randomisation; (2) study length; (3) sample characteristics and (4) the measure(s) used. All information was placed in a spreadsheet for reference.
Assessment of PA measurement quality
The quality of a study's PA measurement was assessed by extracting information regarding the methods, design and purpose of the PA measure(s) utilised in the study. Information about the PA measurement protocol included the following aspects: (1) the measure used; (2) the citation of a measurement study in regard to the tool used; (3) evidence of validity and reliability and (4) population specificity.
Type of measure of PA
The measures used in these interventions were placed into two broad categories: self-report and objective measures. The following measures were considered as self-report: diaries or logs, questionnaires, surveys and recall interviews. Objective measures included: doubly labelled water, indirect or direct calorimetry, accelerometers, pedometers, multisensor armbands, heart rate monitoring and direct observation.
Citation of a measurement study
A measurement study is one in which the primary purpose of the study is to determine validity or reliability of a measure. The assessment of proper citation of measurement studies included the following inquiries: (1) citation for reliability; (2) citation for validity and (3) the study cited for evidence of validity or reliability was indeed a measurement study.
Evidence of validity and reliability for the PA measure used
The reliability of a measure refers to the degree to which measurements of the same trait are reproducible under the same conditions.23 The reliability of a measure is an important means by which a measure can be deemed to have accuracy and consistency.24 The assessment of a measure's reliability protocol included inquiries on the following measurement properties: (1) the measure used in the intervention had previously established reliability; (2) the intervention study determined reliability of the measure used within the sample and (3) the psychometric properties (ie, Cronbach's α, interclass correlations, inter-rater correlation) of a measure's reliability were reported in the intervention study, either from previous reliability data or from within sample data.
The validity of the measure can be best described as the soundness of the interpretations of the results of a test by which accurate conclusions may be drawn to the results.25 There are several different types of validity (eg, criterion-based validity), which, when used in summation, may add to the evidence of the validity of the test.26 Briefly, criterion-based validity is evaluated by comparing the test scores with one or more external variables (called criteria) that are considered to provide a direct measure of the characteristic or behaviour in question. Our assessment of validity of the measures used in interventions to increase older adult PA included inquiries on the following properties: (1) the measure used in the intervention had previously established validity; (2) psychometric properties (ie, R2 and r) of the measure's validity were reported in the intervention study, either from previous validity data or from within the sample and (3) there was evidence of criterion-based validity for the measure used in the intervention.
Population specificity of the PA measure used
Population specificity refers to the characteristics of a sample by which a measure was validated. The specificity of a population can refer to a number of different characteristics such as age, ethnicity or sex. To avoid greatly reducing the ability to accurately interpret findings, researchers should avoid using tools that solely have validity and reliability established for populations that differ from the one they are presently measuring, as this greatly reduces the ability to accurately interpret findings.27 Population specificity of a study's measurement tool was assessed via: (1) determining if the population for which reliability was calculated was an older adult population and (2) determining if the population for which validity was calculated was an older adult population.
The evaluation included a total of nine questions on proper measurement use. The two principal authors (RF and SM) independently rated the quality of the PA measurement of the individual papers, and consensus was achieved through discussion. Discrepancies were settled by the third author (MB).
Data analysis
Information extracted from the articles was placed in a spreadsheet. The information extracted was then used to calculate averages and ranges across all studies for study demographics. Information regarding PA measurement was also recorded in the spreadsheet. The measure(s) used was first recorded for each study, and then a binary system was used (1=Yes, 0=No) for each of the items of interest (ie, type of PA measure, citation of a measurement study, evidence of validity and reliability, etc). Percentages and averages were then calculated for each of the areas of interest.
Results
Search results
Figure 1 describes the results of our search. A total of 6312 hits were identified. Of these, 512 titles were selected for further screening. After removing 291 duplicate titles, 230 article abstracts were scanned for inclusion, of which 165 were eliminated. The remaining 65 studies were assessed for eligibility and an additional 28 were removed, yielding 37 studies eligible for review. The most frequent reasons for exclusion were: (1) participants were under 65 years of age or (2) the study did not measure PA. Seven additional studies were identified through reference scanning, resulting in a total of 44 studies for the final review.
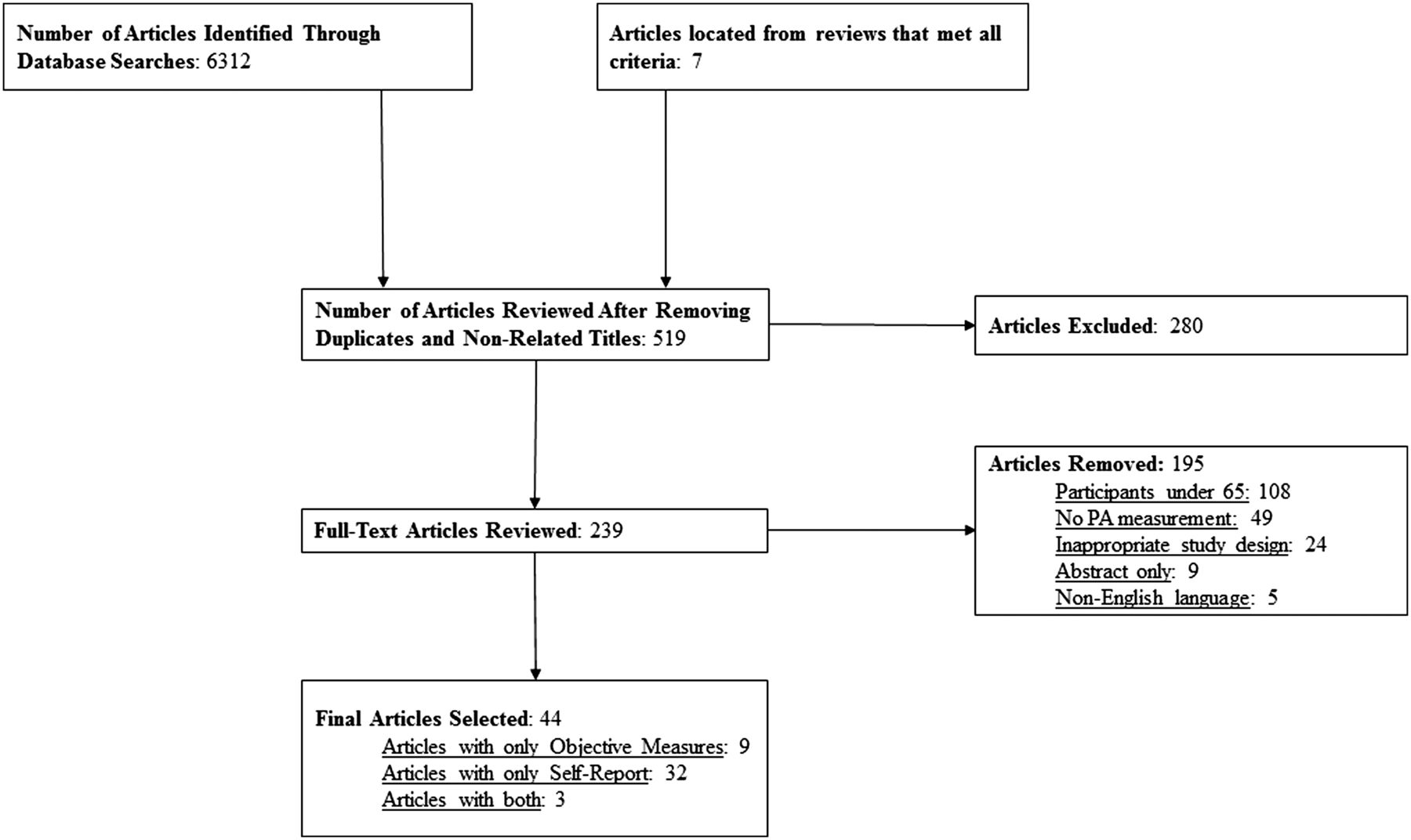
{kind=link}
Flow chart of the identification of interventions for inclusion in the study.
Summary of article characteristics
The average duration of the studies reviewed was 8.6 months,28–71 with 93% employing randomised trials.28–38 ,40–51 ,53–55 ,57–66 ,68–71 Sample sizes for the studies ranged from 15 to 1800 participants. Age of the participants across the studies varied considerably (65–92 years). Of the 8493 participants in these studies, 59% were female.
A wide variety of samples were obtained from many different locations including North America and Europe, as well as Asia. Additionally, the samples gathered were composed of healthy populations, and also populations that were living with different health conditions and comorbidities such as heart disease,28 ,71 diabetes65 and urinary incontinence.62
A total of 33 different measures were used to assess changes in PA behaviour and energy expenditure in these interventions (table 1). Objective measures were used in 12 of the studies reviewed while self-report were used in 32 studies.28 ,31 ,32 ,34–38 ,40–48 ,50 ,51 ,53–55 ,57–61 ,63 ,64 ,66 ,69 ,70 Six studies used multiple measures29 ,33 ,39 ,47 ,52 ,62 and three studies used a combination of objective measures and self-report.29 ,33 ,39
Use and frequency of different measures used across studies
Studies using self-report
Use of self-report by study
There were 32 studies that measured PA via self-report.28 ,29 ,31–48 ,50 ,51 ,53–55 ,57–61 ,63 ,64 ,66 ,69 ,70 Among those using self-report, four studies used multiple measures,29 ,33 ,39 ,47 with three of them also using objective measures,29 ,33 ,39 and the remaining study utilising two different self-reports.47 Studies using self-report ranged in size from 16 to 1800 participants.28 ,29 ,31–48 ,50 ,51 ,53–55 ,57–61 ,63 ,64 ,66 ,69 ,70
Measures used
Online supplementary table S1 describes the different measures used to determine PA behaviour. Of the 32 studies that used self-report, the most commonly used measure was the Community Health Activities Model Program for Seniors Physical Activity Questionnaire (CHAMPS); it was used in eight studies.34 ,35 ,43 ,46 ,48 ,55 ,64 ,70 Other frequently used self-reports included the Physical Activity Scale for the Elderly (used in three studies as the primary measure of PA, and once as a secondary measure)3 ,32 ,33 ,47 and the Yale Physical Activity Survey (used in two studies as a primary measure of PA, and once as a secondary measure).39 ,58 ,59 Three separate studies used unnamed questionnaires.41 ,42 ,54
Studies using objective measures
Use of objective measures by study
Of the 12 studies that utilised objective measures, 6 used hip accelerometers,29 ,49 ,52 ,62 ,68 ,71 2 used wrist accelerometers56 ,65 and four studies used pedometers.30 ,33 ,39 ,67 Additionally, two studies used direct observation as a secondary measure of PA (hip accelerometry was the primary measure in both these studies).52 ,62 Among studies that used objective measures, multiple measures were used in five studies,29 ,33 ,39 ,52 ,62 three of which used self-report as a secondary measure.29 ,33 ,39 The remaining two studies that employed multiple measures used direct observation,52 ,62 as previously mentioned. Studies using objective measures ranged in sample size from 15 participants to 280.29 ,30 ,33 ,39 ,49 ,52 ,56 ,62 ,65 ,67 ,68 ,71 Among studies using accelerometers to investigate PA behaviour, sample sizes ranged from 23 to 280,38 ,57 ,59 ,63 ,68 ,70 ,72 and sample sizes among studies utilising pedometers also varied (15–263 participants).30 ,39 ,42 ,48
Measures used
Of the six studies that measured PA with hip accelerometers, two studies used the RT329 ,71 and two studies used the MTI Actigraph;49 ,68 the other two studies used the Caltrac Motion Sensor62 and the Caltrac Personal Activity Monitor.52 Neither study that measured PA with wrist accelerometers used the same device. Finally, two of the four pedometer studies used the Yamax Digi-Walker SW-200 device;33 ,39 the remaining two pedometer studies used the HJ-720ITC Digital Pedometer30 and the Kenz Lifecoder EX.67
Measurement properties of PA measures
Citation of measurement tools
Online supplementary table S1 describes the quality of measurement for each study and table 2 describes the measurement quality across all studies. Citations for reliability were found for 59% of the measures used across studies (43% of objective measures and 65% of self-report),28 ,29 ,31–35 ,37 ,39 ,41 ,43–47 ,55 ,57–59 ,61 ,63 ,64 ,66–68 ,70 ,71 and citations for validity were given for 63% of the measures (50% of objective measures and 68% of self-report).28 ,29 ,31–36 ,39 ,41 ,43–47 ,49 ,55 ,57–61 ,63 ,64 ,66–68 ,70 ,71 Of the citations for reliability, 100% of the studies using objective measures cited a measurement study,29 ,33 ,39 ,67 ,68 ,71 while 88% of the self-report cited a measurement study.28 ,31–35 ,37 ,39 ,43–47 ,55 ,57 ,58 ,59 ,61 ,64 ,66 Measurement studies for validity were cited for 100% of the studies using objective measures29 ,33 ,39 ,49 ,67 ,68 ,71 and 88% of the self-report methods.28 ,29 ,31–37 ,39 ,43–47 ,55 ,57 ,58–61 ,64 ,66
Properties of measurement across studies
Measures with validity and reliability
Only 61% of the measures used in the interventions reviewed had previously established reliability (43% of objective measures and 68% of self-report).28 ,29 ,31–35 ,37–39 ,41 ,43–48 ,55 ,57 ,58 ,59 ,61 ,64 ,66–68 ,70 ,71 Validity had been previously determined in 73% of the measures used (64% of objective measures and 76% of self-report).28 ,29 ,31–39 ,41 ,43–46 ,48 ,49 ,52 ,55 ,57–62 ,64 ,66 ,67 ,68 ,70 ,71 Both validity and reliability had been established in 67% of the measures utilised across interventions (64% of objective measures and 68% of self-report),28 ,29 ,31–39 ,41 ,43–49 ,52 ,55 ,57–62 ,64 ,66–71 with 29% of the measures used in these studies having neither reliability nor validity.29 ,30 ,40 ,42 ,47 ,50–54 ,56 ,62 ,63 Within sample reliability was only collected in 7% of the interventions,28 ,31 ,38 and only for studies using self-report. Psychometric properties for the PA measures were provided in only 16% of the studies reviewed.28 ,29 ,31 ,38 ,46 ,58 ,66 ,67
Criterion-based validity
Of the studies using measures with pre-established validity, 64% of the measures were validated by a criterion measure.29 ,31 ,33 ,37 ,39 ,44 ,45 ,47 ,49 ,52 ,57 ,58–60 ,64 ,67 ,68 ,71 For these studies, 100% of the objective measures with pre-established validity were validated against a criterion measure,29 ,33 ,39 ,49 ,52 ,67 ,68 ,71 while only 60% of self-report with pre-established validity were validated against criterion measures.29 ,31 ,33 ,37–39 ,44 ,45 ,47 ,57–60 ,64 Additionally, 71% of valid objective measures used a criterion measure to validate energy expenditure estimates,39 ,49 ,52 ,67 ,68 and 100% of valid objective measures were validated against a criterion measure to estimate PA.33 ,39 ,49 ,52 ,67 ,68 ,71 One study provided a citation for validity, however, the accelerometer used in the validation study was not the same device as the one used in the intervention.71
Population specificity
Population-specific reliability studies were cited for 33% of the studies using objective measures that cited a measurement study,39 ,71 while 63% of the studies using self-report cited population-specific reliability studies.28 ,32–35 ,37 ,39 ,41 ,43 ,46 ,47 ,55 ,58 ,59 ,64 ,71 Only 29% of the studies using objective measures (that also cited a measurement study)39 ,71 and 77% of studies using self-report cited a population-specific validity study.28 ,32–37 ,39 ,41 ,43 ,46 ,47 ,55 ,58–60 ,64
Discussion
We investigated the different types of PA measures currently being used in older adult (aged 65+ years) interventions. There are many weaknesses to the current measurement practices in interventions to increase older adult PA. While the limitations and weaknesses of assessing PA by self-report are well known,73 it appears that much of the present literature has relied on it as the sole means to quantify PA. Additionally, a large number of these published studies do not provide evidence of validity and reliability.23 Moreover, 29% of the studies reviewed provided no evidence of validity or reliability.
PA and self report
The self-report methods utilised in the studies reviewed differed widely in their ability to accurately and reliably measure PA in older adults. Some of these measures, such as the Physical Activity Scale for the Elderly, have both criterion and construct validity.74 However, a substantial number of the self-report methods currently being used in interventions have no previous investigations of either criterion validity or construct validity.
While self-report, including the more detailed PA questionnaires and activity logs, can provide important information on multiple constructs of PA in older adults, key limitations to their use exist. Age-neutral questionnaires were used in several of the selected studies, which often fail to include types of activities regularly participated in by older adults.72 Walking is the most common activity in which older adults participate,75 and older adult interventions that choose to utilise self-report should use a measure that specifically measures walking intensity.17
Older adults also tend to participate in lower intensity exercise more often than they do in moderate or vigorous PA.76 Moreover, their PA participation is often intermittent, sporadic or unstructured, thus making recall extremely difficult.77 Over-report bias is a common phenomenon of any type of self-report,78 which may lead to inflated results. Since it is recommended that interventions to increase older adult PA focus on behaviour change principles,10 ,79 participants will be more likely to respond favourably to increased PA since they know what the study is interested in changing. This alone draws into question the likelihood that PA can ever be accurately estimated from self-report, since the measurement will always be influenced by the prompting of the intervention to increase PA.
Another issue is that low validity coefficients exist between self-report methods themselves,80 which makes it impossible to determine a common score of PA across self-report assessments. Moreover, self-report possesses low validity coefficients when compared to criterion measures, with varying degrees of over-reporting and under-reporting of PA and energy expenditure.77 ,81 ,82 This effect of compounding error creates a great deal of difficulty for researchers trying to interpret the effect of the intervention.
Despite the significant limitations of self-report, these measures can provide rich information about PA behaviours. For example, self-report methods potentially offer information regarding the types of PA in which individuals participate.83 Moreover, these measures provide environmental information regarding PA, such as where PA takes place.84 Because of these unique attributes of self-report, which cannot be ascertained from objective measures, it is suggested that utilisation of both self-report and objective measures provides the most complete picture of PA.85 Given the evidence of validity and reliability currently available for hip accelerometers and also for CHAMPS, we suggest that future interventions use these measures specifically, and both measures, if possible.
PA and objective measurement
Unlike self-report methods, objective measures are less susceptible to subjectivity and tend to yield more accurate results regarding PA behaviour. Most of the objective measures used in the studies reviewed showed both validity and reliability. However, even with established validity and reliability, objective measures are not immune to limitations. A previous review of accelerometers used in surveillance data noted that accelerometers may provide underestimations for total PA, inaccurate estimates of PA for many common activities (ie, cycling, resistance training, swimming, etc), and often yield results that are not generalisable to the target population.86
Another issue among objective measures used in older adult interventions is, no study has conducted within-sample reliability; nor has inter-rater reliability been conducted for measures utilising direct observation. Inter-rater reliability, given the inherent limitation of relying on observer report, is considered to be necessary to insure accurate measurement by a direct observation measure.87 In addition, the lack of validity data for direct observation measures makes these estimates of PA behaviour even more suspect.
A final concern is, few objective measures used had any population-specific validity or reliability, which are essential components of proper measurement procedure.88 Measures tested in populations other than the one specific to the investigation may yield inaccurate measurements when used. This ultimately can lead to a great deal of both random and systematic error that may confound the true results of the study. Given that the objective measures being used in this review were scarcely tested on older adult populations, a large degree of error may have been introduced to these studies. This issue can be best highlighted with the example of several of the accelerometers having been validated in children, a population with vastly different PA patterns.89 It is unlikely that even the most highly active group of older adults have similar PA behaviour to any population of children.
Researchers conducting interventions to increase older adult PA must therefore consider what type of measure they intend to use for investigating PA changes, and whether the measure is validated for that population. For example, researchers conducting an intervention to increase PA among frail older adults should avoid using a measure that has only been validated in healthy older adults, and vice versa. Failing to use a measure specifically validated in the population of interest may lead to inaccurate results.
Best practices for interventions
It is important that older adult interventions utilise PA measurement tools in a manner that is consistent with the principles of measurement. However, the current body of older adult interventions to promote PA appear to have relied heavily on self-report methods, with many of these measures failing to show evidence of validity or reliability. Thus, future interventions for older adults should make use of the following recommendations.
Recommendations
Properly designed measurement must become a priority if sound conclusions are to be drawn from interventions. Presently, there is not enough evidence to conclude that objective measures are always more suitable than self-report.86 However, there is certainly a growing body of evidence to suggest that PA should be measured objectively whenever feasible in order to draw accurate conclusions about the effects of an intervention. At the very least, interventions designed to increase PA among older adults must use valid and reliable measures. The continued use of measures without any validity or reliability is making the conclusions drawn from these studies questionable at best, and downright wrong at worst.
For a consensus to be reached about the effect of interventions currently being conducted on older adults, PA must be measured by a standardised procedure. In the interim, it is difficult to expect researchers to be able to assess consistencies and similarities between successful interventions, since it is impossible for us at this time to be able to identify successful interventions. For researchers to show that an intervention is successful at increasing PA, we must know that they are using valid and reliable measures that have similar measurement methodologies to previous research, and are choosing appropriate tools to measure the construct of PA that is expected to change following the intervention.
Finally, the different constructs within PA (eg, intensity, frequency, mode, duration, etc) require researchers to be specific and knowledgeable about the measure that they wish to use. Since PA is now a multiconceptual domain, researchers need to be familiar with how to measure PA properly. At the very least, interventionists need to have someone on their staff familiar with these concepts of PA measurement.
Limitations
Not all studies that fit our inclusion criteria may have been included. There is also no set definition for the age at which someone becomes an ‘older adult’, which leads to a great deal of heterogeneity in the age populations of reviews of older adult PA. Our inclusion criteria restriction for age (65+ years) may have limited the number of studies included. In addition, perhaps only studies investigating the oldest of the old are assessing PA less than optimally, while studies that are using younger older adults (ie, aged 55–65 years) are assessing PA more accurately and rigorously. However, the studies that were reviewed were heterogeneous in regard to a number of sample characteristics, including age. Of final concern, a publication bias may exist such that more valid and reliable measures of PA (both self-report and objective measures) are used in studies that do not find publishable results. This lack of publication for more rigorous measures may have potentially skewed our findings towards the null via inflated type I error.
Summary
It is critical that interventions aimed to increase PA among older adults implement measures of PA that are both valid and reliable. Considerable work is needed in order to ensure that interventions to promote PA are being measured properly. Significant issues still exist with how PA is being measured within older adult interventions, regardless of whether these interventions are using self-report or objective measures. Researchers must be cautious when choosing a measure of PA for their intervention and when comparing PA levels across studies, especially when no standardised measurement procedures or tools are being utilised across interventions.
Summary
Most physical activity interventions in older adults are using self-report measures, rather than objective measures of physical activity.
Many of the measures currently being used in older adult interventions lack basic properties such as evidence of validity and reliability.
Researchers implementing older adult physical activity interventions must understand how to perform proper measurement of physical activity in order to draw valid conclusions.
Standardised procedures for physical activity measurement in older adult interventions need to be developed so that common measures are used across studies, thus allowing for proper interpretations of the efficacy of these interventions.
Acknowledgments
The authors would like to acknowledge Dr Glenn Landry for his invaluable help with writing the final manuscript and Dr Jennifer Davis for final edits.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors RSF was the primary author of this manuscript, having planned and written the review. SMM and MWB were involved with planning and also editing the review. KB contributed as a reviewer and provided edits to the manuscript. TL-A was the supervising author for this manuscript. She helped with editing and writing.
Competing interests TL-A is a Canada Research Chair Tier II in Physical Activity, Mobility and Cognitive Neuroscience.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Warm up