Article Text

Abstract
Objective To determine the incidence and characteristics of injuries in female and male gymnastics disciplines (artistic, rhythmic and trampoline) during three Olympic Games with a view to ultimately improving injury prevention.
Methods The National Olympic Committee’s head physicians and the medical teams of the Local Organising Committee of the Olympic Games reported daily the occurrence (or non-occurrence) of newly sustained injuries in artistic, rhythmic and trampoline gymnastics on a standardised report form during the 2008, 2012 and 2016 Summer Olympic Games.
Results During the three Olympic Games, 81 injuries were reported in a total of 963 registered gymnasts, corresponding to an incidence of 84 injuries (95% CI 67 to 102) per 1000 registered gymnasts, with no difference in injury incidence between female and male gymnasts. Thirty-eight per cent of injuries led to time-loss from sport. The most frequent injury location and injury type were the ankle (22%) and sprain (35%), respectively. The most common diagnosis was ankle sprain (14% of all injuries and 23% of time-loss injuries). The injury incidence was highest in female (107±35) and male artistic gymnastics (83±32), followed by female rhythmic gymnastics (73±30), and lower in male (63±69) and female (43±43) trampoline gymnastics.
Conclusions Research should focus on preventing injuries in artistic gymnastics and of the condition of ankle sprain. Injury surveillance studies should be continued during major championships and throughout the entire competitive season as the Olympic Games provides only a snapshot (although an important one).
- epidemiology
- gymnastics
- olympics
- injury
- injury prevention
Statistics from Altmetric.com
Introduction
Gymnastics is a popular sport with high participation rates worldwide.1 The International Gymnastics Federation (FIG, http://www.fig-gymnastics.com) has 148 affiliated/associated federations, and it is estimated that worldwide about 50 million people of all ages regularly perform gymnastics in a club setting. Among the different gymnastics disciplines, the current programme at the Olympic Games includes artistic gymnastics (men’s and women’s), rhythmic gymnastics (women’s) and trampoline gymnastics (men’s and women’s),1 2 comprising about 320 gymnasts (≈3% of all registered athletes) at each Olympic Games.
Gymnastics requires explosive, balance and artistic skills, and includes movements with high levels of intensity and difficulty.1 3 Elite gymnasts, aged from 7 to 18 years, are exposed to high training loads of up to 21–37 hours per week, for 11–12 months per year according to reports.1 2 4–6 In addition, gymnastics training begins in childhood; talent scouting for USA Gymnastics looks at children aged between 6 and 11 years.2 3 These gymnasts have immature musculoskeletal systems and consequently their growth cartilage, articular cartilage and bones are more susceptible to injury.7 The combination of all these aspects, and others including low-energy availability, gives rise to the concern regarding the risk of injury.1 2 6 8
Several studies have provided epidemiological data on female artistic gymnasts of different ages, levels and settings.1 2 These studies cover gymnasts at elite level,4 5 9–11 club level4 6 12 13 and school activities.14–17 Injury rates range from 1.6 to 4.1 per 1000 hours of training,4–6 9 with the elite-level gymnasts being exposed to higher rates, more severe injuries6 9 and higher risk during competitions (2–6 times more than in training conditions).6 15 16 In comparison, much less is known regarding the injury risk in men’s artistic,11 12 17 18 women’s and men’s trampoline,19 and women’s rhythmic gymnastics.20 21
As a first step towards prevention strategies,22 23 improving knowledge on injury epidemiology in the three gymnastics disciplines will be relevant. In addition, given the differences in the nature of these Olympic disciplines (eg, in physical demands, skills and rules), it is of interest to determine whether injury risks and characteristics differ across disciplines.1 2 The Olympic Games provide a unique opportunity to analyse and compare the injury risk and characteristics in elite-level athletes of different disciplines under similar conditions (eg, same level of play, identical environmental conditions). In addition, given the efforts of the IOC to protect athletes’ health,24–26 and by the FIG to prevent gymnastics injuries (http://www.fig-gymnastics.com), as well as given the changes made by the FIG to the rules and in the Code of Points,1 2 it is of interest to analyse the change in injury risk and characteristics over time.
We aimed to determine the incidence and characteristics of injuries in elite gymnastics, specifically in the three Olympic disciplines (artistic, rhythmic and trampoline) during three consecutive Olympic Games (2008, 2012 and 2016) and to evaluate their changes over time.
Methods
The IOC injury and illness surveillance system for multisport events24 was used to record the injuries during the last three summer Olympic Games: the Beijing Olympic Games from 9 to 24 August 2008 (OG 2008),25 the London Olympic Games from 27 July to 12 August 2012 (OG 2012)26 and the Rio Olympics Games from 5 to 21 August 2016 (OG 2016).
The study design, study implementation, injury definition and data collection procedures were identical for the three Olympic Games and have previously been described in detail.24–26 The National Olympic Committee’s (NOC’s) head physicians and the medical teams of the Local Organising Committee of the Olympic Games were asked to report daily the occurrence (or non-occurrence) of newly sustained injuries on a standardised paper report form.24–26 An injury was defined as ‘any musculoskeletal complaint or concussion newly incurred (exclusion of pre-existing and not fully rehabilitated injuries) due to competition and/or training during the Olympic Games that received medical attention regardless of the consequences with respect to absence from competition or training’.24 In cases where a single incident caused multiple injury types or affected multiple body parts, only the most severe diagnosis was recorded.25 26 Confidentiality of all information was ensured so that no individual athlete could be identified. Ethical approval for injury and illness surveillance during these Olympic Games was obtained from the medical research ethics committee of the South-Eastern Norway Regional Health Authority, Norway (2011/388-4).
Incidences of injuries were calculated as the number of injuries per 1000 registered gymnasts using a list of gymnasts provided by the IOC. Data were analysed and are presented using numbers, frequencies, percentages, cross-tabulations, incidences with 95% CIs, relative risks (RR) with 95% CI, magnitude thresholds27 and with the χ2 test. Comparative analyses between disciplines and individual Olympic Games were performed only if the number of injuries was statistically sufficient. All data were processed using Excel. Significance was accepted at p<0.05.
Results
Number and incidence of injuries
A total of 963 gymnasts participated in the three Olympic Games, competing mainly in artistic and rhythmic gymnastics (90.1% of all registered gymnasts). These two disciplines accounted for most of the recorded injuries (93.8%) (table 1).
Number of registered gymnasts and (time-loss) injuries, percentages of (time-loss) injuries and incidences of injuries per 1000 registered gymnasts in the three Olympics gymnastics disciplines according to sex, during the 2008, 2012 and 2016 Olympic Games
Eighty-one injuries were reported in gymnasts, corresponding to an incidence of 84.1±17.5 injuries per 1000 registered gymnasts. Fifty-four injuries were reported in female (66%) and 27 (33%) in male gymnasts. The injury incidence was similar between female and male gymnasts (86.4±22.0 vs 79.9±28.9 injuries per 1000 registered gymnasts, respectively; RR=1.08; 95% CI 0.69 to 1.68, trivial) (table 2).
Number of registered gymnasts and injuries, incidences of injuries per 1000 registered gymnasts and relative risks (female being the reference group) with lower and upper limits of 95% CI (±95% CI) and probabilistic inferences about the true standardised magnitude in relative risks, in male and female gymnasts during the 2008, 2012 and 2016 Olympic Games (OG)
Thirty-one injuries led to time-loss from sport (38.3%), corresponding to an incidence of 32.2±11.1 injuries per 1000 registered gymnasts, without any significant difference between female and male gymnasts (27.2±12.8 vs 41.4±21.2 injuries per 1000 registered gymnasts, respectively; RR=0.66; 95% CI 0.33 to 1.32, small) (table 1).
The injury incidence in artistic gymnastics was significantly higher in 2016 than in 2008. While a similar trend in the same direction was observed for women’s artistic gymnastics, the results were not significant for men’s artistic gymnastics (table 3).
Changes in injury incidences per 1000 registered gymnasts with 95% CI (±95% CI) from the 2008 to the 2012 and the 2016 Olympic Games (OG) regarding the gymnastics disciplines
Injury characteristics in gymnastics
The affected body parts, types, circumstances and causes are presented in tables 4 and 5. The lower limb was affected in 62.8% of injuries, the trunk in 23.1% and the upper limb in 14.1%. The most frequent injury location was the ankle (21.8%), followed by the lumbar spine (14.1%) and the foot (12.8%). The most frequent types of injury were sprains (34.6%), followed by tendinopathy/arthritis/impingements (17.3%), contusions (9.9%) and fractures (7.4%). The most common diagnosis was ankle sprain (13.6%).
Percentage of injuries (and percentage of time-loss injuries) for location, type, circumstance and causes according to the three Olympic gymnastics disciplines and sex during the 2008, 2012 and 2016 Olympic Games
Percentage of injuries (and percentage of time-loss injuries) according to the location and types for all the three Olympic gymnastics disciplines during the 2008, 2012 and 2016 Olympic Games
More injuries occurred during training (49.4%) compared with competition (39.5%) (missing information for 11.1%). Acute trauma injuries were dominant (contact with immobile objects (23.4%) and non-contact trauma (22.1%)), followed by overuse injuries (with both sudden (15.6%) and gradual onset (11.7%)), and recurrence of previous injuries (14.3%).
The most common time-loss injury location was the ankle (28.6%), and most common time-loss injury type was sprains (41.9%), the main circumstance was during competition (58.1%), and the most common causes were contact with immobile object (33.3%) and non-contact trauma (30.0%) (table 4). The injury frequency differed significantly between injuries and time-loss injuries for circumstance (χ2=3.9, p<0.05), but not for location, type and cause (table 5). The proportion of time-loss injuries was higher in competition than in training (56.3% vs 22.5%; χ2=8.6, p=0.003). All eight injuries with >4 weeks absence were sustained in artistic gymnastics, five during competition, one during training and two unknown, and were two foot fractures, one ankle fracture and one lower leg fracture, one neck meniscus/cartilage lesion, one ruptured knee ligament, one groin sprain and one knee lesion.
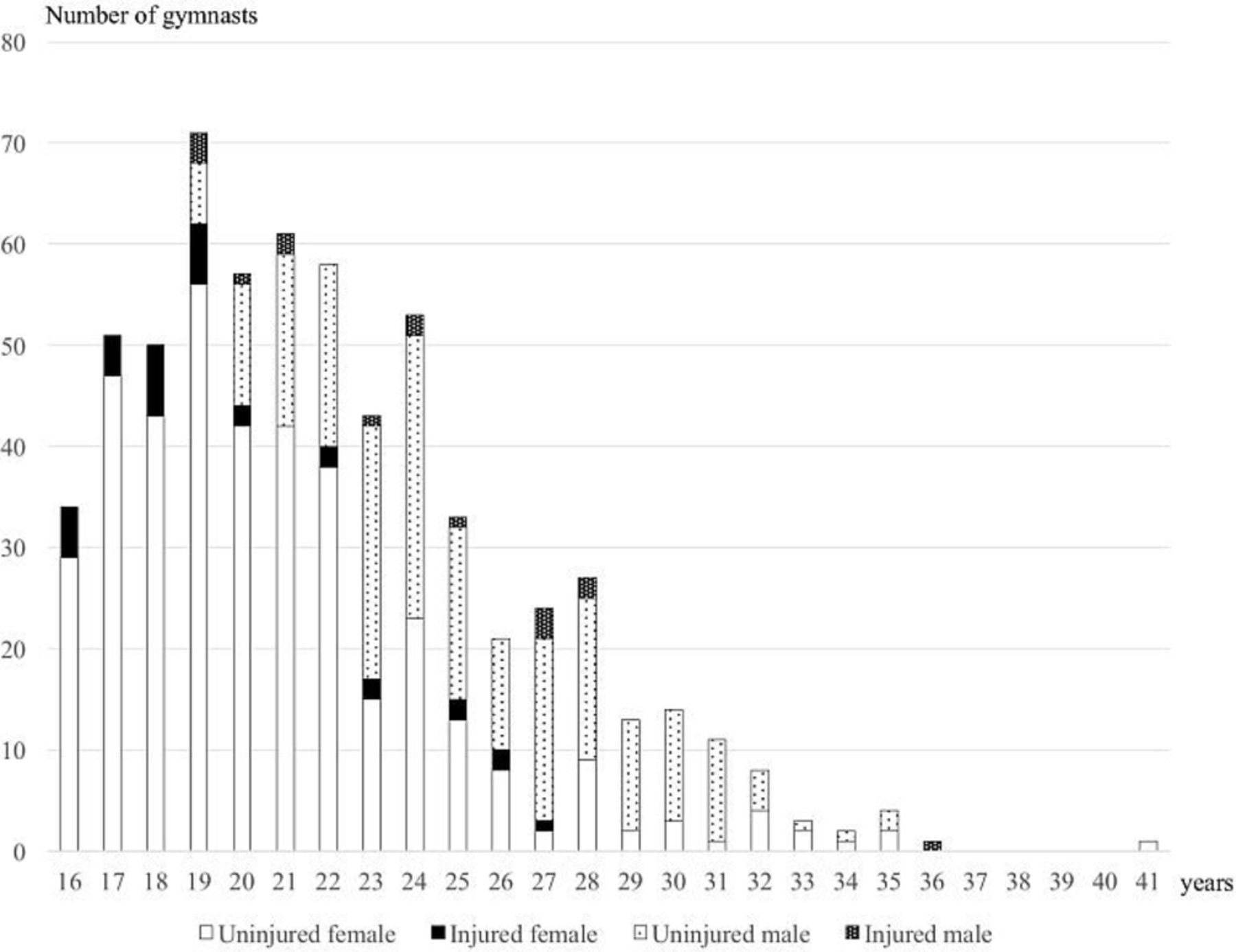
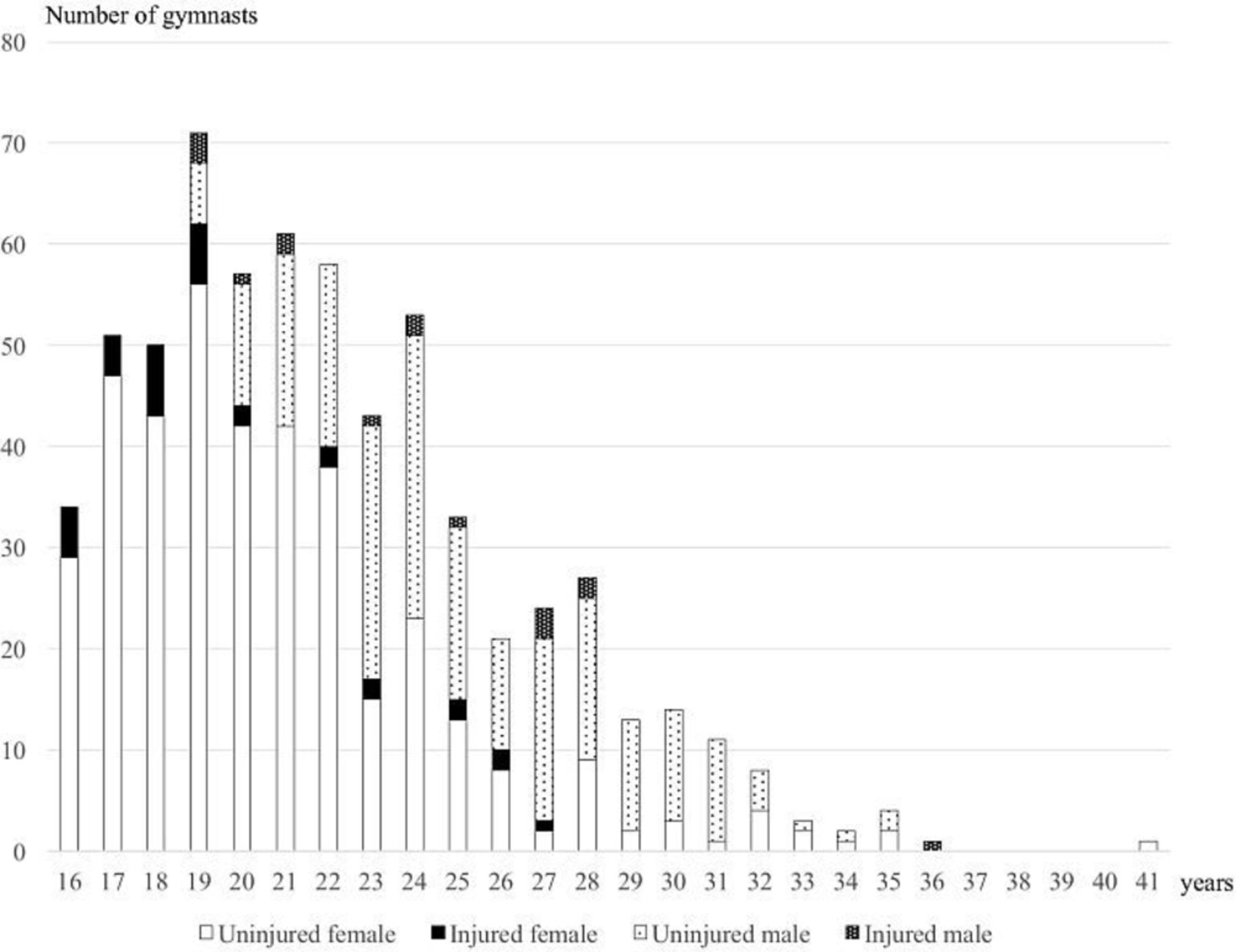
The mean age of injured gymnasts was 21.1±4.3 years (range from 16 to 36 years; 32 missing values including 24 from OG 2012), with significant differences between female and male gymnasts (19.6±3.3 vs 24.1±4.5 years; p<0.001), but without significant differences in the mean age of uninjured gymnasts (22.2±4.3 years, range from 16 to 41 years; values were missing for OG 2012 (n=323); p=0.07). Eighteen per cent of injured gymnasts were under the age of 18 years and 51% were <20 years, compared with 13% and 31% of uninjured gymnasts, respectively (χ2=1.2, p=0.3; χ2=8.6, p=0.003, respectively). Numbers of injured and uninjured gymnasts are presented in figure 1, and injury incidences per age category are reported in table 2.
{kind=link}
Number of uninjured and injured male and female gymnasts in different age groups during the 2008, 2012 and 2016 Olympic Games.
The comparison of the injury characteristics between the three Olympic Games was not possible due to the small number of injuries.
Injury incidence and characteristics according to gymnastics disciplines
Injury incidences were generally higher in women’s and men’s artistic gymnastics as well as in women’s rhythmic gymnastics, and lower in men’s and women’s trampoline gymnastics, whereas time-loss injury incidences were higher in men’s and women’s artistic gymnastics, and lower in women’s rhythmic gymnastics (tables 1 and 2). Time-loss injuries represent an important proportion of injuries in men’s artistic gymnastics (58.5%), without statistical differences with women’s artistic or rhythmic gymnastics (χ2=3.2; p=0.20).
The characteristics of (time-loss) injuries according to disciplines are presented in table 4. Due to the low number of injuries per disciplines, only comparisons between women’s and men’s artistic gymnastics were performed. The injury frequency differed significantly between women’s and men’s artistic gymnastics for circumstance (χ2=4.4, p<0.05), but not for location, type and cause (table 4). Compared with males, female artistic gymnasts sustained significantly more ankle sprains (27.4±18.7 vs 3.4±6.7 injuries per 1000 registered gymnasts, respectively; RR=7.95; 95% CI 1.00 to 63.1, very large) and training injuries (51.4±25.3 vs 17.2±15.0 injuries per 1000 registered gymnasts, respectively; RR=2.98; 95% CI 1.10 to 8.09, moderate), whereas no gender differences were found for other locations, types, causes or circumstances.
Discussion
The main findings of the present study were that (1) injury incidence was 84±18 injuries per 1000 registered gymnasts during the three Olympic Games without any difference between female and male gymnasts, (2) the injury incidence in artistic gymnastics increased from the 2008 to the 2016 Olympic Games, (3) injury incidences varied between age groups with higher rates among the youngest and the oldest gymnasts, (4) ankle sprain was the most frequent diagnosis (14%), (5) higher injury incidences were reported in women’s and men’s artistic gymnastics than in rhythmic and trampoline gymnastics, and (6) about half of the injuries in artistic gymnastics (58% for male and 42% for female gymnasts) resulted in time-loss injuries but just 19% in rhythmic and none in trampoline.
Gymnastic injury risk is moderate
The overall incidence of gymnastic injury during the Olympic Games was lower than the overall injury incidence in all sports reported from the 2008 and 2012 Summer Olympic Games.25 26 Artistic, rhythmic and trampoline gymnastics can be considered as Olympic sports with a lower risk of injury compared with taekwondo, football, BMX, handball, mountain biking, hockey, weightlifting, athletics and badminton (all with >150 injuries per 1000 athletes).26 However, the injury risk in the three gymnastic disciplines combined was higher than in sports with injury rates <50 injuries per 1000 athletes, for example, archery, canoeing, track cycling, rowing, shooting and equestrian sports in the 2012 OG.26
In comparison to other individual sports and data available from international Championships using a similar injury surveillance system,24 the overall gymnastic injury incidence was also lower than those during athletics28 or aquatic29 championships.
Comparison of these injury incidences with previous epidemiological studies in gymnastics, especially with prospective studies collecting injury data during the entire season,4–6 9 11 13 15 16 is difficult because the injury surveillance systems used were different particularly with regard to the exposure (per number of hours of practice or per gymnast per year in comparison to per number of gymnasts) and consequently the incidences.1 2
Increase of injury rate in artistic gymnastics from the 2008 to the 2016 Olympic Games
Our analysis showed a significant increase of injury incidence in artistic gymnastics from 2008 to 2016, and a similar trend in female artistic gymnastics (table 3). This could be considered as surprising given the efforts made by the IOC and the FIG to prevent injuries in elite athletes. However, this result could be explained by the other changes, such as those in the FIG Code of Points, increasing the required levels of difficulty.2 This should encourage all stakeholders around gymnasts to reconsider the Code of Points with respect to its influence on the injury risk. This result should be interpreted with caution due to the small number of gymnasts and injuries, and the fact that the overall injury incidence in the OG increased from 2008 (96 injuries per 1000 registered athletes25) to 2012 (129 injuries per 1000 athletes26), most probably due to a better compliance of the NOCs medical teams and their physicians with the surveillance system. Ongoing injury surveillance during the Olympic Games and other international gymnastics competitions can help to determine the impact of proposed injury prevention measures and/or changes to the Code of Points 2 on the gymnasts’ injury risk.
Ankles and ligaments were most often affected
In the present study, the ankle was the most frequently injured location, followed by the lumbar spine, foot, hip and groin. Previous studies in gymnastics also reported such locations as sustaining the most injuries.1 4–6 9 12–17
An ankle sprain was the most frequent injury diagnosis (14%) and the primary time-loss injury (22.6%). Although previous reports have not always found it be the most common diagnosis, ankle sprains have always been very high on the list of gymnastics injuries especially in artistic gymnastics.1 5 6 9 15 17
The important proportion of ligament (37%) and bone injuries (12%) was consistent with previous studies in gymnastics,1 2 5 6 9 12 13 15 and also similar to findings from other contact and/or pivot-shift sports (eg, football,30 handball31 or alpine skiing32).
Although not statistically significant, differences in injury frequencies were observed between women’s and men’s artistic gymnastics for location (higher proportion of ankle injuries for females and knee injuries for males) and type (higher proportion of sprains for females and fractures for males) (table 4). The sex-related differences in apparatus (female: vault, uneven bars, beam, floor exercise; and males: floor exercise, pommel horse, rings, vault table, parallel bars and horizontal bar), and consequently in the biomechanical and physiological constraints could explain these differences in injury characteristics.
Gymnastics competition leads to a higher risk of time-loss injuries than training
When analysing injury circumstances, we reported a higher proportion of time-loss injuries in competition than in training (table 1). Among the eight injuries requiring >4 weeks of absence, five were competition injuries (one in training and two unknown). This is consistent with a previous study, where a higher rate of severe injury in competitions, especially in high-level gymnasts, was reported.6 The role of different equipment and conditions, lack of confidence or preparation, nerves and time pressures, skill difficulties, travel and possibly insufficient training have all previously been discussed as aetiologies or factors of the high injury rates during competitions.2 6 13
In addition, the incidence of training injuries may be lower in the context of the Olympic Games because the conventional wisdom tends to reduce training days during the Olympic Games, allowing these athletes a moment of respite between competition days to save energy and thereby also reducing their risk of injury.
It is also important to note that fortunately no catastrophic injuries (head and spinal cord injuries1 33) were suffered by gymnasts either in the present study (only one neck meniscus or cartilage lesion with an estimated 42 days of absence) or in any other previous gymnastic injury surveillance protocol.5 6 8 9 11
Artistic gymnastics is the discipline associated with the highest injury risk
To our knowledge, data are limited regarding the injury rate and characteristics in men’s artistic,11 12 17 18 women’s and men’s trampoline19 and rhythmic gymnastics.20 21 The present study reports information on the injury rates and characteristics in these disciplines during three Olympic Games. However, a significant limitation of the present study is the small number of registered gymnasts, and consequently of injuries which restricted statistical comparison between gymnastics disciplines. The present study showed that injury incidence varied between disciplines with artistic gymnastics having the highest risk. Higher injury incidences were reported in women’s and men’s artistic gymnastics than in women’s rhythmic gymnastics, and lower injury incidences in women’s and men’s trampoline gymnastics. Differences in physical demands, skills and rules probably influence the injury risk. Comparison with previous studies is difficult because, to our knowledge, this is the first study to analyse the injury rates under identical conditions in these three Olympic disciplines.
Paying attention to young gymnasts!
Gymnastics involves young athletes with immature musculoskeletal systems,6 13 and we wanted to analyse the influence of age on injury risk. Unfortunately, age was missing for 34% of registered gymnasts and 40% of injured gymnasts, which represents another significant limitation of the study.
A preliminary analysis showed that the mean age of injured gymnasts was 21±4 years, without significant differences with the mean age of uninjured gymnasts (22±4 years). The fact that this mean age seems lower than that reported for all sports during the 2008 OG (26±5 years)25 or during international athletics championships (26±4 years),28 is in favour of our hypothesis that gymnastics injuries involve young gymnasts.
Injury incidences varied between age groups with higher rates among the youngest and the oldest gymnasts. This is consistent with clinical experience since young gymnasts could be more susceptible to injury due to their immature musculoskeletal system and lower physical conditioning, and older gymnasts could have weaker musculoskeletal tissues caused by ageing and years of gymnastic practice.
Further studies should be done to clearly analyse the influence of age and maturation on gymnastics injury risk and its characteristics.
Methodological considerations
Edouard et al 34 highlighted the need of clear methodological parameters to ensure the quality of the injury surveillance system: medical team participation, coverage of athletes, response rate and completeness of data. For the present study, these parameters are not specific to gymnastics, but are applicable to all disciplines included in the various Olympic Games, and showed good methodological quality.25 26
To our knowledge, this is the first study to provide data on the injury risk and characteristics of elite-level gymnasts in a context of top-level competition using proper surveillance methods. The Olympic Games clearly represent a unique opportunity to have a picture of the risk and characteristics of injuries sustained by elite-level gymnasts during a major international competition. However, injury surveillance does not allow a clear picture of overuse injuries,26 which represent an important proportion of injuries in this sport with high training loads and durations.2 5 6 8 9 This clearly supports the need of further studies over an entire season.
The exposure used in the present study (per 1000 registered gymnasts) is the reference for epidemiological studies during multievent competitions.24–26 However, it does not account for the potential variance in exposure of participants to risk of injury (eg, not all gymnasts compete in all events).2 As a result, the injury rates reported in the present study lack precision and are difficult to compare meaningfully within and across studies.
The data used in the present study are based on a general data acquisition form for all Olympic sports24–26 and do not include a specific questionnaire for gymnastics. Gymnastics includes different competition formats, a variety of apparatus, specific rules for each apparatus, as well as specific pathologies for each apparatus.3 6 16 A more specific surveillance of gymnastics would require noting the apparatus concerned, the level of the difficulty of the exercise as well as the format of competition.
Suggestions for gymnastics injury prevention
These preliminary results and their limitations support the value of running injury surveillance studies during international competitions (gymnastics continental and world championships) as is done with football,30 athletics28 and aquatics.29 In addition, pre-participation health questionnaires would be relevant for such injury surveillance29 35 since 10%–20% gymnasts present injury complaints at some time during a season,6 and this would provide vital information regarding any injuries occurring in the month preceding a championship and so better understand injury risks during international competitions. In addition, injury surveillance over an entire season is highly relevant for injury prevention.6 13 22 This should at least include demographic information, longitudinal anthropometric follow-up, information on the movement during which an injury occurred, monitoring of impact loads and psychological parameters.6 8 10 13 In addition, it is also fundamental to collect injury data both during competitions and in-season training as well as exposure data for all gymnasts to provide accurate evaluations of injury risks.2
Efforts should be focused on artistic gymnastics since this is the discipline with the highest injury risk and the greatest number of gymnasts. This can include long-term injury surveillance monitoring,3 36 optimal medical follow-up of gymnasts with musculoskeletal screening and/or pre-participation physical examination,8 36 optimised physical conditioning,36 37 good mastery of techniques,3 improving the preparation for gymnastics competition (intensity and skill difficulty, performance anxiety and competitive stress) and also a better knowledge of the constraints/stresses/biomechanics of artistic gymnastics whether this be the acute constraints inherent in the movements themselves or chronic constraints due to the accumulation of training loads.38 Other strategies for injury prevention in artistic gymnastics have been proposed such as monitoring an gymnast’s growth and paying attention to the immature musculoskeletal system, preventing the first injury, improving healing and the rehabilitation process, improving recovery, follow-up of nutritional aspects, mental preparation, education, equipment, rules and the Code of Points.3 6 8 36 39 We speculate that improving these aspects may also allow an improvement in performance; that would be a win-win performance-prevention strategy.
Given the high percentage of ankle sprains, especially in female gymnasts, strategies focusing on primary and secondary ankle sprain prevention should be implemented including strengthening, postural control and neuromuscular training, and/or ankle bracing.15 40
Since a third of all injuries are caused by contact with an immobile object, this raises a question about the equipment; gymnastic injury prevention can be done by improving the safety of the equipment.3 8 36
In summary, artistic gymnastics is the discipline with the highest injury risk, while injury risk in rhythmic gymnastics and trampoline was low in the years studied. Consequently, suggestions to prevent injuries should target the group of artistic gymnasts and their increased risk of sustaining time-loss injuries and ankle sprains. These efforts will be facilitated by regular/constant monitoring of injuries and training loads.
What are the new findings?
Injury incidence was 84 injuries (95% CI 67 to 102) per 1000 registered gymnasts during the three Olympic Games, with no significant risk difference between female and male gymnasts.
Artistic gymnastics was the discipline with the highest injury risk with 107 (95% CI 71 to 141) and 83 injuries (95% CI 51 to 114) per 1000 registered gymnasts in female and male gymnasts, respectively.
Injury incidences varied among age groups with higher rates among the youngest and the oldest gymnasts.
An ankle sprain was the most frequent injury diagnosis (14%) and time-loss injury diagnosis (23%).
Ligament (37%) and bone injuries (12%) represented the most frequent injury types of injury.
How might it impact on clinical practice in the future?
Gymnastic injury prevention should be oriented towards the discipline of artistic gymnastics, focusing on ankle sprains, especially in female gymnasts, and on bone and knee injuries in male gymnasts.
Acknowledgments
The authors highly appreciate the cooperation of the medical staffs of the National Olympic Committee and the medical teams of the medical staffs Local Organising Committee of the Olympic Games who volunteered their time to collect the data for this project.
References
Footnotes
Contributors PE: substantial contributions to the conception and design of the study, analysis and interpretation of data, drafting, writing and revising of the manuscript, and final approval of the version to be published. KS: substantial contributions to the conception and design of the study, collection, analysis and interpretation of data, drafting, writing and revising of the manuscript, and final approval of the version to be published. AJ: substantial contributions to the conception and design of the project, collection and interpretation of data, revision of the manuscript, and final approval of the version to be published. ML: substantial contributions to the interpretation of data, revision of the manuscript, and final approval of the version to be published. TS: substantial contributions to the collection, analysis and interpretation of data, revision of the manuscript, and final approval of the version to be published. LE: substantial contributions to the conception and design of the project, collection and interpretation of data, revision of the manuscript, and final approval of the version to be published.
Funding The data acquisition was funded by the International Olympic Committee, which has contributed to planning, developing and executing the injury surveillance procedure from with the Beijing Games onwards.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The present study is a part of an injury and illness surveillance study during the Olympic Games, which was reviewed and approved by the medical research ethics committee of the South-Eastern Norway Regional Health Authority, Norway (2011/388-4).
Provenance and peer review Not commissioned; externally peer reviewed.