Article Text

Abstract
Objective To investigate the effect of FIFA injury prevention programmes in football (FIFA 11 and FIFA 11+).
Design Systematic review and meta-analysis.
Eligibility criteria for selecting studies Randomised controlled trials comparing the FIFA injury prevention programmes with a control (no or sham intervention) among football players.
Data sources MEDLINE via PubMed, EMBASE via OVID, CINAHL via Ebsco, Web of Science, SportDiscus and Cochrane Central Register of Controlled Trials, from 2004 to 14 March 2016.
Results 6 cluster-randomised controlled trials had assessed the effect of FIFA injury prevention programmes compared with controls on the overall football injury incidence in recreational/subelite football. These studies included 2 specific exercise-based injury prevention programmes: FIFA 11 (2 studies) and FIFA 11+ (4 studies). The primary analysis showed a reduction in the overall injury risk ratio of 0.75 (95% CI 0.57 to 0.98), p=0.04, in favour of the FIFA injury prevention programmes. Secondary analyses revealed that when pooling the 4 studies applying the FIFA 11+ prevention programme, a reduction in the overall injury risk ratio (incidence rate ratio (IRR) 0.61; 95% CI 0.48 to 0.77, p<0.001) was present in favour of the FIFA 11+ prevention programme. No reduction was present when pooling the 2 studies including the FIFA 11 prevention programme (IRR 0.99; 95% CI 0.80 to 1.23, p=0.940).
Conclusions An injury-preventing effect of the FIFA injury prevention programmes compared with controls was shown in football. This effect was induced by the FIFA 11+ prevention programme which has a substantial injury-preventing effect by reducing football injuries by 39%, whereas a preventive effect of the FIFA 11 prevention programme could not be documented.
Trial registration number PROSPERO CRD42015024120.
- Football
- Injury prevention
- Exercises
Statistics from Altmetric.com
Introduction
FIFA estimates that more than one-quarter of a billion people around the world regularly participate in football (soccer).1 Football has been recognised, together with running, as one of the most promising sports and leisure time activities to improve health.2 Football improves cardiovascular and metabolic health,2 and diminishes risk factors for lifestyle diseases, such as diabetes and hypertension.3 However, football also includes an inherent risk of injury,4 ,5 which is why injury prevention in football is crucial.6
European data show that millions of sports-related injuries occur each year and require medical attention and of all sports-related injuries seen in general practice, about one in four are football-related.7 Furthermore, 5.8 million people each year are treated at hospitals in Europe due to injuries associated with sports.8 Team ball sports account for almost half of all hospital-related sports injury treatment—and football accounts for two-third of these.8 Since 2004, FIFA has focused on strategies for injury prevention by introducing FIFA Medical Assessment and Research Centre (F-MARC) prevention programmes, known as the FIFA injury prevention programmes, and assessed their effects on football injury rates.9 These programmes include specific strengthening, balancing and jumping/landing exercises, and are to be included during a structured warm-up session. The goal of the programmes is to improve strength, balance and jumping/landing ability, which may lead to injury reduction.10–12 Two variations of such programmes have been developed and provided by FIFA, the FIFA 11 and the FIFA 11+ prevention programme.10 The FIFA 11+ is a revised version of the original FIFA 11 prevention programme.10–12 The FIFA 11+ includes similar key exercises as the FIFA 11 with minor additions, including a more dynamic warm-up and a more specific progression model for the included exercises to allow for more variation and optimising physical improvement (figure 1).10–12 The programmes have been tested in different football cohorts and individual studies, but with varying effects on injury estimates.10 Findings of no differences in injury estimates from single studies cannot, however, be considered confirmation of no effect.10 This may simply be due to insufficient power to detect reductions in injury rates of <40%, which the first FIFA injury prevention programme trial was powered to detect.12 Pooling data from individual studies into a meta-analysis offers an opportunity to increase statistical power and test whether the FIFA injury prevention programmes are associated with injury reduction, as originally hypothesised in the initial studies where FIFA was involved.10–12

Specific characteristics and differences of the FIFA 11 prevention programme and the FIFA 11+prevention programme. Similar types of grey shade indicate similar types of exercise.
Since the specific strategic goal of the F-MARC since 2009 has been proclaimed to be: ‘to prevent football injuries and to promote football as a health-enhancing leisure activity, improving social behaviour’,6 ,9 ,13 investigating the effect of the FIFA injury prevention programmes seems more timely and relevant than ever. Until now, only narrative reviews and systematic reviews including results from randomised and observational studies have been published.6 ,10 ,14 We therefore carried out a comprehensive and up-to-date systematic review and meta-analysis of the effects of the FIFA injury prevention programmes in football, including only randomised controlled trials, to provide level 1 evidence in this field.
Methods
We used the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) as a guideline for this study.15 The study was registered at PROSPERO (ID=CRD42015024120), and a publicly available comprehensive study protocol including data extraction forms was uploaded at the following website: http://vbn.aau.dk/files/229186677/The_effect_of_the_FIFA_11_prevention_programmes_on_the_overall_injury_rate_in_football_a_systematic_review_and_meta_analysis_version1_1.pdf
Deviations from study registration and study protocol
Agreement by raters on risk of bias decisions for the included randomised controlled studies was calculated as a percentage of agreement and κ values, and included in the results. Since the secondary analysis concerning type of programme showed that only the FIFA 11+ prevention programme was effective in reducing injuries, all secondary outcomes concerning lower limb, hamstring, knee and ankle injuries were only analysed in relation to this programme. Furthermore, a post hoc analysis on hip/groin injury in relation to this programme was also included. Preplanned secondary analyses on the incidence rate ratio (IRR) in the following subgroups: gender (male and female), and mean age groups (youth (<19 years), seniors (19–30 years), old girls/boys (31–39 years) and veterans (>39 years)) were not conducted, as the included studies did not allow making meaningful comparisons with only six studies, where studies with male (n=3) and female participants (n=3) significantly differed in the age group they targeted. The predefined secondary analysis of compliance at team level was not performed as all team-level data could not be obtained from the corresponding authors of the included studies. Instead, the preplanned analysis of the association between prevention programme compliance and injury incidence was further supported by a post hoc analysis of the association between prevention programme compliance and the overall injury IRR from each study to accommodate for the risk of substantial variance in injury incidence between studies due to other factors than the FIFA injury prevention programmes.
Eligibility criteria
We included only randomised or cluster-randomised controlled trials comparing the FIFA injury prevention programmes with a control (no or sham intervention) among football players. To be included, studies were required to fulfil the following criteria: (1) the full-text paper published in a peer-reviewed journal was available; (2) the study contained original data from a randomised controlled or a cluster-randomised trial; (3) the preventive effect of FIFA 11 or the FIFA 11+ prevention programme was evaluated; (4) only football players were included; and (5) football injury was an outcome. For the assessment of harms (adverse events), we also included all other original studies or reports including practical execution of FIFA injury prevention programmes in football.
Literature search and study selection
We systematically searched the following bibliographic databases: MEDLINE via PubMed, EMBASE via OVID, CINAHL via Ebsco, Web of Science, SportDiscus and Cochrane Central Register of Controlled Trials, from 2004 to 14 March 2016, as the FIFA injury prevention programmes were initiated and implemented from 2004 to 2005.9 ,13 A hand search of the reference lists of relevant articles was also conducted for other potentially relevant references, and F-MARC was contacted to verify if any important FIFA 11 or FIFA 11+ studies/publications did not appear from the search. No restriction on language was included in the search. The following search strategy was tested and found to be the most valid and efficient across databases, and was applied in all the databases aforementioned: (fifa OR f-marc OR fmarc OR prevention program* OR warm-up program* OR warmup program* OR the11) AND (football OR foot ball OR soccer). Possible relevant studies, identified by titles and abstracts from the search, were downloaded into Reference Manager V.14 (Thomson Reuters, USA) and duplicates were removed. Two authors (KT and KKK) independently performed the selection of studies based on the title and abstract provided by the bibliographic databases. This was followed by full-text evaluation of the selected studies from the first selection step. Disagreement between the two reviewers was solved by discussion. If consensus was not achieved, a third reviewer (EMB) was involved.
Data extraction
Two reviewers (EE and MBC) independently extracted data using a specifically designed standardised data extracting form (see study protocol), and afterwards the reviewers compared the extracted data for consistency. All inconsistencies between the two forms were resolved by discussion between the two data extractors. Any disagreement between the data extractors after the initial discussion related to inconsistencies between the two individual data extractions was to be solved by involving a third person (EMB). General study information, participants and intervention characteristics, compliance, adverse events, withdrawals and outcome measures were extracted. Where data were not available from tables or the results section, the authors of the study in question were contacted by email, with one reminder after 2 weeks, if they did not respond to the first email. Data obtained from authors not available from the articles can be seen in table 1, indicated by asterisks.
Summary of included RCT studies investigating the effect of FIFA injury prevention programmes
Primary outcome
Effect of FIFA injury prevention programmes on football injury rates
The primary outcome was overall injury incidence defined as the total number of injuries per 1000 hours of football exposure. This included all injuries (overuse and traumatic) sustained during the study period in training and match play.
Secondary outcomes
Effect of FIFA injury prevention programmes on football injury rates
Secondary outcomes were lower limb injury incidence and region-specific injury incidence for hamstring, hip/groin, knee and ankle, all defined as the number of injuries per 1000 hours of football exposure, respectively. This included all injuries (overuse and traumatic) in each category sustained during the study period in training and match play.
Compliance with the FIFA injury prevention programmes and its association with football injury rates
In the present study, compliance with the intervention was defined and estimated as the number of FIFA injury prevention programme sessions performed at team level during the intervention period divided by the length of the intervention period in months. The mean compliance for each study included in the primary analysis was estimated at team level from data available from included trials. For the same trials, the compliance for each individual team was estimated from similar data, at team level, obtained directly from the authors of the original trials. Accordingly, data at team level were obtained on: total number of injuries; total exposure time (hours); number of FIFA injury prevention programme sessions performed, and the duration of the FIFA injury prevention programme exercise period (months). The first author of this systematic review (KT) contacted corresponding authors of cluster-randomised studies included in the primary analysis concerning these compliance/injury data, and asked them to provide this information in a prespecified data extraction form on compliance and injury rates at team level (study protocol).
Harms resulting from the execution of the FIFA injury prevention programmes
The number and type(s) of adverse effects resulting from the actual execution of the FIFA injury prevention programmes (experienced while performing the prevention exercises) were obtained from all identifiable studies including practical execution of these programmes.
Synthesis of results
Effect of FIFA injury prevention programmes on football injury rates
For the primary analysis on the effects of the FIFA injury prevention programmes on overall injury rates, we calculated the pooled overall injury incidence for intervention and groups separately using data on injuries and exposure from all included cluster-randomised studies. If the data used to calculate the injury incidence were not available in the published article, the first author (KT) of the systematic review requested the missing data from the author(s). All cluster-randomised trials were adjusted for cluster effect in all pooled analyses. Since only one included study11 reported cluster-adjusted estimates, we used the intracluster correlation coefficient (ICC) from their trial on all trials to adjust for a potential cluster effect by calculating the inflation factor (IF). The equation for cluster adjustment is IF=1+(n−1)ρ, where ρ is the ICC, n the average cluster size and IF the inflation factor.16 ,17 Effective sample size was then calculated by dividing the number of injuries and exposure hours by IF, as described in the Cochrane Handbook for Systematic Review of Interventions, V.5.1 (part 3: 16.3.4).17
For the primary and secondary analyses including all randomised studies using FIFA injury prevention programmes, the overall injury IRR and 95% CIs were estimated as the relative effect size. In the secondary analyses on body region-specific injury rates, we only included studies using the FIFA 11+ prevention programme, and IRR and 95% CIs were estimated as the relative effect size using the extracted and pooled injury data from the following body regions: lower limb, hamstring, hip/groin, knee, and ankle, analysed in five separate analyses, one for each body region.
Stata V.12 (StataCorp LP) was used to perform the meta-analysis and calculate the pooled estimates. A forest plot is presented to allow for visual comparisons between studies. The level of statistical heterogeneity for pooled data was established using the χ2 and I2 statistics. The χ2 and I2 statistics describe heterogeneity or homogeneity of the comparisons with p<0.05 indicating a significant heterogeneity.18 The Mantel-Haenszel19 ,20 random-effects method was selected for all analyses.
Compliance with the FIFA injury prevention programmes and its relation to football injury rates
To assess the association between prevention programme compliance and effect on injury incidence, we performed two random-effects meta-regression analyses using Stata. One meta-regression was performed using the injury incidence in the intervention group as the outcome and the average team compliance in each study as the explanatory variable. The post hoc meta-regression was performed to investigate the association between IRR from each study as the outcome and the average team compliance from each study as the explanatory variable.
Harms resulting from the execution of the FIFA injury prevention programmes
Adverse effect/harms of applying an FIFA injury prevention programme was given as number and type(s) of adverse effects resulting from the actual execution of the FIFA injury prevention programmes (experienced while performing the prevention exercises) relative to the total number of players performing the FIFA injury prevention programmes in the included studies.
Risk of bias assessment
The included cluster-randomised studies were assessed for risk of bias by two independent raters (EE and MBC) using the Cochrane Collaboration's tool for assessing risk of bias in randomised controlled trials.17 Each trial was evaluated across seven domains of bias, including one or more items that were appraised in two parts. First, the relevant trials' characteristics related to the item were summarised. Second, each bias domain was judged as high or low risk of bias according to its possible effect on the results of the trial. When the possible effect was unknown or insufficient detail was reported, the item was judged as unclear. All the above concerning risk of bias followed the description outlined in the Cochrane Handbook for Systematic Review of Interventions, V.5.1 (part 2: 8.5.1).17 Since only cluster-randomised trials were included, particular types of bias were assessed in the ‘other bias’ domain for all studies, according to how to assess risk of bias in cluster-randomised trials following the recommendations in the Cochrane Handbook for Systematic Review of Interventions, V.5.1 (part 3: 16.3.2).17 Any disagreements between ratings were resolved by discussion between the raters. Consultation with a third party (EMB) was to be used if disagreements still persisted after this discussion. An assessment of the methodological quality was not performed, because no evidence for such appraisals and judgements exists as to why such an assessment could be potentially misleading.17
High risk of bias is to be expected from the domains concerning blinding of participants and researchers (performance bias), and blinding of outcome assessment (detection bias). In prevention studies using active exercise programmes such as the FIFA injury prevention programmes, it is very difficult to blind the participants to the intervention. Furthermore, it is impossible to blind the outcome assessment as the reporting of injuries is self-reported by definition. Risk of bias assessment was therefore followed as recommended in the Cochrane Handbook for Systematic Review of Interventions, V.5.1 (part 2: 8.5.1 and part 3: 16.3.2),17 but not considered for sensitivity analyses in the final evaluation of the primary or the secondary outcomes. Intertester reliability of ratings was calculated and presented using percentage of agreement and unweighted κ statistics.
Results
The literature search yielded 2400 studies after removal of duplicates. Out of these, 51 were considered for inclusion after review of title and abstract. Following a full-text review, 19 reports were excluded due to 11 not qualifying as full-text articles, and 8 because they did not include football players performing the FIFA injury prevention programmes. This left 32 studies investigating the FIFA injury prevention programmes, including potential harms.9 ,11 ,12 ,21–49 Out of these, 26 studies were not cluster-randomised trials or randomised controlled trials on FIFA injury prevention programmes, leaving 6 studies11 ,12 ,21 ,33 ,40 ,43 for the assessment of the effect of the FIFA injury prevention programmes on football injury rates in players playing at the recreational/subelite level (figure 2). None of these six studies included players at the elite level. Two studies involved the FIFA 11 prevention programme,12 ,21 and four studies involved the FIFA 11+ prevention programme.11 ,33 ,40 ,43
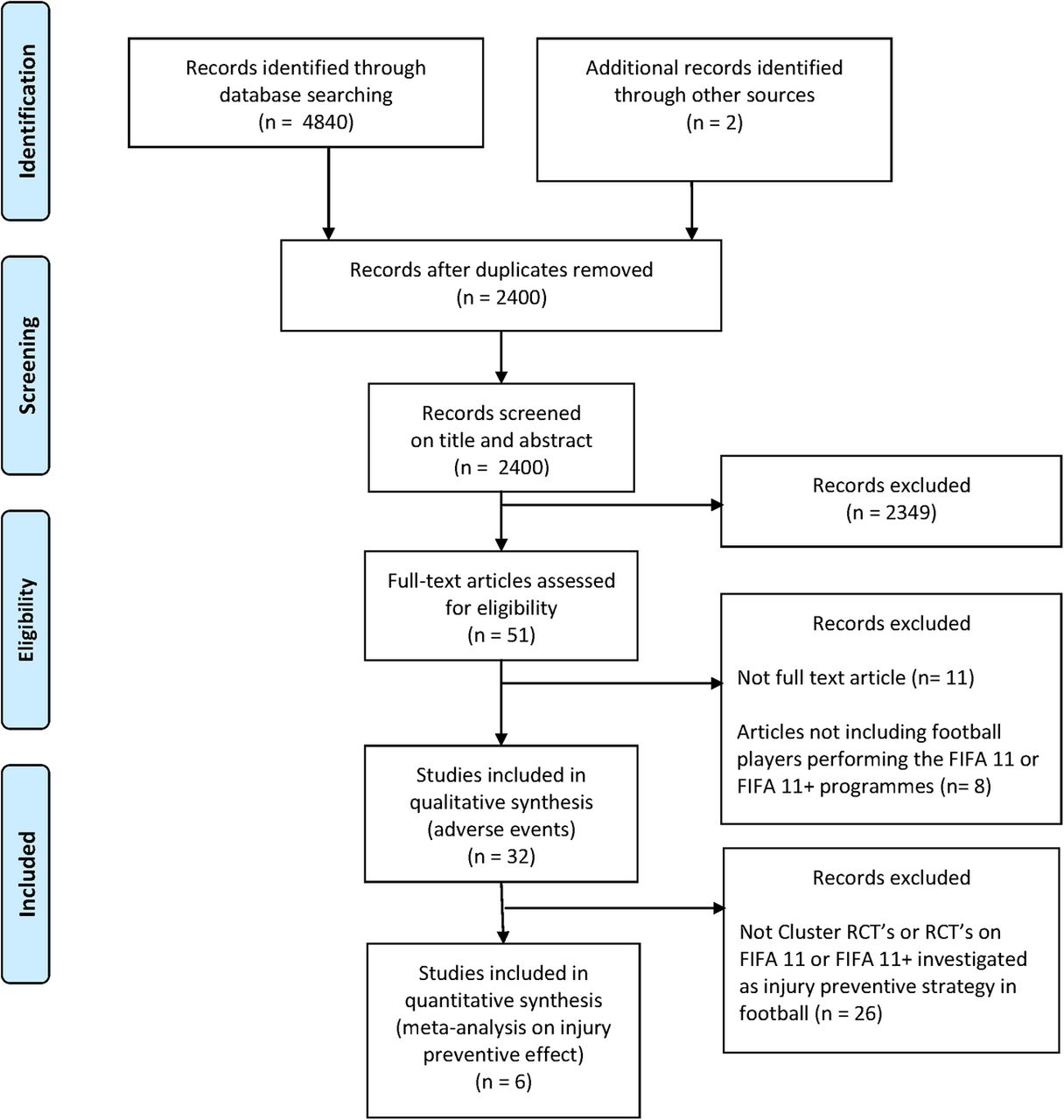
Flow chart of study selection for the analysis of the effects of the FIFA injury prevention programmes on injury prevention, and possible adverse events related to these programmes. RCT, randomised controlled trial.
Effect of FIFA injury prevention programmes on football injury rates
The six included randomised controlled trials had randomly allocated 186 teams (3806 football players) to FIFA injury prevention programmes, and 180 teams (3645 players) to the control group (no programme).
Study characteristics
The mean age of players in the individual trials ranged from 15 to 45 years. The follow-up time for the trials included periods of 5–9 months (table 1).
Synthesis of results
By pooling data of 6574 individuals playing football at the recreational/subelite level, 510.055 exposure hours and 2454 overall injuries were collected from the six included randomised controlled trials. The pooled total injury incidence was 3.99 injuries per 1000 hours of exposure for the intervention group and 5.57 injuries per 1000 hours of exposure for the control group.
In the primary analysis, and for the primary outcome (overall injury rate), the pooled results showed a 25% overall injury reduction per 1000 hours of exposure in the FIFA injury prevention programmes (FIFA 11 and FIFA 11+) group compared with the control group (IRR 0.75; 95% CI 0.57 to 0.98, p=0.036; figure 3). There was significant heterogeneity in this analysis (I2=68.9%, p=0.007).

Primary analysis of overall injury rates in FIFA injury prevention programmes compared with control intervention. IRR, incidence rate ratio.
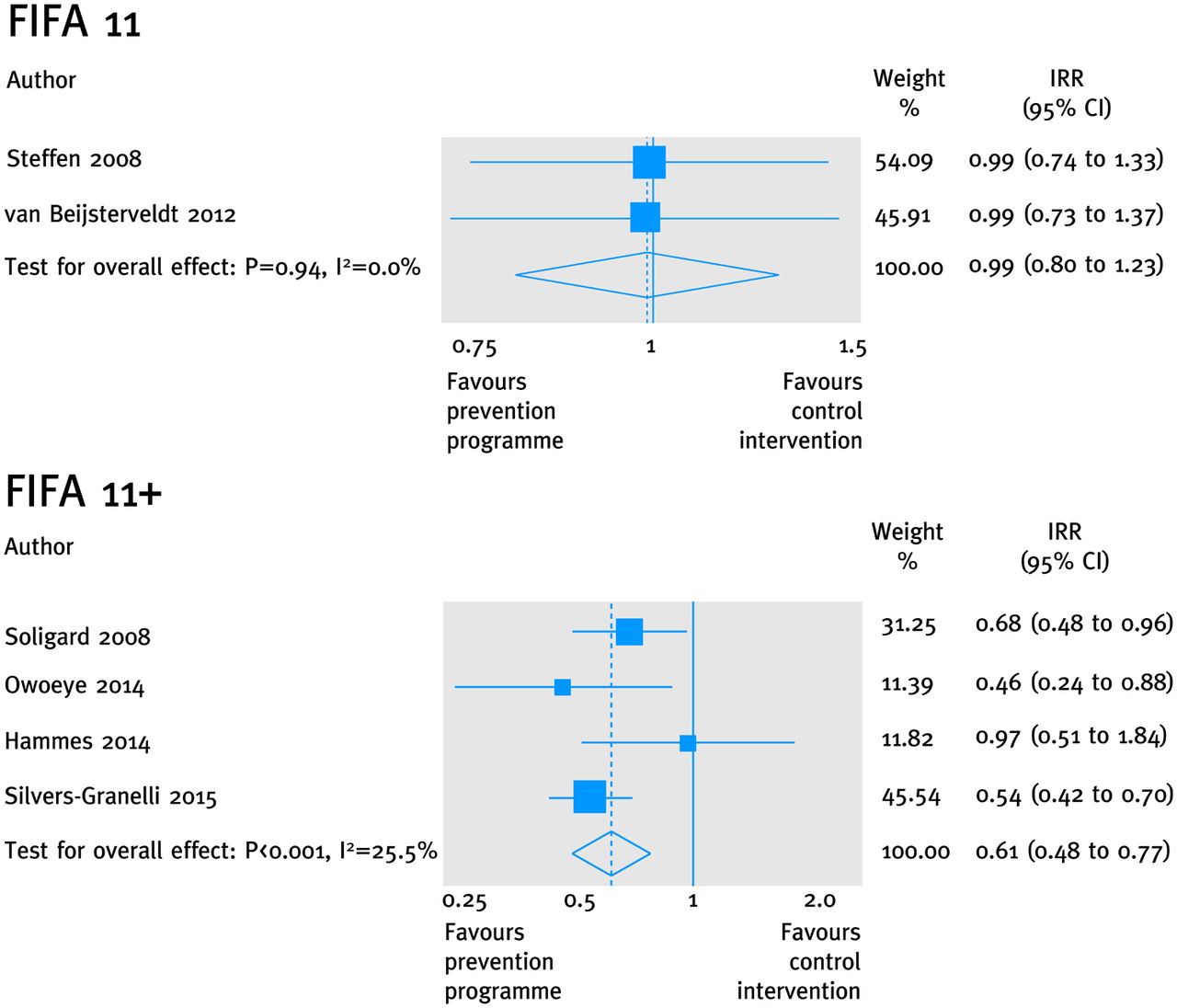
In the secondary analyses (type of programme), for the primary outcome (overall injury rate) the pooled results showed injury reduction per 1000 hours of exposure in the FIFA 11+ programme group compared with the control group (IRR 0.61; 95% CI 0.48 to 0.77, p<0.001, I2=25.5%, p=0.259), but no significant reduction in the FIFA 11 programme group (IRR 0.99; 95% CI 0.80 to 1.23, p=0.940, I2=0.0%, p=0.982) compared with the control group (figure 4).

Secondary analysis of overall injury rates for FIFA 11 and FIFA 11+, respectively, compared with control intervention. IRR, incidence rate ratio.
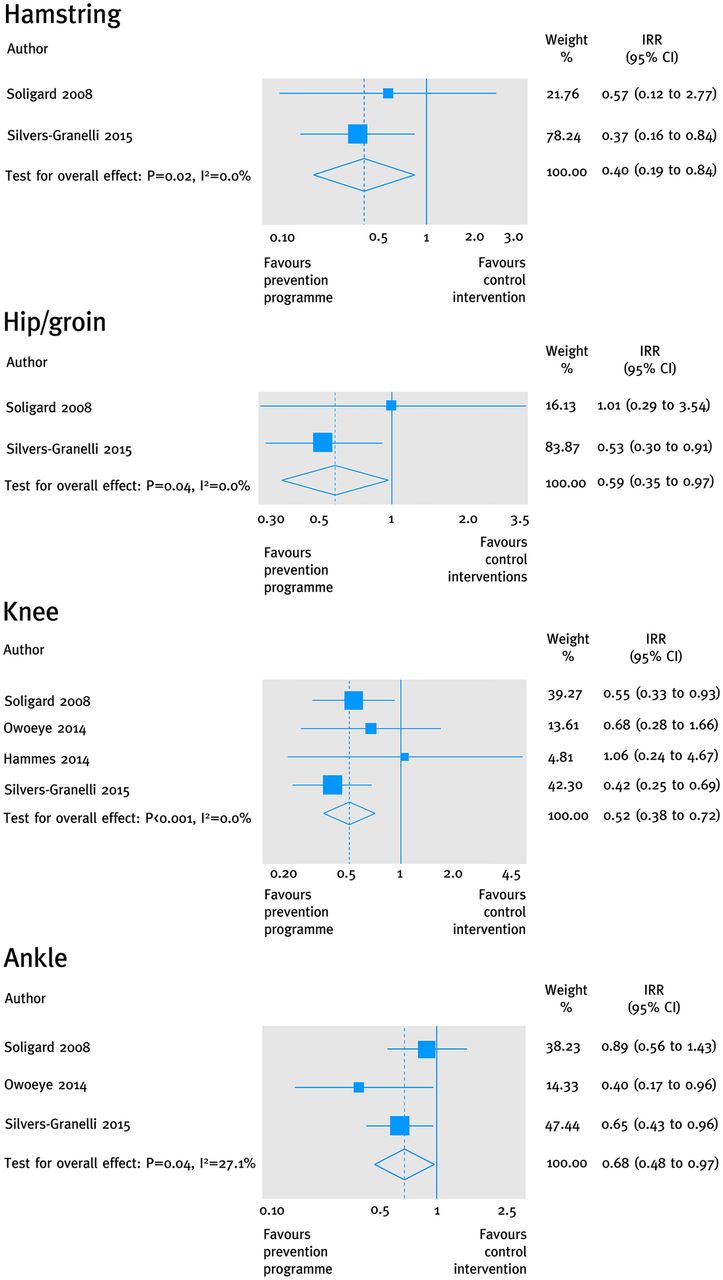
In the secondary analyses (body region) for the secondary outcome (region-specific injury rates) associated with the FIFA 11+ programme, an overall injury reduction existed in favour of the FIFA 11+ programme for lower limb injuries (IRR 0.63; 95% CI 0.48 to 0.81, p<0.001, I2=28.1%, p=0.243). More specifically, an overall injury reduction existed in favour of the FIFA 11+ programme for the following body region-specific outcomes: hamstring injuries (IRR 0.40; 95% CI 0.19 to 0.84, p=0.016, I2=0.0%, p=0.627), hip/groin injuries (IRR 0.59; 95% CI 0.35 to 0.97, p=0.037, I2=0.0%%, p=0.350), knee injuries (IRR 0.52; 95% CI 0.38 to 0.72, p<0.001, I2=0.0%, p=0.573) and ankle injuries (IRR 0.68; 95% CI 0.48 to 0.97, p=0.035, I2=27.1%, p=0.254; figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Secondary analyses of injury rates in relation to conducting the FIFA 11+ prevention programme compared with control intervention for the following specific body regions: hamstring, hip/groin, knee, and ankle. IRR, incidence rate ratio.
Compliance
Four of the six studies included information in the methods section concerning the FIFA 11 injury prevention programmes (FIFA 11+ and FIFA 11) which specified that the programme should be performed at least twice a week.11 ,12 ,40 ,43 This is in accordance with the recommendation from F-MARC on the execution of FIFA injury prevention programmes (http://www.f-marc.com/11plus/11plus/).
Study characteristics
For the six cluster-randomised studies, the average number of FIFA injury prevention programme sessions per week performed by included intervention teams was 1.2 (SD±0.7) sessions/week. From information on 158 intervention teams from five studies,11 ,12 ,21 ,33 ,43 out of 168 intervention teams from all six included studies in total,11 ,12 ,21 ,33 ,40 ,43 the number of FIFA injury prevention programmes sessions conducted on average per week at team level was obtained: 15% of teams did less than half a session per week, 53% did less than one session per week, 72% did less than one and a half sessions per week, and 87% did less than two sessions per week, meaning that 13% of all intervention clubs reached the suggested minimum of at least two sessions per week.
Synthesis of results
There was no significant association between average compliance in the individual studies and the overall injury incidence estimate from the intervention group in each study (adjusted R2=−18.8%, p=0.670). The post hoc meta-regression showed no significant association between compliance and IRR from each study (adjusted R2=72.4%, p=0.107). However, the direction of this non-significant association did point towards a higher preventative effect among the studies with higher compliance.
Risk of bias
Agreement by raters on risk of bias decisions for the six included cluster-randomised controlled studies was 78% (unweighted κ 0.66) for the six main risk of bias domains. All disagreements were caused by reading errors, where one of the reviewers had overlooked specific information. The two reviewers resolved all disagreements and no third reviewer involvement was needed for achieving consensus. Judgements on the domain ‘other bias’ were discussed among the reviewers for all six studies. All studies were assessed as having a high risk of bias in at least three domains (see online supplementary table S2). In all studies, neither intervention providers nor intervention receivers (performance bias), or outcome assessment in the form of self-reported injury (detection bias), could be considered blinded (see online supplementary table S2).
supplementary table S2
Risk of bias assessment of RCT studies investigating the effect of FIFA injury prevention programmes
Harms
None of the 32 studies included preplanned and standardised registration of information on adverse events.
Study characteristics
Out of all 32 studies9 ,11 ,12 ,21–49 including information on practical execution of the FIFA injury prevention programmes, only one cluster-randomised trial11 commented on possible harms (adverse events).
Synthesis of results
In relation to the total number of players performing the FIFA injury prevention programmes (n=4594), only one report of a minor hamstring strain was mentioned in the discussion section.11
Discussion
In this systematic review and meta-analysis where the primary outcome was the overall injury incidence, we found a statistically significant reduction in football injuries in recreational/subelite football players in favour of the FIFA injury prevention programmes compared with controls (no programme). The secondary analyses revealed that significant effects were found when pooling data from studies applying the FIFA 11+ prevention programme, whereas no significant effects were found when pooling data from studies applying the FIFA 11 prevention programme.
Level 1 evidence on the effect of FIFA injury prevention programmes
One previous systematic review including a meta-analysis by Al Attar et al14 was published in 2015. The study investigated the benefits of FIFA injury prevention programmes in footballers. While this study reported very similar overall injury reduction estimates to those of this study, the analyses and conclusions in the study by Al Attar et al14 were based on studies different from those included in the current review and meta-analysis. They included both randomised and observational studies in their meta-analysis,14 and thus did not separate meta-analyses on cluster-randomised/randomised controlled studies from analyses made on observational studies, as recommended in the Cochrane Handbook for Systematic Review of Interventions.17 Furthermore, cluster-adjusted estimates were not calculated by Al Attar et al,14 which means that the effective sample size was never taken into account.16 These are central points when performing systematic reviews including meta-analyses, which we have previously addressed in a letter to the editor,50 since we were concerned about the confidence one could have in the robustness of the estimates considering the statistical approach applied by Al Attar et al.14 To the best of our knowledge, this study is therefore the first systematic review and meta-analysis to exclusively provide level 1 evidence from cluster-randomised studies in a pooled meta-analysis and, furthermore, to account for possible cluster effects to the same extent shown by Soligard et al11 to be present among the teams in their large prevention study.
The FIFA 11 prevention programme versus the FIFA 11+ prevention programme
Our study documents that cluster-randomised studies of FIFA injury prevention programmes, when pooled together, show a substantial injury reduction in recreational/subelite football. This effect seems to be primarily driven by the large effect of the FIFA 11+ prevention programme, as the initially introduced FIFA 11 prevention programme alone does not seem to induce any injury-reducing effect. The heterogeneity analyses also support this notion, as significant heterogeneity between FIFA injury prevention programme studies only exists when pooling studies including FIFA 11 and FIFA 11+ together, and disappears when pooling FIFA 11 and FIFA 11+ prevention programme studies separately. This suggests that effect sizes from the studies including these two different programmes are diverse. This diversity cannot be investigated or explained by differences in the methodology used in these studies, as all studies have similar issues concerning risk of bias.
What modulates the injury-preventing effect of the FIFA 11+ programme: compliance or conditioning?
The finding of no injury-preventing effect from the FIFA 11 prevention programme in the large study by Steffen et al12 was initially suggested to be due to the low compliance. This was, however, somehow contradicted by the findings of van Beijsterveldt et al,21 which also did not show any injury-preventing effect of the FIFA 11 prevention programme, despite having a much higher team compliance than the study of Steffen et al.12 The findings of this study did not reveal any statistically significant association between compliance (the number of sessions performed per week at team level) and overall injury incidence, or overall injury IRR, although the post hoc analysis (using IRR) did point towards the possibility of a higher preventative effect among the studies with the highest team compliance. Two studies on the FIFA 11+ programme have indicated, within the same study context (female adolescent footballers) and injury definition, that there is an association between individual player compliance (number of sessions performed) and an overall injury- preventing effect.44 ,47 The indications from these studies suggest that FIFA 11+ is the most efficacious in individuals with higher compliance rates.44 ,47 Importantly, all studies11 ,12 ,21 ,33 ,40 ,43 included in the present systematic review and meta-analysis showed poor overall team compliance in terms of achieving the minimally suggested prevention programme dosage of at least two weekly team sessions. Only 13% of all teams from the included studies reached this benchmark. Getting at least two team sessions a week may therefore still be important to achieve the optimal effect, which is further supported by the fact that physiological and performance improvements documented from the FIFA 11+ programme were obtained from studies where football players were performing the prevention programmes 2–3 times a week for 8–12 weeks.23 ,25–30 ,34 Several FIFA 11+ programme studies have shown improvements in quadriceps and hamstring muscle strength, as well as in balance, agility and running speed, after only 8–12 weeks execution of the FIFA 11+ prevention programme compared with a control group with no warm-up programme.23 ,25–30 ,34 In contrast, the much less strenuous FIFA 11 prevention programme seems to induce no or only minimal physiological adaptations in quadriceps and hamstring strength, as well as in balance, agility or running speed.12 ,45 In this context, we speculate that the large difference in prescribed exercise intensity between the FIFA 11 and the FIFA 11+ prevention programmes could also provide a possible explanation for the discrepancy in injury-preventing effects between the two programmes. Accordingly, despite similar exercises being included in both programmes, the FIFA 11+ includes much higher loads/skill levels, longer active muscle contractions (time under muscle tension) and/or more repetitions for these type of exercises (figure 1). By introducing three exercise progression levels in the FIFA 11+ for each exercise, the number of repetitions and the time under tension for the strength training exercises alone are increased 2–3 times when a player exercises at levels 2 and 3.11 ,12
Harms related to the execution of FIFA injury prevention programmes
We also searched the literature for information on harms (adverse events) associated with the execution of the FIFA injury prevention programmes, and we included all studies published from 2004 onwards. We only found one report of injury on 4594 players performing the FIFA injury programmes. Based on the lack of preplanned and standardised registration of adverse events related to the FIFA injury prevention programmes, it is questionable how meaningful this result is. Future FIFA injury prevention programme studies need to ensure a more stringent and transparent reporting of adverse events related to the prevention programme, as it cannot be assumed that this is negligible based on reports from existing studies.
The FIFA 11+ prevention programme works in controlled studies—now it is time for adoption and implementation!
An injury-preventing effect of 25% was present when conducting the FIFA injury prevention programmes compared with following the usual training and match routines in recreational/subelite football, but no clinically meaningful conclusion can be drawn from this result due to the apparent diversity in effect sizes between studies looking at FIFA 11 and FIFA 11+ prevention programmes. More specifically, the FIFA 11+ prevention programme was shown to have a substantial injury-preventing effect by reducing football injuries by 39%, whereas a preventive effect from the FIFA 11 prevention programme alone could not be documented. Reducing injuries to this extent by using an exercise-based prevention programme has, furthermore, been shown to reduce injury-related costs in football by more than 40%.36 ,51
At this point in time, very little information on the actual adoption and implementation of the FIFA injury prevention programmes exists. Data from a few preliminary studies suggest that it may not be realistic to transfer the results from this study to elite football where application, relevance, dosage and intensity need to be specifically defined and adapted to the elite environment.52–56 More research and information on how to optimise adoption and implementation of FIFA 11+ at all levels should therefore be given high priority in the future, as positive effects from this prevention programme are now well documented. Providing substantial level 1 evidence-based information for the programme's preventive effects and for the injury-related cost that can be saved from using the programme is among the first important steps towards worldwide adoption and implementation. Furthermore, the information needs to reach health and football policymakers in order to highlight and encourage the importance of adopting and implementing the FIFA 11+ prevention programme at all recreational levels of football, as football is globally the most popular sport, and is an excellent form of physical activity. Football is, as such, already documented to be one of the most potent physical activities to induce important health benefits such as cardiovascular and metabolic health across ages and genders;3 thus, reducing football injuries associated with this form of activity is crucial.
Methodological limitations and considerations
A limitation of this study is that the included studies in the meta-analyses use different injury definitions. While four out of the six included studies only report ‘time-loss’ injuries, the remaining two studies report all injuries. Although such a discrepancy in injury definitions can provide different injury incidences between studies, it should not affect the IRR within randomised controlled trials. Furthermore, we did not assess statistically for publication bias (tests for funnel plot asymmetry) due to the low number of included studies in our meta-analyses. This is, however, in accordance with the Cochrane Handbook for Systematic Review of Interventions, V.5.1 (part 2: 10.4.3), where tests for funnel plot asymmetry are only recommended when there are at least 10 studies included in the meta-analysis.17
Despite not reaching the recommended dose, this study clearly shows that application of the FIFA 11+ reduces injuries dramatically in recreational and subelite football, which relates to the majority of players worldwide. However, more studies on exercise intensity, dose–response relationship, as well as adoption, implementation and compliance with the FIFA 11+ programme are called for to improve understanding of what the most important parameters are when we aim to adopt and implement the FIFA 11+ programme at the different levels of football.
In conclusion, an injury-preventing effect of the FIFA injury prevention programmes compared with usual care (no injury prevention programme) was shown in football. This effect was induced by the FIFA 11+ prevention programme which has a substantial injury-preventing effect by reducing football injuries to a clinically relevant 39%. In contrast to this, a preventive effect of the FIFA 11 prevention programme could not be documented.
What are the findings?
The FIFA 11+ prevention programme has a substantial injury-preventing effect by reducing football injuries in recreational/subelite football by 39%, whereas a preventive effect from the FIFA 11 prevention programme alone could not be documented.
The FIFA 11+ prevention programme reduces the top four most prevalent football injuries: hamstring, hip/groin, knee and ankle injury by 60%, 41%, 48% and 32%, respectively.
Less than 15% of intervention teams from randomised controlled trials investigating the effect of FIFA injury prevention programmes reached the recommended dose of two sessions per week during the season. This suggests that there is room for improvement when it comes to optimal adoption and implementation of FIFA injury prevention programmes.
Preplanned and standardised registration of adverse events related to the execution of FIFA injury prevention programmes are generally lacking. Possible adverse effects of the programmes have therefore not been sufficiently investigated at present.
How might it impact on clinical practice in the future?
Since football induces important health benefits across gender and lifespan by improving cardiovascular and metabolic health, and preventing risk factors for lifestyle diseases, the prevention of injuries through implementing the FIFA 11+ prevention programme in recreational/subelite football is important to optimise the number of players who will achieve important health benefits from playing football.
Through the provision of level 1 evidence-based information from the current study, worldwide adoption and implementation of the FIFA 11+ prevention programme should be further encouraged among all relevant parties—from health and football policymakers, stakeholders and associations to clubs, coaches and players at all recreational/subelite levels of football.
To support future adaptation and implementation of the FIFA 11+ programme, there is a need to focus on dose–response relationships, compliance and potential adverse events in relation to the usage of the FIFA 11+ at different levels of football.
References
Footnotes
Twitter Follow Kristian Thorborg @KThorborg
Contributors KT, KKK, MBC, EE, EMB and MSR all participated in the conception and design of the study. KT, KKK and EE were responsible for acquisition of data. MSR did the statistical analysis, and KT, KKK, MBC, EE and EMB took part in the interpretation of the analysis. KT drafted the manuscript. All authors critically revised the manuscript for important intellectual content and approved the final version of the manuscript. KT is the guarantor.
Funding EMB is supported by the OAK foundation (grant number Ocay-07-264).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The statistical code and data set are available from the corresponding author.