Article Text

Abstract
Objectives Cam morphology is not completely understood. The aim of this study was threefold: (1) to investigate if cam morphology development is associated with growth plate status; (2) to examine whether cam morphology continues to develop after growth plate closure; and (3) to qualitatively describe cam morphology development over 5-year follow-up.
Methods Academy male football players (n=49) participated in this prospective 5-year follow-up study (baseline 12–19 years old). Anteroposterior and frog-leg lateral views were obtained at baseline (142 hips), 2.5-year (126 hips) and 5-year follow-up (98 hips). Cam morphology on these time points was defined as: (A) visual scores of the anterior head-neck junction, classified as: (1) normal, (2) flattening, and (3) prominence; and (B) alpha angle ≥60°. Proximal femoral growth plates were classified as open or closed. Cam morphology development was defined as every increase in visual score and/or increase in alpha angle from <60° to ≥60°, between two time points. This resulted in 224 measurements for cam morphology development analysis.
Results Cam morphology development was significantly associated with open growth plates based on visual score (OR: 10.03, 95% CI 3.49 to 28.84, p<0.001) and alpha angle (OR: 2.85, 95% CI 1.18 to 6.88, p=0.020). With both definitions combined, cam developed in 104 of 142 hips during follow-up. Of these 104 hips, cam developed in 86 hips (82.7%) with open growth plate and in 18 hips (17.3%) with a closed growth plate. Cam morphology developed from 12 to 13 years of age until growth plate closure around 18 years.
Conclusion Cam morphology of the hip is more likely to develop with an open growth plate.
- FAI syndrome
- cam morphology
- growth plate
- hip
- football
Statistics from Altmetric.com
Introduction
Femoroacetabular impingement syndrome is a symptomatic motion-related disorder resulting from a premature contact between the proximal femur and acetabulum.1 This is often due to pincer and/or cam morphology. Cam morphology is characterised by extra bone formation mostly located in the anterolateral head-neck junction, which can be forced into the acetabulum during hip flexion and internal rotation. In general, cam morphology does not necessarily lead to symptoms, but has a strong relationship with reduced function and future hip osteoarthritis.2–7
The aetiology of cam morphology is not fully understood. It is more prevalent in athletes than in non-athletes,8 9 with prevalence reported above 60% in high-impact sports such as football,8 10–13 basketball9 and ice hockey.14–16 Finite element analysis revealed that repetitive movements of deep flexion and external rotation in hips with an open growth plate are possible triggers for extra bone formation in the anterolateral head-neck junction.17 Cam morphology is first visible on radiographs from the age of 12 to 13 years and gradually increases in size during skeletal growth.8 9 18 During this prepubertal phase, bone is more responsive to loading. This might be due to nutrients, sex steroids, growth hormone peaks, insulin-like growth factors and genetic factors.19 Bone is likely to change to meet the demands of mechanical loading during childhood.20 Interestingly, cam morphology typically develops at the location where the growth plate extends into the femoral neck.10 Data from the 2.5-year follow-up of the current cohort suggested that cam morphology might only develop when the growth plate is open, but only a small number of hips had closed growth plates at 2.5-year follow-up.10 If this observation proves correct, interventions to prevent cam morphology development are probably only useful during skeletal growth. To the best of our knowledge, no other prospective follow-up data are available on this topic.
This study aimed to assess the association between growth plate status and future cam morphology development during a minimum of 5 years’ follow-up, to investigate if cam morphology continues to develop after proximal femoral growth plate closure, and to qualitatively describe cam morphology development in this 5-year time period.
Methods
Participants
All 89 academy male football players of Feyenoord Rotterdam (the Netherlands) who attended at baseline were invited to participate again and 49 of 89 (55.1%) joined this 5-year follow-up study. The football players were aged between 12 and 19 years at baseline. Recruitment for 5-year follow-up took place between June and October 2015. Inclusion criteria for the initial inclusion were playing in selection teams of Feyenoord Rotterdam (the Netherlands). Exclusion criteria were any hip disorder.8 10 Each participant gave written consent. For individuals younger than 18 years, written consent was also obtained from at least one parent.
Radiographs
The standardised radiographic protocol used for this 5-year follow-up was the same as at baseline and 2.5-year follow-up.8 10 In short, three radiographs of the hip were obtained: a standardised anteroposterior (AP) view of the pelvis and a frog-leg lateral view of each hip. Using these projections we were able to examine the lateral (on AP view) and anterosuperior (on frog-leg lateral view) femoral head-neck junction to detect cam morphology. For the AP view, 15° internal rotation was ensured by positioning the participant supine with his feet in a special frame. For the frog-leg lateral view, the participant was placed in the supine position with the hip in flexion and abduction, using a 45° wedge under the knee to secure standardised position.
Visual scores
The anterolateral head-neck junction in all radiographs was semiquantitatively scored (ordinal variable) as: (1) normal, (2) flattening or (3) prominence.
Normal: slight symmetric concavities of the anterior head-neck junction with respect to the posterior head-neck junction.
Flattening: moderate decrease in the anterior head-neck offset with respect to the posterior head-neck junction.
Prominence: convexity in the anterior head-neck junction, as opposed to a concavity.
Cam morphology was defined as the presence of either a flattening or prominence of the proximal femur. An experienced orthopaedic surgeon and musculoskeletal radiologist determined the visual scores of all hips, based on consensus. Each hip was scored with the available radiographs of all three time points in one session. The visual scores showed a kappa of 0.68 for intraobserver reliability in the baseline study.8
Alpha angle
The proximal femoral shape was outlined by a set of points that were manually positioned on anatomical landmarks using Statistical Shape Modelling software (ASM toolkit, Manchester University, Manchester, UK). Images of left-sided joints were mirrored to appear as right-sided joints. Using MATLAB V.7.1.0 (MathWorks, Natick, Massachusetts, USA), the alpha angle was automatically calculated in all radiographs from a set of points that were manually positioned on predefined anatomical landmarks of the proximal femur.8 10 An alpha angle ≥60° was defined as cam morphology.21 The highest alpha angle value on the AP or frog-leg lateral views of each hip was used for analysis. When a hip had an alpha angle ≥60° at a certain point, we defined this hip as having cam morphology at the subsequent follow-up time point as well. For alpha angle, the intraclass correlation coefficient (ICC) for interobserver reliability was 0.73. Intraobserver reliability ICC ranged from 0.85 to 0.99.6 The measurement error is calculated by the root mean square error (RMSE). This resulted in an RMSE between 1.68 and 1.99.6
Growth plate status
The growth plate status (open or closed) was scored at the same time, based on consensus. The growth plate was scored as closed, if the full growth plate was totally fused and visible as a sclerotic line. If only a small part of the growth plate remained open in any radiographic view, that growth plate was scored as open. Growth plate status was scored in 126 radiographs during 2.5-year follow-up, and those radiographs were scored again during 5-year follow-up, resulting in a kappa of 0.94 for intraobserver reliability.
Definition of cam morphology development
Every increase in visual scores (dichotomous scale) and/or increase of alpha angle from <60° to ≥60° (dichotomous scale) was defined as cam morphology development. As presented in figure 1, we assessed the development of cam morphology by pairwise comparison between baseline and 2.5-year follow-up (63 participants, 126 hips), between baseline and 5-year follow-up, if participants did not attend the 2.5-year follow-up (8 participants, 16 hips), and between 2.5-year follow-up and 5-year follow-up (41 participants, 82 hips). This resulted in a total of 224 different pairwise comparisons.

Flow chart of all analysed participants at baseline, 2.5-year follow-up and 5-year follow-up. Note: Temporary dropouts are dropouts which did not attend at 2.5-year follow-up. Definitive dropouts are dropouts who were not included in the next time point. Cam morphology development was measured between baseline and 2.5 years’ follow-up (n=126), between 2.5-year follow-up and 5-year follow-up (n=82), and between baseline and 5-year follow-up in case participants who did participate at 5-year follow-up but not at 2.5-year follow-up (n=16). This resulted in 224 measurements of cam morphology development.
Statistical analysis
Differences in baseline characteristics between included participants and dropouts were tested using an independent samples t-test. Cam morphology prevalence was described per hip. Development of cam morphology is analysed blinded on hips of participants who attended at least two time points. This resulted in radiographs of 142 hips at baseline, 126 hips at 2.5-year follow-up, and 82 and 16 hips at 5-year follow-up (figure 1). Cam morphology development was analysed twice (for visual score and alpha angle) in 224 radiographs, which included repeated measurements. Growth plate status is presented in 71 persons (142 hips). The association between growth plate status and cam morphology development was calculated by means of logistic regression. By using logistic regression in a ‘Generalized Estimated Equations’ model, we were able to take into account the correlation that exists within a person regarding follow-up time and side. A sensitivity analysis was performed to see if defining hips with alpha angle <60° as cam morphology, when a previous time point had alpha angle ≥60°, affected the results (online supplementary table 1). The statistical evaluation was performed using SPSS V.21.0 (Windows).
Supplementary file 1
Results
Patient characteristics
Demographic data are presented in table 1. The mean follow-up time was 5.3±0.1 years (range 5.0–5.6 years). In total, 224 radiographs were analysed in 71 different football players with multiple time points (figure 1). Of 89 participants at baseline, 40 did not participate at 5-year follow-up (44.9%). Of these 40 participants, 24 rejected the invitation, 4 were playing football abroad, 11 were unreachable and 1 did not show up. At 5-year follow-up, all 49 participants were still playing football. Of those 49 participants, 28 (57.1%) were still active in the first or second team or youth academy of a professional football club. The remaining 21 players (42.9%) were active at an amateur football level. There were no significant differences in baseline demographic data between the 49 participants who attended the 5-year follow-up and the dropouts (table 2).
Demographic data of baseline, 2.5-year follow-up and 5-year follow-up
Demographic baseline data of 5-year follow-up participants compared with dropouts
Cam morphology prevalence
Cam morphology based on visual scores was found in 77 of 142 hips (54.2%, 35 left and 42 right) at baseline, in 99 of 126 hips (78.6%, 47 left and 52 right) at 2.5-year follow-up and in 80 of 98 hips (81.6%, 39 left and 41 right) at 5-year follow-up. Cam morphology based on alpha angle was found in 70 of 142 hips (49.3%, 31 left and 39 right) at baseline, in 86 of 126 hips (68.3%, 42 left and 44 right) at 2.5-year follow-up and in 78 of 98 hips (79.6%, 37 left and 41 right) at 5-year follow-up. The highest visual scores and alpha angles were mostly (ranging from 90.1% to 94.5% during follow-up) found on frog-leg lateral views compared with AP views during follow-up.
Growth plate status
In total, 42 of 142 (29.6%) growth plates were closed at baseline, 72 of 126 (57.1%) at 2.5-year follow-up and 92 of 98 (93.9%) at 5-year follow-up.
Association between cam morphology development and growth plate status
Cam morphology development based on visual scores was observed in 80 of 142 (56.3%) hips. Of these 80 hips, 14 had development from normal to flattening and from flattening to prominence during follow-up. Of these 80 hips, 71 had an open and nine had a closed growth plate. This resulted in a strong association between cam morphology development based on visual scores and open growth plate status (OR: 10.03, 95% CI 3.49 to 28.84, p<0.001), as portrayed in figure 2. Cam morphology development based on alpha angle was observed in 43 of 142 (30.3%) hips. Of these 43 hips, 34 had an open and nine had a closed growth plate. This resulted in a significant association between cam morphology development based on alpha angle and open growth plate status (OR: 2.85, 95% CI 1.18 to 6.88, p=0.020). Of the hips with a closed growth plate that developed cam morphology, seven were only classified by the visual score, eight only by the alpha angle and one was classified as development of cam morphology after growth plate closure by both the visual score and the alpha angle. This resulted in 16 hips (11.3%, in 10 persons) with a closed growth plate that developed cam morphology by either the visual score and/or the alpha angle.

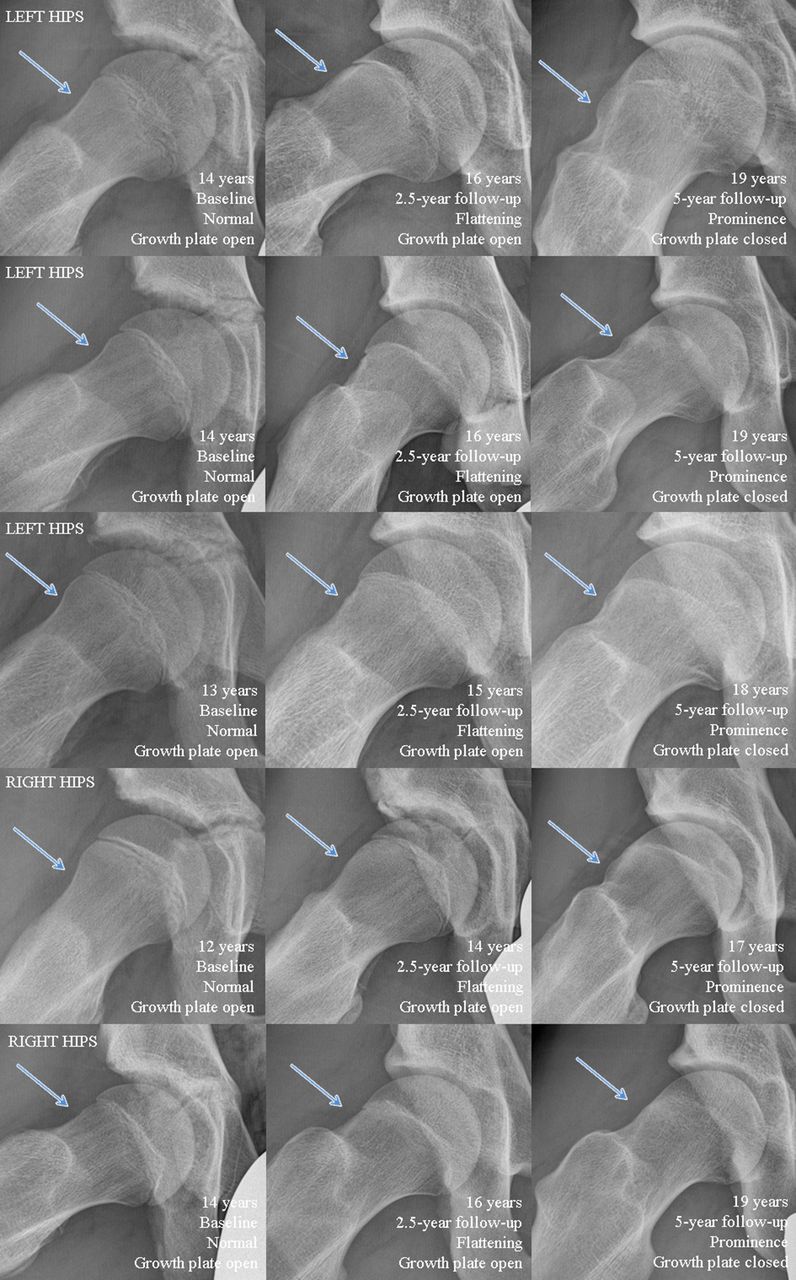
Cam morphology development based on visual scores during follow-up in five different hips of five persons on frog-leg lateral radiographs. Note: In all presented hips, cam morphology development based on visual score from baseline to 2.5-year follow-up, and from 2.5-year follow-up to 5-year follow-up, is observed.
Qualitative description of cam morphology
Some anatomical changes not captured in quantifiable measures were observed during follow-up. In this study, a normal spherical anterolateral head-neck junction of the hip joint based on visual scoring was found in almost all (83.3%) 12-year-old boys. From around the age of 12 to 13 years, the first appearances of cam morphology became visible. Development of cam morphology can be observed via a change in the anterolateral head-neck junction, resulting in extra bone formation in that region. This extra bone formation gradually increased during growth until the age of around 18 years. Cam morphology development is demonstrated in several hips in figure 2. Together with cam morphology development, the lateral side of the growth plate was positioned more distally, appearing like an extension of the growth plate bending towards the greater trochanter. The site of this extension also corresponds with the location of bone where the cam morphology forms. In hips which did not develop cam morphology, the head-neck junction does not undergo major changes. In most cases (82.7%) cam morphology developed in hips with an open growth plate and also when a small part of the growth plate remained open. Conversely, cam morphology development was also observed in 16 different hips with a closed growth plate. Of these 16 hips, 14 had signs of external hip rotation per time point on the radiographic projection during follow-up. These differences in hip rotation could be observed via the differences in projection of the greater trochanter over the neck and the appearance of the lesser trochanter (figure 3). During follow-up, two hips (in one person), with a closed growth plate status, showed cam morphology development without signs of rotation differences (figure 4). These two hips followed the outlined pattern of cam morphology development, more similar to cam morphology development when the growth plate is open.
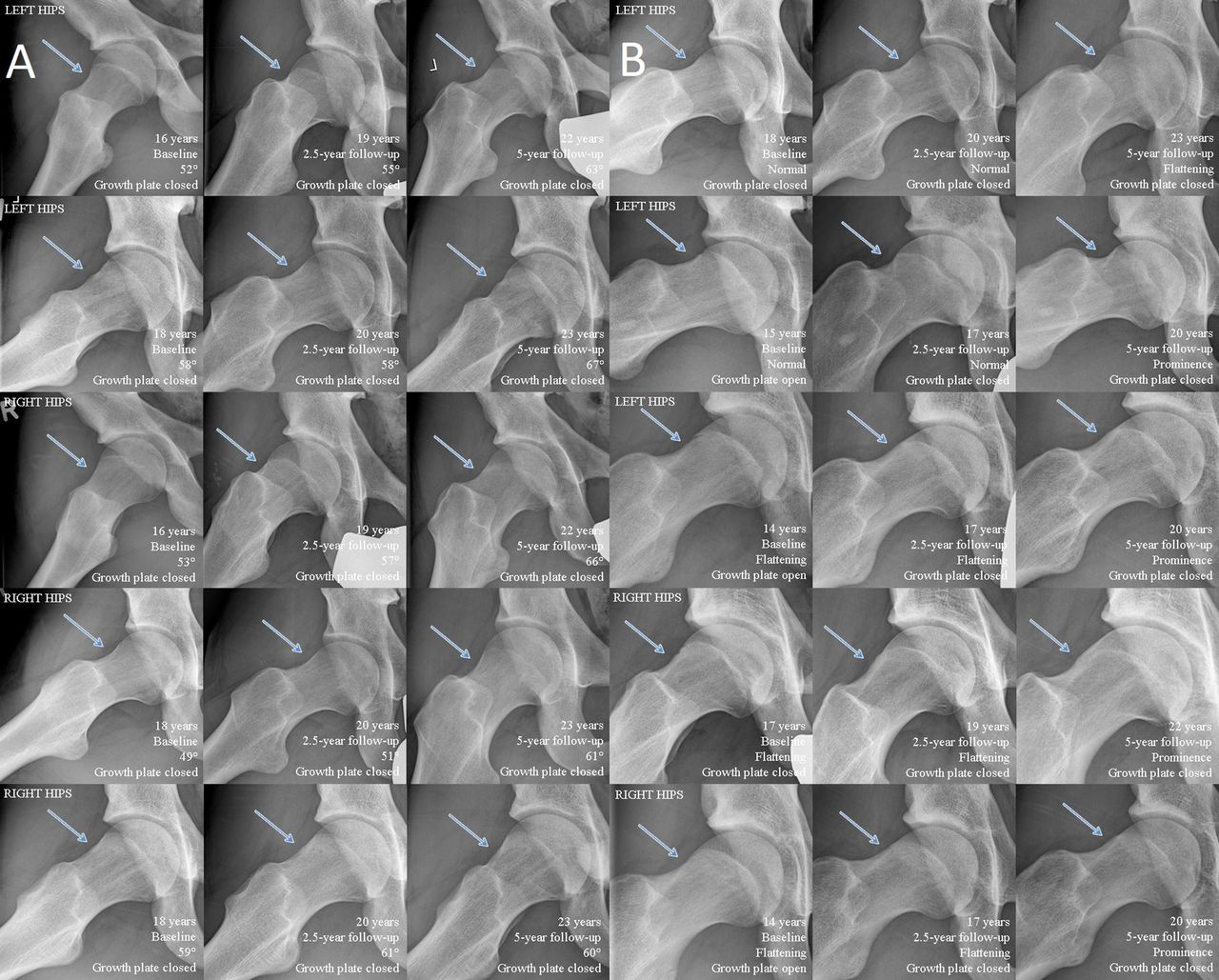
Cam morphology development (based on alpha angle (A) and visual score (B)) possibly caused by hip rotation (visible via greater trochanter projection) on frog-leg lateral radiographs. (A) Besides differences in rotation, the alpha angle increased with ≤10° from 2.5-year follow-up to 5-year follow-up in these hips. (B) Very subtle change in visual score was observed at 5-year follow-up while the femoral head-neck junction was normal or flattened at baseline and 2.5-year follow-up. This change in visual score is possibly due to the slight difference in rotation during the follow-up times.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cam morphology development based on alpha angle and visual score on frog-leg lateral radiographs of one person during follow-up. All presented hips have closed growth plates. Note: From baseline (normal or flattening) to 2.5-year follow-up (flattening) and from 2.5-year follow-up to 5-year follow-up (prominence), cam morphology development is observed. Cam morphology development based on alpha angle is noticed in the right hip from 2.5-year follow-up (53°) to 5-year follow-up (70°).
Discussion
Cam morphology development was strongly associated with growth plate status in this study, which represents the 5-year follow-up data of a cohort with football players. Gradual formation of additional bone at the femoral head-neck junction that ultimately forms cam morphology is mainly observed in participants with an open proximal femoral growth plate. After the growth plate closed, we observed no or little cam morphology development. Due to the prospective design of this study we were able to investigate cam morphology development throughout adolescence and young adulthood, with a sufficient follow-up of hips with closed growth plates.
Aetiology and prevention
The aetiology of cam morphology development is not fully understood. Our results show that cam morphology develops almost exclusively during growth. Cam morphology development is first observed from an age of 12 to 13 years and the prevalence substantially increased during growth. A recent study by Palmer et al 18 investigated cam morphology development in 103 professional male football players and 107 age-matched controls (52 male and 55 female). Corresponding with our results, they found that cam morphology first developed between 12 and 14 years of age. The likely explanation for cam morphology development around this age could be that the skeleton is highly responsive to mechanical loading during this period of growth.19 20 Formation of cam morphology is probably triggered by high-impact sports, providing the potential for the implementation of preventative strategies. A dose–response relationship on training frequency in football players is described previously.18 22 A training schedule with lower impact sports could therefore be a theoretical option to prevent development of cam morphology. A personalised schedule adapted to an individual’s safe activity threshold, training frequency and intensity can be implemented. However, to date, the influence of low-impact sporting activities on cam morphology development is not exactly known and advice regarding preventive strategies for cam morphology remains premature.
Cam morphology development after growth plate closure
Cam morphology development after growth plate closure was found in eight hips based on visual score and nine hips based on alpha angle. From six of eight hips scored by visual score and seven of nine hips scored by alpha angle, it was uncertain if cam morphology truly developed or whether it was quantified as such due to a slight different position of the radiographic view, despite the strict radiographic protocol (figure 3). Another explanation for cam morphology development after growth plate closure might be the use of radiographs instead of MRI. If the growth plate appears closed on a radiograph, it is unsure whether the growth plate is really closed or if there might still be growth potential. In only two hips of one person, development of cam morphology after growth plate closure was observed with certainty. These hips had nearly identical position on the radiographs at all time points (figure 4). These cam morphologies appear more sclerotic and this might possibly be a result of a bony response due to impingement, the shape of head-neck junction or acetabular shape, rather than an adaptive response to loading. This could possibly be explained by the fact that repetitive stimulation of cortical bone due to the impingement may be a stimulus for bone formation.
Limitations
Some limitations of this study need acknowledgement. A high dropout rate of 44.9% is observed during follow-up which potentially has introduced bias. However, baseline characteristics were not statistically different between included football players and dropouts (table 2). Results of this study in male football players might not automatically be generalised to female soccer players. Given that 6 of 98 growth plates were still open at 5-year follow-up, the prevalence is expected to even increase slightly. Another limitation is the use of radiographs leading to an underestimation of both cam morphology prevalence and amount of open growth plates. Differences in rotation of the hip, especially external rotation, could potentially have influenced the results, but due to the same standardised radiographic protocol used at every time point, this effect is likely limited.
Visual scores
Due to limitations of the alpha angle, the anterolateral head-neck junction was also semiquantitatively scored. All the available radiographs over time were presented and scored in one series, which could have introduced bias but also resulted in more reliable prospective visual scores. Bias could have been introduced because the observers were not blinded for growth plate status. However, by showing each hip of one person at the multiple follow-up times at once, the hips could be more reliably categorised into normal, flattening or prominence.
Alpha angle
Although the alpha angle is the most commonly used quantitative measure for cam morphology, this measure does have its limitations. First, the alpha angle might be less valid in hips with an open growth plate since it results in a higher rate of false positive findings, as described previously in this cohort and also observed by others.8 18 Another restriction is that the alpha angle, like every measurement method, has its measurement uncertainty. The values for the minimal detectable change are not available for the alpha angle. For example, of 43 hips that developed cam morphology based on alpha angle, 21 (48.8%) increased in alpha angle less than 10° and 9 (20.9%) of these 21 even less than 5°. This might very well be within the measurement uncertainty. It might therefore be possible that hips were misclassified as having or not having cam morphology. A dichotomous definition of cam morphology based on the alpha angle is used, with the risk of misclassifying hips that have alpha angles around 60°. Lastly, the risk of a false positive or false negative quantification of cam morphology is increased due to repetitive measurements during follow-up.
Conclusion
Cam morphology of the hip develops mainly when the growth plate is open in young male football players. This suggests that cam morphology is a bony adaptation resulting from stimulating of the growth plate by sporting activities, which has implications for possible future preventative measures for cam morphology formation.
What are the findings?
Cam morphology mainly develops when the proximal femoral growth plate is open.
Development of cam morphology after closure of the proximal femoral growth plate was very rare.
How might it impact on clinical practice in the future?
Possible interventions to prevent development of cam morphology might only be useful during skeletal growth.
Acknowledgments
The authors thank Raymond van Meenen, Rob Kurvers, Marcel de Geus and the other staff members of Feyenoord Football Academy for their collaboration in this study. This study would not have been possible without the study participants and their families, to whom we offer our sincerest gratitude.
References
Footnotes
Contributors PK, RA: study conception/design, data acquisition, data analysis and interpretation, drafting of manuscript. MPH, AZG: data acquisition, data interpretation, critical revision. JANV: study conception/design, data acquisition, critical revision. JHW: study conception/design, data acquisition, data analysis and interpretation, critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Approved by the Medical Ethical Committee of Erasmus Medical Centre, Rotterdam, the Netherlands (METC: 2009-235).
Provenance and peer review Not commissioned; externally peer reviewed.