Article Text

Abstract
Objective Normal-weight oligo-amenorrhoeic athletes (OAA) are at risk for low bone mineral density (BMD). Data are lacking regarding the impact of oestrogen administration on bone outcomes in OAA. Our objective was to determine the effects of transdermal versus oral oestrogen administration on bone in OAA engaged in weight-bearing activity.
Methods 121 patients with OAA aged 14–25 years were randomised to receive: (1) a 17β-estradiol transdermal patch continuously with cyclic oral micronised progesterone (PATCH), (2) a combined ethinyl estradiol and desogestrel pill (PILL) or (3) no oestrogen/progesterone (NONE). All participants received calcium and vitamin D supplementation. Areal BMD was assessed at the lumbar spine, femoral neck, total hip and total body less head using dual-energy X-ray absorptiometry at baseline, 6 and 12 months. Intention-to-treat (ITT) and completers analyses were performed.
Results Randomised groups did not differ for age, body mass index or BMD Z-scores at baseline. For ITT analysis, spine and femoral neck BMD Z-scores significantly increased in the PATCH versus PILL (p=0.011 and p=0.021, respectively) and NONE (p=0.021 and p=0.033, respectively) groups, and hip BMD Z-scores significantly increased in the PATCH versus PILL group (p=0.018). Similar findings were noted in completers analysis.
Conclusion Transdermal estradiol over 12 months improves BMD in young OAA, particularly compared with an ethinyl estradiol-containing contraceptive pill/oral contraceptives.
Trial registration number NCT00946192; Pre-results
- female athlete triad
- endocrine
- bone mineral density
- adolescent
- bone
Statistics from Altmetric.com
What are the findings?
In this randomised clinical trial of adolescent and young adult oligo-amenorrhoeic athletes, lumbar spine and femoral neck bone mineral density (BMD) Z-scores significantly increased with transdermal estradiol plus cyclic oral progesterone compared with a combined oral contraceptive and compared with no therapy.
Hip BMD Z-scores significantly increased with transdermal estradiol plus cyclic oral progesterone administration compared with combined oral contraceptive use.
How might it impact on clinical practice in the future?
Transdermal estradiol administration may be a useful adjunct therapy to enhance bone health in oligo-amenorrhoeic athletes.
Combined oral contraceptives should not be used to improve bone health.
Introduction
Athletes participating in endurance and leanness sports are at particular risk of developing the Female Athlete Triad of low energy availability, menstrual dysfunction and low bone mineral density (BMD).1 2 Amenorrhoea occurs in up to 66% of athletes.3 Beneficial effects of weight-bearing exercise on bone during adolescence/young adulthood are lost in oligo-amenorrhoeic athletes (OAA), who have lower BMD than eumenorrhoeic athletes,4 5 increasing fracture risk.6 Because adolescence is critical for bone accrual,7 preventing and treating oligo-amenorrhoea during this developmental period is essential for optimising future bone health.
Many physicians prescribe combined oral contraceptives (COCs) to treat oligo-amenorrhoea and/or low BMD, despite limited supporting data.8 9 Lack of efficacy of oral oestrogen is attributed to: (1) hepatic first-pass effects that downregulate insulin-like growth factor-1 (IGF-1), an important bone-trophic hormone, and (2) ethinyl estradiol, the most common form of oestrogen in COCs, being non-physiological.10 Transdermal 17β-estradiol (E2), the physiological form of oestrogen, avoids IGF-1 downregulation and increases BMD in low-weight girls with anorexia nervosa (AN).11 Because pubertal IGF-1 increases are critical to adolescent bone accrual, lack of IGF-1 suppression with transdermal estradiol may be beneficial to adolescents/young adults. No studies have examined the impact of transdermal versus oral oestrogen replacement on BMD in normal-weight adolescent/young adult OAA. We aimed to determine the impact of a transdermally administered, physiological oestrogen versus a common COC versus no oestrogen on BMD in young, normal-weight, weight-bearing OAA. We hypothesised that BMD would improve over 12 months with transdermal 17β-E2 administration compared with COCs or no oestrogen.
Subjects and methods
Subject selection
Following a preliminary telephone call, we invited 140 girls/young women aged 14–25 years for a screening visit; 121 met criteria for OAA and consented for participation. These ages were chosen because women 14–25 years old are actively accruing bone towards attainment of peak bone mass.12 All participants had a bone age ≥14 years, when statural growth is mostly complete and oestrogen replacement should not impact adult height. All had a body mass index (BMI) of >10th percentile or >17.5 kg/m2 to avoid enrolling women with active AN per Diagnostic and Statistical Manual of Mental Disorders, 4th edition.13 Oligo-amenorrhoea was defined as absence of menses for ≥3 months within a ≥6-month period of oligomenorrhoea (cycle length >6 weeks) preceding study participation, or absence of menarche at ≥15 years. Six subjects had primary amenorrhoea (other pathology ruled out before study entry). A study psychologist assessed participants for current/past eating disorders: 28 had histories of suspected/diagnosed eating disorders. All were above the ‘low weight’ threshold (BMI of >10th percentile or >17.5 kg/m2) and deemed eligible for participation.
Enrolment was limited to endurance athletes participating in ≥4 hours of aerobic weight-bearing training and/or ≥20 miles of running weekly for ≥6 preceding months to minimise physical activity variability. Gymnasts and rowers were excluded because their training involves different weight-bearing activities. Exclusion criteria included aetiologies other than endurance training causing oligo-amenorrhoea (e.g., pregnancy, primary ovarian insufficiency, hyperprolactinaemia, thyroid dysfunction and polycystic ovarian syndrome) and conditions affecting bone metabolism (e.g., diabetes, pituitary, renal or gastrointestinal disease). Individuals using medications affecting bone (e.g., oestrogen, progesterone, anabolic steroids and glucocorticoids) were also excluded. If randomised to oestrogen and progesterone, exclusion criteria included complex migraines, first-degree relatives with breast or other oestrogen-dependent cancers and family/personal history of conditions increasing thromboembolic risk. Participants were recruited through Institutional Review Board (IRB)-approved (A) fliers sent to paediatricians, internists, adolescent and sports medicine physicians, paediatric and adult endocrinologists and dietitians in the greater Boston area, posted at medical clinics and study recruitment sites within Harvard-affiliated hospitals, distributed during local high school and collegiate sporting events (e.g., Commonwealth Games and events at Reggie Lewis Track and Athletic Center) and posted around college campuses and neighbourhood businesses; (B) email notifications to coaches affiliated with area colleges; and (C) postings on collegiate job sites. We attempted to reach adolescent/young adult athlete and non-athlete populations representative of the general population of athletes/non-athletes. The study was approved by our IRB. Informed consent was obtained from subjects aged ≥18 years and parents of subjects aged <18 years, and informed assent from subjects aged <18 years.
Experimental protocol
A complete history, including exercise habits, was obtained. Height was measured on a wall-mounted stadiometer to the nearest millimetre, weight on an electronic scale to the nearest 0.1 kg, and pubertal (Tanner) stage assessed. A wrist/hand radiograph was used to determine bone age. Subjects completed the Bouchard 3-day activity record,14 eating disorder questionnaires (Eating Disorder Inventory-215 and Three-Factor Eating Questionnaire-R18),16 a 4-day food diary, indirect calorimetry for resting energy expenditure17 and had fasting morning blood drawn for 25(OH)vitamin D, calcium, parathyroid hormone (PTH), estradiol, sex hormone-binding globulin (SHBG), IGF-1, procollagen type 1 N-terminal propeptide (P1NP) and N-telopeptide (NTX). Dual-energy X-ray absorptiometry (DXA) was used to assess lumbar spine, femoral neck, total hip and total body less head (TBLH) bone mineral content (BMC) and areal BMD, lean and fat mass. DXA scans used the same instrument and scanning software (Hologic QDR-Discovery A, Apex software V.13.3; Waltham, Massachusetts, USA). Coefficients of variation (CVs) for areal BMD, fat and lean mass are 0.8%–1.1%, 2.1% and 1.0%, respectively.
One hundred and twenty-one eligible OAAs were randomised to one of three arms: (i) PATCH: physiological oestrogen replacement via 100 mcg transdermal 17β-E2 applied twice weekly and cyclic micronised progesterone (200 mg) for 12 days each month, (2) PILL: a COC containing 30 µg ethinyl estradiol with 0.15 mg desogestrel18 or (3) NONE: no oestrogen or progesterone. All received ≥1200 mg elemental calcium and 800 IU vitamin D daily. Subjects were reminded that PATCH was not a form of contraception and counselled on non-hormonal options. DXA scans and estradiol, SHBG, IGF-1, PINP and NTX levels were repeated at 6 and 12 months.19 Subjects with spontaneous menses in the NONE group were scheduled for visits within 10 days of menses onset for consistency, given variations in estradiol and bone turnover markers across the menstrual cycle. In this group, 64.3% and 17.9% of subjects at the 6-month visit, and 62.5% and 25.0% at the 12-month visit reported spontaneous irregular or monthly menses, respectively. Subjects were asked to inform study staff when menses began to time visits accordingly. Although visits included DXA scans and blood draws, the timing was relevant in the context of laboratory testing only. Menses in the PATCH and PILL groups were induced by study medications, with only minimal fluctuations expected in biochemical endpoints over time. Interviews, calendars, questionnaires and medication containers helped assess compliance and adverse effects.
Biochemical analysis
An electrochemiluminescence immunoassay was used to measure PTH (sensitivity 6.0 pg/mL; intra-assay CV 0.9%–3.0%), 17β-E2 (sensitivity 25.0 pg/mL; intra-assay CV 1.2%–6.7%) and SHBG (2.00 nmol/L; intra-assay CV 1.1%–1.7%) at LabCorp. An immunochemiluminometric assay was used to measure 25(OH)vitamin D (Labcorp; sensitivity 4.0 ng/mL; intra-assay CV 4.8%–7.7%), a radioimmunoassay to measure P1NP (Orion Diagnostics, Espoo, Finland; sensitivity 2.0 ng/mL; intra-assay CV 6.5%–10.2%) and an ELISA to measure NTX (LabCorp; sensitivity 3.2 nmol BCE/L; intra-assay CV 11.9%–14.0%). Mass spectrometry was used to measure IGF-1 (Quest Diagnostics, San Juan Capistrano, California, USA; sensitivity 15.6 ng/mL; intra-assay CV 3.5%–15%).
Statistical methods
We used SAS and JMP V.13.0 for analyses and report data as means±SEM or median (IQR). Baseline characteristics were compared using overall analysis of variance (ANOVA). An intention-to-treat (ITT) population-based analysis included all randomised participants in the longitudinal linear mixed effects model to determine whether PATCH performed better than PILL or NONE in improving BMD. Completers secondary analyses was performed.
Our primary endpoint was the prospective change in spine BMD Z-scores in PATCH versus PILL and NONE. Linearity of longitudinal response over time from individual subjects held. Areal BMC, BMD, and Z-scores were analysed by a mixed model ANOVA. We assumed each subject had a different linear trajectory and tested that the mean trajectory was different in PATCH versus PILL and NONE. For completers analyses, we compared changes in bone measures in PATCH versus PILL and NONE at 6 and 12 months, using a general linear model. All outcomes were compared among the three groups using Fisher’s least significant difference test, controlling for known determinants of prospective BMD changes (age, height, race, ethnicity and weight changes); if overall p values between groups were <0.05, pairwise comparisons were performed. Further adjustment for multiple comparisons was unnecessary because of preliminary significance testing with three groups.20
The relative protective effect of PATCH and PILL versus NONE (2.5% increase in BMD) was measured by the adjusted ORs, with Wald 95% CIs, controlling for effects of age, race, ethnicity, height and weight change using multivariable logistic regression models. Pearson or Spearman correlations were used to determine associations of changes in levels of bone markers and BMD with changes in estradiol, SHBG and IGF-1. Regression modelling determined independent predictors of BMD changes after controlling for covariates. Fisher’s exact test was used to compare proportions in PATCH, PILL or NONE groups for reported adverse effects.
Patient involvement
Patients were not involved in development of the research question, outcome measures, study design, or assessment of the burden of intervention. We did encourage participants to inform their peers about the study and its purpose to facilitate recruitment. We will send the main study paper to study participants once the data are published.
Results
Baseline characteristics
Baseline characteristics did not differ among randomisation groups (table 1), nor for study completers versus non-completers (data not shown). Of 121 randomised subjects, 73 completed the study (figure 1), with 70% and 60% completers at 6 months and 12 months, respectively. Groups did not differ for attrition rates, nor 12 month changes in weight, BMI, fat and lean mass (table 4).

Numbers of oligo-amenorrhoeic athletes (OAAs) recruited for the study and attrition over the 12-month study duration in the three randomisation groups (PATCH, PILL and NONE). COCs, combined oral contraceptives.
Baseline clinical characteristics of oligo-amenorrhoeic athletes (OAAa) randomised to PATCH, PILL, or NONE groups
Changes in DXA measures over 6 and 12 months
Data for ITT analysis are shown in online supplementary table 1. At the spine, BMC, BMD and BMD Z-scores significantly increased in PATCH compared with PILL, and BMD Z-scores increased in PATCH versus NONE. At the femoral neck, BMD and BMD Z-scores increased in PATCH versus PILL, and BMD Z-scores in PATCH versus NONE. At the total hip, BMC, BMD and BMD Z-scores increased in PATCH versus PILL, and BMD in NONE versus PILL.
Supplemental material
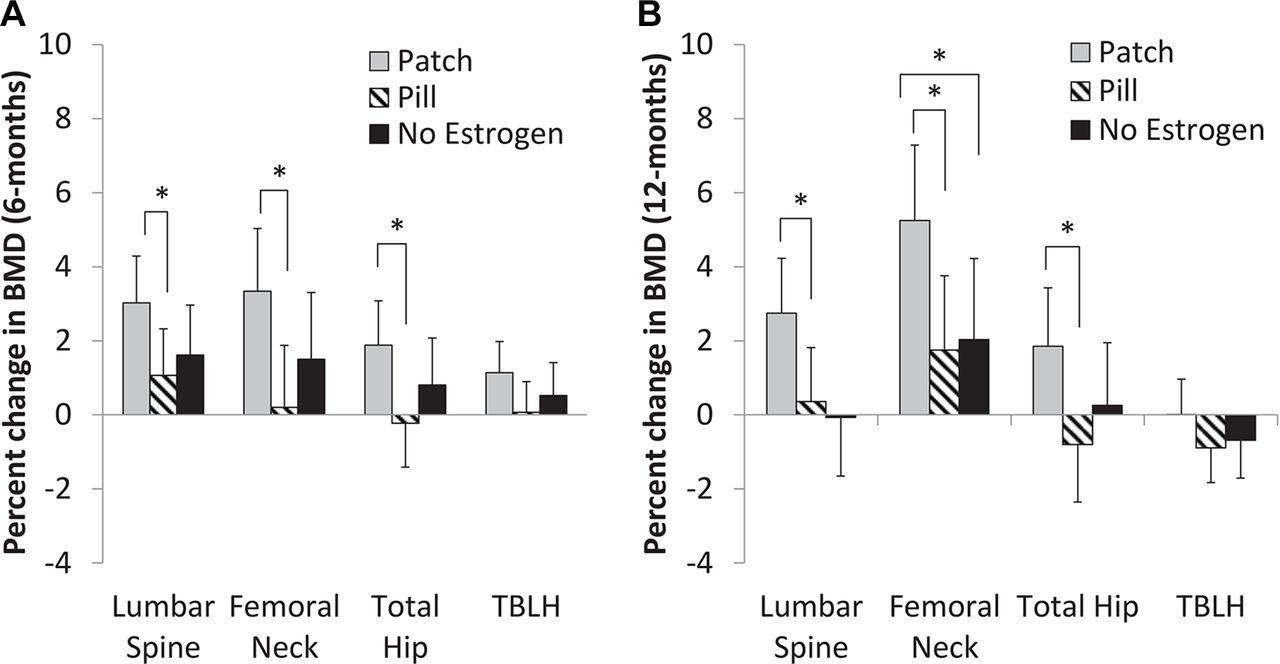
Differences among completers for absolute changes in BMC, BMD and BMD Z-scores are shown in table 2, and percent BMD changes are shown in figure 2A,B. At 12 months, at the spine, PATCH demonstrated greater increases in BMC, BMD and percent change in BMD than PILL, and in BMC, BMD, BMD Z-score and percent change in BMD than NONE. At the femoral neck and total hip, PATCH versus PILL demonstrated greater increases in BMD and percent change in BMD. PATCH versus NONE demonstrated increases in BMD, BMD Z-scores and percent change in BMD at the femoral neck, but not the total hip. Twelve-month completers in PATCH had a BMD increase of 2.75%, 5.25% and 1.85% at the spine, femoral neck and total hip, respectively.
{kind=link}
{kind=link}
Percent change in bone mineral density (BMD) in completers at 6 months (A) and 12 months (B). TBLH, total body less head. *Significant at p<0.05.
Six-month and 12-month changes in DXA bone parameters in completers randomised to the PATCH, PILL or NONE (controlled for age, height, race and ethnicity)
The adjusted ORs [95% CI; p-value] for a protective effect of PATCH vs. NONE on BMD (defined as >2.5% increase in BMD) were 11.22 (2.12–59.29; P=0.008], 10.76 (2.07–55.98; P=0.001], 6.27 (0.97–40.32; P=0.011], and 1.44 (0.19–10.76; P=0.292] for the spine, femoral neck, total hip, and TBLH, respectively, controlling for age, height, race, ethnicity, and weight change. The PILL was not protective at any site.
Changes in biochemical parameters over 6 months and 12 months
Table 3 shows changes in biochemical parameters for completers at 6 months and 12 months. Online supplementary table 2 shows the mixed effects model ITT and completers analysis of the effect of PATCH versus PILL versus NONE on biochemical parameters. IGF-1 and P1NP decreased over the study duration in PILL compared with PATCH and PILL compared with NONE. Changes in P1NP over 12 months were positively associated with changes in estradiol (r=0.35, p=0.004) and IGF-1 (r=0.37, p=0.003), and inversely with changes in SHBG (r=−0.28, p=0.019). In a regression model including changes in estradiol, IGF-1 and SHBG, changes in IGF-1 remained associated with changes in P1NP (β-estimate 0.161, p=0.016), whereas other associations were lost. For changes in BMD over time, changes in estradiol were associated with changes in femoral neck, spine and hip BMD at 12 months (r≥0.27, p≤0.024). Changes in DXA measures were not associated with changes in IGF-1 or SHBG.
Six-month and 12-month changes in biochemical parameters in completers randomised to PATCH, PILL or NONE
Measures of compliance and adverse events
Estradiol increased more in PATCH versus PILL and NONE at 6 months and 12 months. SHBG increased in PILL versus PATCH and NONE (table 3, online supplementary table 2). This suggests more bioavailable estradiol in PATCH versus PILL and NONE, and good compliance with study drugs in PATCH and PILL groups (based on changes in estradiol and SHBG, respectively). Online supplementary table 3 reports adverse events and illustrates no differences among groups.
Discussion
While many practitioners prescribe COCs as a treatment for menstrual disturbances in OAA, this is the first study to compare, head-to-head, effects of transdermal 17β-E2 replacement in physiological doses (with cyclic progesterone) versus COC on bone outcomes in normal-weight OAA, a population at high risk for stress fractures from overuse and hormonal suppression.2 6 This is also the first study to demonstrate that physiological 17β-E2 replacement performed better than COC in improving BMD in OAA, particularly at the spine and femoral neck, while women receiving COC fared worse than those receiving no oestrogen at the total hip.
This supports our findings in adolescents with AN, an illness associated with severely decreased energy availability, where we demonstrated increases in spine and hip BMD over 18 months using transdermal 17β-E2 and cyclic progesterone compared with placebo.11 There was no PILL group, but bone accrual in the PATCH group approximated bone accrual in eumenorrhoeic controls.11 Specifically, spine BMD increased 2.5% at 12 months in PATCH compared with a decrease of 0.1% with placebo. Our current findings over 12 months in a less nutritionally restricted, overall normal-weight population indicate a 2.7% increase in spine BMD in PATCH versus an increase of 0.4% in PILL, and a decrease of 0.1% in NONE. Thus, our findings in a normal-weight hypoestrogenic group are similar to those reported in an underweight hypoestrogenic group over the same duration. In the current study, we did not find differences in hip BMD in PATCH versus NONE at 12 months in OAA, consistent with the AN study, where small differences in hip BMD were evident only at 18 months. This is possibly explained by the greater trabecular content of the spine versus total hip and greater antiresorptive effects of oestrogen at primarily trabecular sites.21
Possible explanations for our findings are:
Transdermal 17β-E2 does not undergo hepatic first-pass metabolism or suppress IGF-1, a bone-trophic hormone downregulated by COCs.22 Consistent with this, PILL had greater reductions in IGF-1 and P1NP than PATCH and NONE groups. Changes in IGF-1 were associated with changes in P1NP even after controlling for covariates.
Ethinyl estradiol (in COCs) has a dose-dependent stimulatory effect on hepatic SHBG production.23 24 We were able to use this effect as a marker of compliance in the PILL group. Higher SHBG may lower bioavailable estradiol.25 Changes in SHBG were inversely associated with changes in P1NP; these associations were lost in a multivariate model.
We selected a generic COC formulation for this study (30 µg ethinyl estradiol, 0.15 mg desogestrel), rather than a lower oestrogen dose. This COC resulted in a decrease in serum estradiol at 6 months and 12 months compared with baseline and compared with PATCH, which had an increase in estradiol at both time points versus baseline. The PILL group also had lower estradiol at 6 months and 12 months versus NONE, consistent with our assay measuring 17β-E2, and not ethinyl estradiol, the oestrogen in the COC. 17β-E2 may be more effective than ethinyl estradiol in preventing bone resorption. However, premenopausal women receiving a COC containing 17β-E2 and nomegestrol acetate versus a COC containing ethinyl estradiol/levonorgestrel for 2 years did not differ for bone outcomes.26 We found significant associations of changes in estradiol with changes in P1NP and BMD.
It is unclear whether a COC with a lower ethinyl estradiol dose (10–20 µg) would be less detrimental to bone by minimising increases in SHBG. Data regarding the impact of ethinyl estradiol dose on bone are conflicting. One study showed a trend for lower BMD with lower doses and longer duration of use in young women,27 while another found lower BMD with 15 versus 30 µg ethinyl estradiol COC formulations in adolescents.28 Other studies have not demonstrated a difference in BMD based on ethinyl estradiol dose.29 30
The COC group used the standard prescription of 21 days of active and 7 days of placebo pills, whereas the PATCH group received 17β-E2 continuously. Over 12 months, this led to greater oestrogen exposure in the latter group, possibly impacting outcomes more favourably. However, decrements in total hip BMD suggest a deleterious effect of COCs on bone, possibly more marked with continuous use of active pills. Furthermore, continuous use of active pills may have caused greater and sustained SHBG elevations.
Standard treatments for AN and Triad focus on increasing energy availability and weight restoration to improve menstrual function and BMD.1 31 32 However, patient resistance to behavioural changes can delay the process, possibly increasing short-term and long-term risk for fractures. Athletes often feel pressured to maintain very low body fat because of sports performance misconceptions and coach and societal pressures.33 34 Educating and convincing an athlete to improve his or her hormonal milieu by improving energy balance, modifying body composition and resuming menses can be a long process. This study (and our previous AN study)11 suggests that physiological transdermal 17β-E2 with cyclic progesterone may be an adjunct treatment for young women with hypothalamic oligo-amenorrhoea to improve BMD while simultaneously improving energy availability.
Limitations
Attrition was considerable, though comparable with studies in similar populations.11 35 However, differences between groups were similar in our completers and ITT analyses. Repeated attempts to contact study dropouts were made. Dropouts seemed primarily related to subjects’ (mostly scholastic and collegiate athletes) busy schedules and rarely due to treatment effects. Notably, side effects did not differ among groups. We tested one dose of the 17β-E2 patch and one dose and type of COC, limiting generalisability of our results. Importantly, estradiol levels in the PATCH group were in the range used for replacement therapy, suggesting appropriateness of the dose. Also, we used a COC with a commonly prescribed ethinyl estradiol dose,36 intended to be representative of COC use in the general population. Further research is needed to: (1) compare other COC formulations (including oral 17β-E2), (2) determine the possible role of progesterone on bone endpoints, and (3) understand if BMD improvements through use of transdermal estradiol correlate with a reduction of bone stress injury in OAA.
Conclusion
This study has many strengths. Subjects were limited to endurance, weight-bearing OAA who met stringent activity type and volume criteria, in an attempt to limit confounding lifestyle factors. We carefully monitored compliance, side effects and treatment effects at multiple time points. Study length and time commitment may have contributed to greater attrition, but also provided multiple ways to detect possible treatment effects on bone parameters. This is the first study to demonstrate that transdermal 17β-E2 is superior to both no treatment and a typical COC in improving bone outcomes in OAA, particularly spine and femoral neck BMD. While oligo-amenorrhoea should be treated with an interdisciplinary team using a biopsychosocial approach, and addressing energy availability and lifestyle remains the first line of management, transdermal 17β-E2 may be a therapeutic adjunct to optimise bone accrual, particularly during critical adolescent and young adult years.
Six-month and 12-month changes in BMI and body weight, and data for reported menstrual history in completers randomised to PATCH, PILL or NONE
Acknowledgments
We would like to thank our subjects who participated in this study and our funding sources: NIH grants R0I HD060827, K24 HD071843 and UL1TR001102 and S10 RR023045.
References
Footnotes
Contributors MM conceived the project and designed the study. MM, KEA and MLB contributed to study protocol and key data interpretation. KEA, MM, VS, CB, MS, KJCR, AT and KE were involved in patient assessments, visits and study coordination. HL and MM performed the statistical analysis. KEA wrote the initial draft of the paper. MM, KEA, MLB, HL and AK critically edited and revised the paper.
Funding This study was funded by National Institutes of Health grants R0I HD060827, K24 HD071843 and UL1TR001102 and S10 RR023045.
Competing interests MM has served on the Scientific Advisory Board of Novo Nordisk, is a coinvestigator on an investigator-initiated grant from Novo Nordisk and is a consultant for Sanofi Pharmaceuticals.
Patient consent Obtained.
Ethics approval Massachusetts General Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement These data have not been previously published and are original data. In addition, no other entity has permission to use these data.
Correction notice This article has been corrected since it published Online First. The patient consent statement has been corrected.