Article Text

Abstract
Background Musculoskeletal pain is common and its treatment costly. Both group and individual physiotherapy interventions which incorporate exercise aim to reduce pain and disability. Do the additional time and costs of individual physiotherapy result in superior outcomes?
Objective To compare the effectiveness of group and individual physiotherapy including exercise on musculoskeletal pain and disability.
Methods Eleven electronic databases were searched by two independent reviewers. Randomised controlled trials (RCTs) including participants with musculoskeletal conditions which compared group and individual physiotherapy interventions that incorporated exercise were eligible. Study quality was assessed using the PEDro scale by two independent reviewers, and treatment effects were compared by meta-analyses.
Results Fourteen RCTs were eligible, including patients with low back pain (7 studies), neck pain (4), knee pain (2) and shoulder pain (1). We found no clinically significant differences in pain and disability between group and individual physiotherapy involving exercise.
Conclusions Only small, clinically irrelevant differences in pain or disability outcomes were found between group and individual physiotherapy incorporating exercise. Since all but one study included other interventions together with exercise in either the group or individual arm, deciphering the unique effect of the way in which exercise is delivered is difficult. Group interventions may need to be considered more often, given their similar effectiveness and potentially lower healthcare costs.
- Exercise
- Physiotherapy
- Evidence based review
- Meta-analysis
Statistics from Altmetric.com
Introduction
Musculoskeletal (MSK) conditions are a common and costly source of pain and functional disability, resulting in a significant personal, social and economic burden.1–3 Collectively, they cause 21.3% of the total years lived with disability in the world, affecting one in four adults in Europe alone.4 Low back pain (LBP) has the highest global burden of disease, with neck pain ranking fourth, and other MSK conditions ranking fifth.5 ,6 Finding effective interventions for the management of MSK conditions is therefore of utmost importance.
Physiotherapy management of MSK conditions commonly consists of exercise and passive adjuncts, including manual therapy, electrotherapy and thermal modalities.7 ,8 However, passive therapies provide only short-term benefits.9 ,10 Exercise is probably the most effective component of physiotherapy for a range of MSK conditions; many systematic reviews and randomised controlled trials (RCTs) corroborate its benefit in reducing pain and disability.11–19
Physiotherapy that includes exercise can be supervised individually or in groups. Both modes have been shown to be more effective than waiting list control groups and non-supervised programmes (eg, home exercise programmes).20–26 Individual physiotherapy is the most widely adopted approach for MSK conditions.27 However, group physiotherapy may be as effective.18 ,28 Advantages of group physiotherapy include the social interaction for participants and the lower cost compared with individualised care.18 Although it is clear that group and individual physiotherapy interventions that incorporate exercise are better than minimal or no treatment, it remains unclear whether either is better than the other. In addition, many people with MSK conditions appear to be either overtreated or treated inefficiently, without improving their outcome.29–32
A recent rapid review33 of five databases investigated the effectiveness of group education and exercise interventions in people with osteoarthritis and chronic LBP. Interventions that included group education were as effective as individual physiotherapy and medical management. In that review,33 group interventions were not required to be delivered by a physiotherapist and the authors included group education interventions that contained some individual sessions. The group interventions were compared with several different treatments (individual physiotherapy, usual medical management, booklets and no intervention), while the control interventions were not required to have an exercise component.
No systematic review has compared physiotherapist-delivered group-only and individual-only programmes that incorporate exercise across all MSK conditions. Therefore, the primary objective of this systematic review was to assess the comparative effectiveness of group and individual physiotherapy programmes that incorporate exercise on pain and disability in patients with MSK conditions.
Methods
Search strategy
This review was registered on the PROSPERO database (CRD42014014486) and has been reported in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement.34 All relevant RCTs meeting the inclusion criteria were identified by a computer-aided search of the Medline, Cinahl, Academic Search Complete, AMED, SPORTDiscus, PsycINFO, Biomedical Reference Collection, PsycARTICLES, Embase, Scopus and Web of Science databases during August 2014 from the period of inception (figure 1). The search was restricted to include only trials that involved humans and were published in English.

Literature search flowchart. MDT, multidisciplinary team.
Two reviewers (MO and AH) conducted the electronic searches independently. The strategy had four components which were combined: (1) physiotherapy AND (2) individual/group AND (3) RCT and NOT (4) non-MSK conditions.
The exact search strings used are shown in figure 2.

Search terms.
Inclusion/exclusion criteria
Study design
Only reports of completed RCTs published in peer-reviewed journals were included.
Population
Studies with participants with MSK conditions (eg, low back, neck, hip, knee, ankle, shoulder, elbow or wrist pain) were included. Studies that involved participants with specific pathologies/conditions (eg, pregnancy, incontinence, ‘red flag’ disorders (eg, spinal cord compression/cauda equina, spinal cord injury, cancer, fracture) or neurological, cardiac, renal or respiratory, rheumatological conditions) were excluded.
Interventions
Studies were required to compare group and individual physiotherapy. Both were required to include exercise. Individual physiotherapy was eligible for inclusion whether or not it also involved a passive therapy. The addition, or absence, of other co-interventions (eg, manual therapy, education, relaxation) did not affect the eligibility of studies but, where present, these were noted. Studies were not eligible if they compared group physiotherapy with group physiotherapy or compared individual physiotherapy with individual physiotherapy. Similarly, if interventions contained a combination of group and individual components, they were excluded. Studies were also excluded if interventions had multidisciplinary team involvement (eg, psychology, occupational therapy or dietician). Studies that compared group or individual physiotherapy with a minimalist control group only (eg, simply providing education/advice booklets or a self-directed home exercise programme which did not involve regular tailoring and/or progression) were excluded. These were deemed irrelevant, as both group and individual physiotherapy incorporating exercise have established superiority over them.20 ,22 ,23 ,25 ,26 ,35
Clinical outcomes
Studies had to report results from one or more outcome measures in the domains of pain intensity and/or functional disability.
Study selection
Two authors (MO and AH) followed the same procedure for study selection and data extraction. After removal of duplicates, they independently screened the titles and abstracts of the articles found and excluded ineligible articles. If no abstract was available, or eligibility was not clear, full-text articles were retrieved to determine inclusion or exclusion. The full-text version of an article was obtained if the title and abstract seemed to fulfil the inclusion criteria or if the eligibility of the study was unclear. Disagreements on study eligibility were resolved in a consensus meeting with two other authors (KM and KO). Original study authors were emailed, where necessary, to provide clarity on interventions or methodology. The reference lists of the selected articles were also manually searched for any further relevant articles.
Quality assessment
Methodological quality of the included studies was rated independently by two assessors (MO and AH) using the reliable36 and valid37 PEDro scale. The scale has 11 criteria, 10 of which are scored. When it was unclear whether a study met a criterion, or if no clear information about the item was given, the author of the original study was contacted for clarity. If the two assessors disagreed about an individual study, a consensus decision was reached. Each item was scored as ‘yes’ if it fulfilled the criteria, and ‘no’ when there was a risk of bias or a lack of clarity. The quality was classified as ‘high’ (≥6/10), ‘fair’ (≥4–6/10) or ‘poor’ (<4/10), according to PEDro scores38 to aid interpretation of study quality if the findings were inconsistent. The quality assessment scores for all studies are shown in online supplementary file 1.
Supplementary file 1
Data extraction
Data for each study were extracted and cross-checked by two authors (MO and AH). The following data were extracted: (1) characteristics of the participants: sample size, sex, age, area of pain; (2) inclusion criteria; (3) characteristics of the interventions: the type, frequency and duration of group and individual physiotherapy and (4) characteristics of the outcomes: pain and disability outcome measures, follow-up times. Similarities in the outcome measures used, the MSK conditions involved, the participants included and the physiotherapy interventions examined allowed for pooled analysis of the data. The data extracted from all studies are shown in online supplementary file 2.
Supplementary file 2
Data analysis
Data analysis was performed by a statistician (HP). The effects of group and individual physiotherapy incorporating exercise were compared using meta-analyses. The primary outcomes of interest were pain intensity and functional disability. Pain intensity was measured using the Visual Analogue Scale (VAS) or Numerical Rating Scale. The reported pain intensity scores were converted to a 0–100 point scale, where necessary, and a mean difference (MD) was computed. The analysis of functional disability required a standardised MD (SMD) to be computed as studies used a number of different measures to report disability, including the Roland–Morris Disability Questionnaire, Oswestry Disability Index, Northwick Park Neck Pain Questionnaire, Neck Disability Index and Western Ontario and McMaster Universities Arthritis Index (WOMAC).
Analyses were carried out at three assessment points: (1) short-term follow-up (up to 3 months); (2) medium-term follow-up (>3 months and <12 months) and (3) long-term follow-up (≥12 months). The meta-analysis analysed all the studies together. Subgroup analyses were also conducted by testing differences in pain and disability between neck pain, LBP and knee pain separately. A sensitivity analysis was conducted to determine whether limiting the analysis to high-quality studies changed the results.
A random-effects model was selected for all analyses a priori,39 and heterogeneity between treatment studies was reported using the I2 statistic. In studies where multiple contrasts were examined (eg, individual physiotherapy vs group physiotherapy A vs group physiotherapy B), the sample size in the shared comparison was halved in order to avoid double counting of participants in the analyses.
In studies where SDs were not reported at follow-up times, the baseline SD was used in the analysis. Where data were summarised using median and IQR values, the mean was approximated using the median and the width of the IQR was used as an approximation of 1.35 times the SD.39 Pooled 95% CIs were computed for MD and SMD, and CIs excluding zero were considered statistically significant. Clinical relevance was determined using the following effect-size classifications: (1) small (not clinically relevant): MD<10 (ie, <10% of the 100 mm VAS), SMD (Cohen's d) of 0.2; (2) medium: MD<20, SMD (Cohen's d) of 0.5; (3) large: MD≥20, SMD (Cohen's d) of 0.8.40 Heterogeneity between studies was assessed visually from the Forest plots, using formal Q-tests (χ2 test statistic and p value) and the I2 statistic. Substantial heterogeneity was determined using the cut-off point I2≥50%. All analyses were conducted in Review Manager 5.2.
Results
Literature search
Study identification is summarised in figure 1. The literature search of databases yielded 14 579 potentially relevant articles. Duplicates (7896) were removed and 6683 titles and abstracts were scanned. Fifty-seven full-text studies were retrieved, with 43 studies being excluded as ineligible. Searching the reference lists of these articles did not yield any further articles. The major reasons for exclusion were multidisciplinary team involvement in interventions, mixed group and individual physiotherapy being provided, no exercise being included in the physiotherapy, lack of individual or group physiotherapy and the individual intervention being minimal (eg, solely providing an information leaflet). Fourteen studies met the selection criteria. Four authors were emailed to obtain further information for clarification and two of them replied.
Quality assessment
The quality assessment scores are shown in online supplementary file 1. Thirteen studies were rated as ‘high quality’ and one as ‘fair quality’ according to the PEDro scale. Four studies were awarded a score of 8/1028 ,41–43 and one a score of 4/10.44 Common methodological limitations included lack of therapist and patient blinding, which would be practically unavoidable in trials of exercise therapy, as well as large loss to follow-up.
Population
Studies involved participants with LBP43–49 (n=7), neck pain42 ,50–52 (n=4), knee pain41 ,53 (n=2) and shoulder pain28 (n=1). The majority of participants had chronic pain (ie, >3 months). The sample sizes of the included studies ranged from 12 to 249. The mean (SD) age across all studies was 48 (12) years.
Intervention characteristics
The characteristics of the various group and individual physiotherapy interventions are shown in online supplementary file 2. Group physiotherapy mainly consisted of exercise, education and relaxation, whereas individual physiotherapy mainly consisted of exercise, education and passive modalities. Only four studies41 ,48 ,52 ,53 had a group intervention of exercise alone. Only two studies48 ,50 had an individual intervention consisting of exercise alone. Only one study48 had both a group and individual intervention providing exercise alone.
Clinical outcome measures
All studies reported a disability measure. The shoulder pain study28 did not report a pain intensity measure. Ten of the other 13 studies used the Numerical Rating Scale or VAS to measure pain intensity. Three common disability measures (Oswestry Disability Index, Neck Disability Index and Roland–Morris Disability Questionnaire) were used in nine studies. The specific pain intensity and disability measures for each individual study are shown in online supplementary file 2.
Meta-analysis studies
Twelve studies were included in the meta-analysis of pain and disability. One study on LBP43 was excluded as there were significant differences in baseline disability between the groups. The one study on shoulder pain28 was excluded as the authors were unable to provide the means and SDs required for analysis. Subgroup analyses were conducted by testing pooled differences in pain and disability between LBP, neck pain and knee pain at each follow-up time; no significant differences were found (p>0.05). We conducted a sensitivity analysis limited to the 11 ‘high-quality’ studies and no significant differences were found for pain or disability (p>0.05).
Effects of individual versus group physiotherapy on pain intensity
No statistically significant difference was found for pain intensity between individual and group physiotherapy including exercise at short-term (12 studies, n=480, MD=−0.39, 95% CI −3.07 to 2.28) and medium-term (seven studies, n=361, MD=−1.41, 95% CI −4.48 to 1.66) follow-up (figure 3).

Effect of individual versus group physiotherapy on pain. NRS, numerical rating scale.
A small, yet statistically significant, difference was found for pain intensity between individual and group physiotherapy including exercise at long-term (seven studies, n=307, MD=−3.51, 95% CI −6.14 to −0.88) follow-up, favouring group interventions (figure 3).
Effects of individual versus group physiotherapy on disability
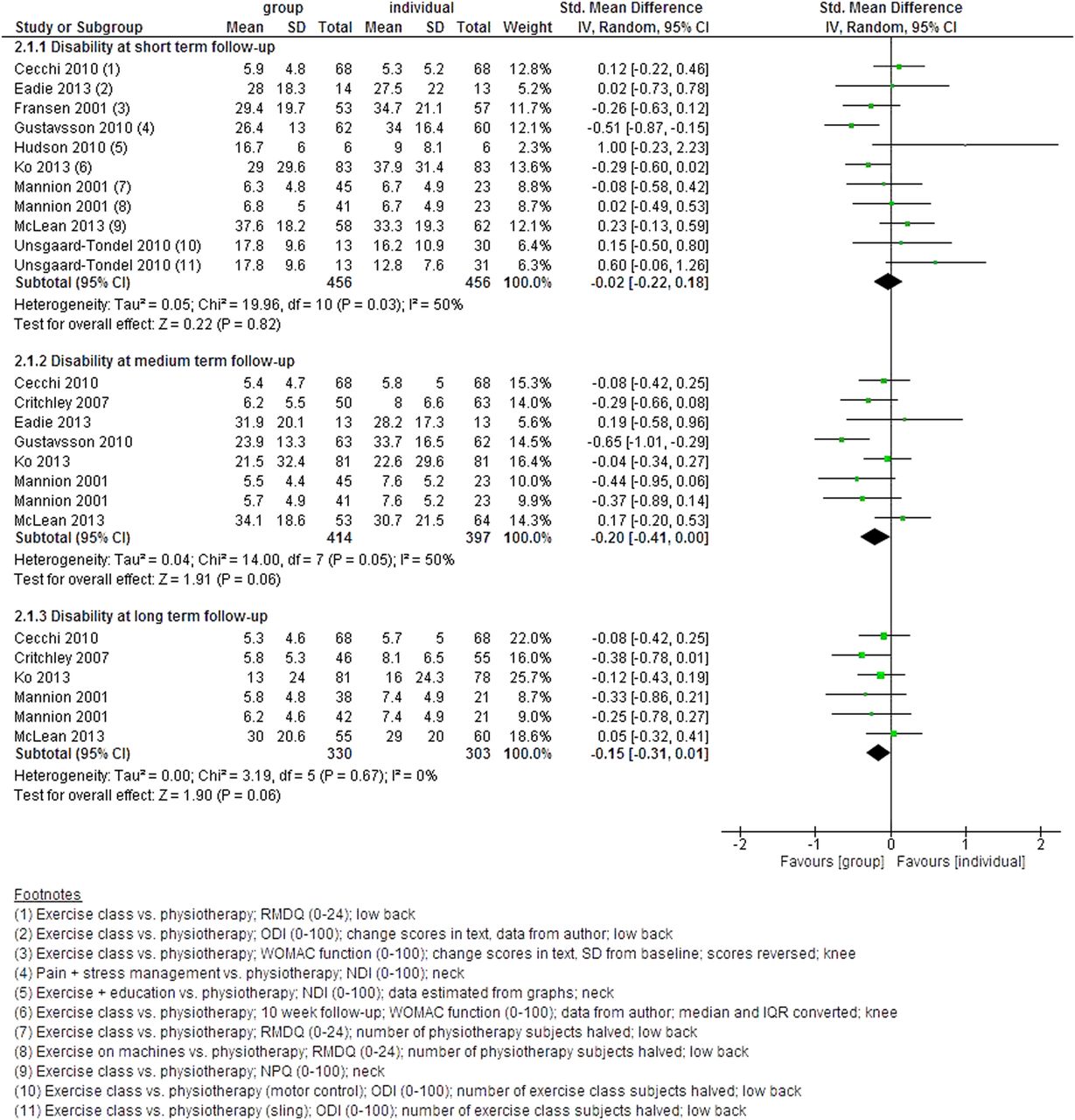
No statistically significant difference was found for disability between individual and group physiotherapy including exercise at short-term (12 studies, n=480, MD=−0.02, 95% CI −0.21 to 0.16) follow-up (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of individual versus group physiotherapy on disability. NDI, Neck Disability Index; ODI, Oswestry Disability Index; RMDQ, Roland–Morris Disability Questionnaire; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
A small, yet statistically significant, difference was found for disability between individual and group physiotherapy including exercise at medium-term (eight studies, n=414, MD=−0.20, 95% CI −0.41 to 0.00) and long-term (seven studies, n=343, MD=−0.14, 95% CI −0.30 to 0.01) follow-up, favouring group interventions (figure 4).
Studies excluded from meta-analysis
The one excluded study on LBP43 found no statistically significant differences for pain and disability between individual and group physiotherapy including exercise at all follow-up periods. The one excluded study on shoulder pain28 found a statistically significant difference for pain and disability between individual and group physiotherapy including exercise at all follow-up periods, favouring group interventions.
Discussion
Main findings
For pain and disability, no clinically significant differences were found between group and individual physiotherapy including exercise. For some of the comparisons performed, particularly in the long-term, group interventions were more effective, but these differences were small and not clinically relevant.
The small and similar effects yielded by the two modes of physiotherapy support choosing more cost-efficient group interventions,46 provided that they are feasible and acceptable to patients. Our review extends previous findings14 ,54 ,55 that show no superiority for one type of exercise over another in the management of MSK conditions. Our findings are also consistent with those of a recent review,33 where self-management that included group physiotherapy was as effective as individual physiotherapy and medical management in those with LBP and osteoarthritis.
Why is individual physiotherapy including exercise not better than group physiotherapy?
Many clinicians may be surprised that individual physiotherapy was not better than group physiotherapy. This raises the question of whether we failed to find a ‘real’ difference or whether there really is no difference. Is it possible that group programmes provide a similar but cheaper outcome? We provide several avenues for consideration.
One potential explanation for the lack of superiority of individual physiotherapy may be that the group physiotherapy interventions seem to have spent more time on exercise and education. Individual physiotherapy in 12 of the 14 included studies in this review involved other non-exercise-based, passive therapies which have limited evidence of effectiveness.9 ,10 ,56 ,57 Only two individual physiotherapy interventions48 ,50 involved exercise only. Individual physiotherapy involving passive therapies may not spend enough time on exercise in comparison with groups which have no passive therapies. Since dose and content of an intervention can influence outcome,58 we speculate that group interventions may benefit from focusing mainly on evidence-based treatment, such as exercise and education, and excluding other passive therapies (eg, modalities, manual therapy) with limited evidence of efficacy.28
A second possible explanation for the lack of additional benefit from individual physiotherapy might be that the exercise provided was not tailored to the individual needs of patients. For example, the exercises used in most studies did not appear to take into account the baseline exercise capacity of people with MSK conditions. This is not in line with evidence advocating the use of the FITT (Frequency, Intensity, Time, Type) principle for exercise.17 ,59 In addition, patient needs might vary according to their MSK condition, with differences in strength, endurance, flexibility, sensory motor control, muscle recruitment, proprioception and movement patterns. Furthermore, most participants received the same dose and type of exercise. In addition, the exercise did not progress or was completed in such a way that all participants reached the same level, at the same time, with no account taken of variations in individual needs, pain, disability, progress or goals. These factors may explain why using a generic exercise programme is equally effective for a group as for an individual.
A third explanation for the lack of difference might result from not categorising MSK conditions using different risk profiles or clinical presentations to guide treatment.60–62 MSK conditions are biopsychosocial disorders, involving not just pathoanatomical (eg, knee osteoarthritis) and physical factors (eg, deconditioning), but also cognitive (eg, unhelpful beliefs), psychological (eg, depression), lifestyle (eg, physical inactivity, insomnia, stress) and social (eg, work status) factors.
Exercise can influence a wide range of these factors, including mood,63 catastrophising,64 fear65 and self-efficacy.66 However, there was no evidence that exercise interventions in the included studies aimed at dealing with cognitive, psychological and social factors. Furthermore, since few studies in this review measured non-physical factors, detailed analysis of the mechanisms involved in reducing pain in these studies is not possible. Given the multidimensional nature of MSK conditions, it is possible that exercise programmes that deal primarily with only one contributory domain (eg, physical factors) will have small effects.
Possibly, some patients may benefit from more emphasis on some contributory factors than others (eg, exercise prescription vs interventions to deal with depression or sleep, etc). This could be facilitated by the use of screening tools and training. For instance, some studies have shown that for patients with LBP, matching the type and amount of treatment to the perceived needs of the patient improves outcomes.61 ,66 ,67 These studies61 ,66 ,67 included more than just physical rehabilitation, reflecting the biopsychosocial nature of MSK conditions. It should be noted, however, that recent attempts to tailor LBP rehabilitation to individual patients, which deal only with physical factors, have failed to show any benefit of individualisation.29 ,68 This suggests that rehabilitation for MSK conditions may need to be both biopsychosocial and tailored to the individual needs of patients. Nevertheless, the possibility that MSK conditions will remain highly resistant to treatment in some patients, even when an individualised biopsychosocial approach is used, cannot be discounted.
Finally, the potential for better social interaction and social support in groups could be considered as an advantage of group-based rehabilitation.18 ,27
Future research and clinical implications
Based on these findings, if exercise is to be delivered by physiotherapists in the management of MSK conditions, group interventions should be considered owing to the lower healthcare costs. Although a cost–benefit analysis was not the primary aim of this review, the one study46 carrying out an economic evaluation showed no differences in pain and disability between group and individual physiotherapy, but modest cost savings with a group intervention, in line with other literature.69 ,70
If exercise delivered through individual physiotherapy is to show clinical and cost-effectiveness, the exercise may need to be (i) tailored to the exercise capacity and individual needs (eg, strength, flexibility, proprioception and movement patterns) of each patient and/or (ii) deal with the specific biopsychosocial needs of a patient. Furthermore, given the limited long-term effectiveness of passive therapies in MSK conditions,9 ,10 ,56 ,57 individual and group physiotherapy should perhaps eschew these treatments and place greater emphasis on evidence-based treatments (eg, exercise). Providing non-evidence-based passive treatments might reduce the priority a patient places on exercise. As exercise may work via multiple mechanisms, future RCTs should also include analysis to better understand which patients would respond best to exercise, and the mechanisms underlying improvements in pain and disability after exercise. In addition, details of the type of education that accompanies exercise are often not given. As effectiveness depends on the type of education provided,71 ,72 future RCTs should investigate whether supplementing exercise with education which highlights the safety and benefits of activity, together with the multidimensional nature of MSK conditions, results in better outcomes. Furthermore, certain people might be more suited to a group or individual intervention. For example, people with more complex pain disorders or language difficulties might be better suited to an individualised programme.46 These factors and patient preference should be considered when choosing the type of intervention.
Limitations
We acknowledge a number of limitations. (1) Only RCTs published in English were included, and relevant studies in other languages might have been excluded. (2) Both group and individual interventions usually included other co-interventions, with some individual interventions including education and passive modalities (eg, manual therapy), and some group interventions including education and relaxation. All but one study48 included other co-interventions with exercise in either the group or individual arm, so determining the independent effect of exercise is difficult. However, using a multimodal approach to complement exercise is standard physiotherapy practice. Furthermore, the one study48 that included exercise only in both arms, showed no differences between group and individual physiotherapy and underlines our overall conclusion. (3) As only RCTs were included, the very nature of these studies might have contributed to exercise being standardised in a manner that does not always reflect practice. (4) The studies differed in the amount of exercise provided, with some group physiotherapy interventions providing more exercise than the individual physiotherapy comparison. (5) Review procedures have evolved since we submitted the original review protocol. We used a summary score out of 10 and specific cut-off values to distinguish between high- and low-quality studies. With this system a study that fulfils any six of the 10 criteria is deemed high quality. This approach has limitations, however, as meta-epidemiological evidence suggests that failure in any one of the 10 criteria might alone explain a small positive effect on a subjective self-reported outcome. (6) Some study authors did not reply to emails asking about their study interventions and methodology, which might have resulted in errors in quality assessment and inclusion of some studies. However, if criteria were deemed unclear, they were scored accordingly on the PEDro critical appraisal measure. Furthermore, we performed a sensitivity analysis and a consistent study selection procedure, based on strict inclusion/exclusion criteria.
Conclusion
For pain and disability, no clinically significant differences were found between group and individual physiotherapy including exercise. Given the lower healthcare costs of group-based interventions, group physiotherapy for MSK conditions may need to be considered more often.
What are the findings?
Only small, clinically irrelevant differences were found between group and individual physiotherapy incorporating exercise and, where present, these differences favoured group interventions.
Physiotherapy incorporating exercise for musculoskeletal pain delivered on an individual basis is no better than the equivalent treatment in a group. Future research should investigate the effect of individual physiotherapy involving exercise that better matches an individual's capacity and needs, and/or considers other barriers to recovery from pain across the biopsychosocial spectrum.
How might it impact on clinical practice in the future?
Group interventions may need to be considered more often, given their similar effectiveness and lower healthcare costs.
References
Footnotes
Twitter Follow Mary O'Keeffe at @MaryOKeeffe1990
Contributors MO, KO, KM and AH were involved in conception and design. MO and AH independently performed the search and reviewed the literature; carried out the data extraction; rated the quality of the studies. HP performed the meta-analysis. All authors were involved in data analysis and interpretation, and in preparing the manuscript for publication.
Funding MO is supported by an Irish Research Council postgraduate scholarship.
Competing interests KO receives income from delivering educational courses and workshops on the use of an individualised, multidimensional approach to managing chronic low back pain. KM has received funding to conduct research into the use of a group exercise approach for people with shoulder pain.
Provenance and peer review Not commissioned; externally peer reviewed.