Article Text

Abstract
Objectives We investigated the temporal trend and the geographical variation in the rate of an anterior cruciate ligament (ACL) reconstruction and meniscal repair (MR) performed in England during a 20-year window.
Methods All hospital episodes for patients undergoing ACL reconstruction or MR between 1 April 1997 and 31 March 2017 were extracted by procedure code from the national hospital episode statistics. Age-standardised and sex-standardised rates of surgery were calculated using Office for National Statistics population data as the denominator and analysed over time both nationally and regionally by National Health Service clinical commissioning group (CCG).
Results Between 1997–1998 and 2016–2017, there were 133 270 cases of ACL reconstruction (124 489 patients) and 42 651 cases of MR (41 120 patients) (isolated or simultaneous). Nationally, the rate of ACL reconstruction increased 12-fold from 2.0/100K population (95% CI 1.9 to 2.1) in 1997–1998 to 24.2/100K (95% CI 23.8 to 24.6) in 2016–2017. The rate of MR increased more than twofold from 3.0/100K (95% CI 2.8 to 3.1) in 1997–1998 to 7.3/100K (95% CI 7.1 to 7.5) in 2016–2017. Of these cases, the rate of simultaneous ACL reconstruction and MR was 2.6/100K (95% CI 2.5 to 2.8) in 2016/2017. In 2016–2017, for patients aged 20–29, the sex-standardised rate of ACL reconstruction was 76.9/100K (95% CI 74.9 to 78.9) and for MR was 19.8/100K (95% CI 18.8 to 20.9). Practice varied by region—in 2016–2017, 14.5% (30/207) of the CCGs performed more than twice the national average rate of ACL reconstruction and 15.0% (31/207) performed more than twice the national average rate of MR.
Conclusions The rate of ACL reconstruction (12-fold) and MR (2.4-fold) has increased in England over the last two decades. There is variation in these rates across geographical regions and further work is required to deliver standardised treatment guidance for appropriate use.
- knee
- arthroscopy
- meniscus
- anterior cruciate ligament
- ACL
Statistics from Altmetric.com
What are the findings?
Over the last two decades in England, the age-standardised and sex-standardised rate of anterior cruciate ligament reconstruction increased 12 times and meniscal repair increased 2.4 times.
There was variation in the rate of surgery by patient sex and age group, and also geographically by National Health Service commissioning region.
How might it impact on clinical practice in the future?
Health region commissioners may wish to investigate what underlies the variability in the rate of these two procedures and the associated service and financial implications.
There is a need to standardise treatment and develop national treatment guidelines.
Introduction
In the normal knee, the anterior cruciate ligament (ACL) plays an important role in mechanical stability and proprioception.1 ACL injury is common, with a median incidence of approximately 0.03% per person per year overall and up to 3.7% in some groups of professional athletes.2 In the past, operative management of a ruptured ACL has been recommended due to the associated functional impairment and concerns that recurrent instability of the knee may lead to further meniscal or articular damage and, later, osteoarthritis.1 ACL reconstruction (ACLr) has become the treatment of choice for those with symptomatic instability and high-demand individuals.1 3 Nevertheless, recent clinical trial evidence has challenged whether routine ACLr is required to deliver functional joint stability.4 5 Following the publication of this key clinical trial in 2010, a strategy of rehabilitation with optional delayed ACLr has been advocated.4–6 Alternatively, a treatment strategy with early ACLr may prevent secondary injury and achieve more reliable functional outcomes.7 8
Meniscal tears occur in approximately 6% of patients following an acute knee injury and the risk is greater in those with an associated ACL rupture.9 Whereas excision of unstable meniscal tear tissue, ‘meniscectomy’, was standard practice in the past, more recently, meniscal repair (MR) has been strongly advocated, especially for ‘traumatic’ meniscal tears in patients without pre-existing knee osteoarthritis.10–13 MR aims to preserve meniscal tissue and it is believed that maintaining and repairing this tissue will reduce joint contact pressures and contribute to joint stability, consequently reducing the relative risk of subsequent osteoarthritis.10–13 In accordance with this evolving philosophy, a change in practice might be anticipated and, in the USA, a doubling of the rate of MR procedures between 2005 and 2011 has been reported.14 In England, whereas trends in the rate of arthroscopic meniscectomy have been reported recently, trends in MR are unknown.15
An understanding of the trends and variation in intervention rate for these procedures is important to inform health commissioners and support future cost-effectiveness analysis, as well as to determine the potential impact from any change in practice.16 The appropriate intervention rate for the procedures is not yet known, but these data will support an assessment of possible overutilisation or underutilisation of the procedures, comparison between regions and also between the health systems of different countries.
We aimed to review temporal trends and regional variation in the practice of ACLr and MR in England over the last 20 years.
Methods
Data source
The data source was the national hospital episode statistics (HES) dataset for England. HES includes episodes of care delivered in National Health Service (NHS) hospitals, treatment centre care funded by the NHS and privately funded or non-resident patients treated within NHS England hospitals.17
Procedures
All patients undergoing ACLr or MR between 1 April 1997 and 31 March 2017 were identified from the recorded Classification of Surgical Operations and Procedures (OPCS-4) codes (see online supplementary appendix 1 for OPCS-4 code list) and extracted from HES for the purposes of this study.18 Patients undergoing concurrent procedures were included in both the ACL and MR cohorts, respectively, but a separate analysis of the proportion of patients undergoing combined ACL and MR was also performed.
Supplemental material
Statistical analysis
Stata V.15.1 (StataCorp) was used to perform all analyses. To adjust for changes in population demographics over time, denominator data from the Office for National Statistics (ONS) were used to calculate age-standardised and sex-standardised rates with 95% CIs, following the methodology of the Association of Public Health Observatories.19
To investigate for any regional variation in practice, the clinical commissioning group (CCG) responsible for each episode of treatment was extracted. In England, CCGs were created as part of the Health and Social Care Act 2012 and replaced Primary Care Trusts in April 2013.20 CCGs are statutory bodies responsible for the planning and regional delivery of healthcare services. Resident population data by age, sex and year within each CCG were obtained from the ONS.
The geographical information system, QGIS V.3.0 (http://www.qgis.org), was used to map the age-standardised and sex-standardised rate of surgery by CCG of treatment (region where the surgery was undertaken) and also by the CCG of patient residence (region where the patient lived, irrespective of where surgery was undertaken), using the April 2017 CCG boundaries.21 In April 2017, there were 207 CCGs in England, each responsible for a population of approximately 250 000 (70 000–900 000).20 22
Ethical approval
In accordance with the Health Research Authority (HRA) recommendations on analysis of routinely collected observational data, formal research ethics committee approval was not required for this study.23 Prior to the release of the data for analysis, the project was approved by the NHS Digital Independent Group Advising on the Release of Data (IGARD) committee (NHS Digital application DARS-NIC-68703).
Results
Temporal trends
Anterior cruciate ligament reconstruction
Between 1 April 1997 and 31 March 2017, a total of 133 270 ACLrs were performed in 124 489 patients (21 373 female; 17.2%) of mean age 29.5 (SD 9.89). Nationally, the age-standardised and sex-standardised rate of ACLr increased 12 times from 2.0/100 000 (95% CI 1.9 to 2.1) in 1997–1998 to 24.2/100 000 (95% CI 23.8 to 24.6) in 2016–2017 (figure 1). The greatest average annual rate of increase was observed between 2005/2006 and 2008/2009, at 43.08%/year, in comparison to 16.03%/year between 1997/1998 and 2005/2006, and 3.73%/year between 2008/2009 and 2016/2017. The rate of simultaneous ACLr and MR increased from 0% in 1997/1998 to 10.7% (95% CI 10.2% to 11.3%) of ACLr cases (2.6/100 000 population; 95% CI 2.5 to 2.8) in 2016/2017 (online figure S1 in supplementary appendix 2).
Supplemental material

National age-standardised and sex-standardised rate of ACL reconstruction and meniscal repair per 100 000 population, by year. ACLr, anterior cruciate ligament reconstruction.
ACLr was most commonly performed in the 20–29 and 30–39 age groups and increased considerably in all age groups over time (figure 2A). In the under 20 age group, the rate increased 22 times from 0.7/100 000 (95% CI 0.5 to 0.8) in 1997/1998 to 15.4/100 000 (n=2018; 95% CI 14.7 to 16.0) in 2016/2017. In the 20–29 age group, the rate increased 11.5 times from 6.7/100 000 (95% CI 6.0 to 7.3) to 76.9/100 000 (n=5720; 95% CI 74.9 to 78.9). In the 30–39 group, the rate increased 8.6 times from 5.0/100 000 (95% CI 4.5 to 5.5) to 43.1/100 000 (n=3156; 95% CI 41.6 to 44.6). In the 40–49 age group, the rate increased 13.9 times from 1.5/100 000 (95% CI 1.2 to 1.8) to 20.9/100 000 (n=1550; 95% CI 19.9 to 22.0). The greatest percentage increase in the rate of surgery was observed in the 50–59 age group, increasing 32.5 times from 0.2/100 000 (95% CI 0.1 to 0.4) to 6.5/100 000 (n=471; 95% CI 5.9 to 7.0).

(A) Sex-standardised rate of ACL reconstruction by age group and year. (B) Sex-standardised rate of meniscal repair by age group and year. ACL, anterior cruciate ligament.
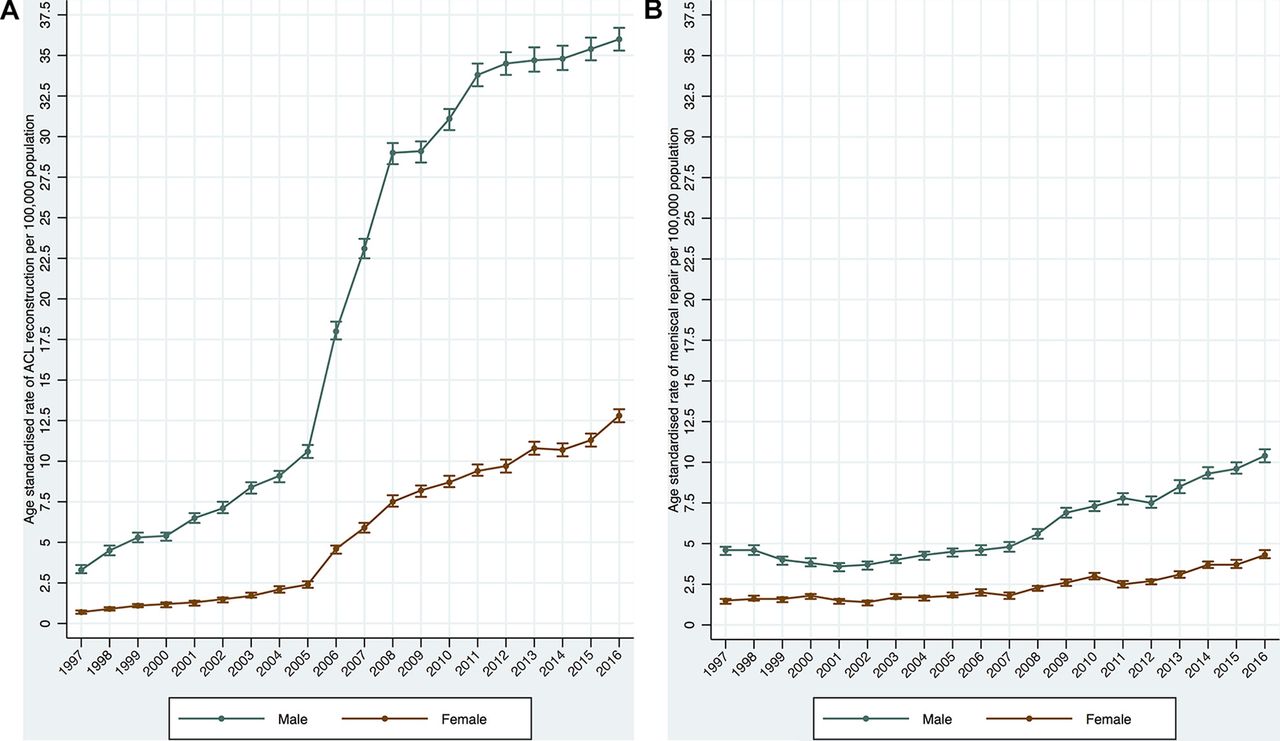
Surgery was performed at a higher rate in male patients and the rate of surgery increased in both male and female patients (figure 3A). In male patients, the rate of surgery increased from 3.3/100 000 (95% CI 3.1 to 3.6) in 1997–1998 to 36.0/100 000 (95% CI 35.3 to 36.7) in 2016–2017. In females, the rate increased from 0.7/100 000 (95% CI 0.6 to 0.8) in 1997–1998 to 12.8/100 000 (95% CI 12.4 to 13.2) in 2016–2017.

(A) Age-standardised rate of ACL reconstruction by sex and year. (B) Age-standardised rate of meniscal repair by sex and year. ACL, anterior cruciate ligament.
Meniscal repair
Over the study period, a total of 42 651 MRs were performed in 41 120 patients (11 761 female; 28.6%) of mean age 33.3 (SD 15.2). Nationally, the age-standardised and sex-standardised rate of MR increased 2.4 times from 3.0/100 000 (95% CI 2.8 to 3.1) in 1997–1998 to 7.3/100 000 (95% CI 7.1 to 7.5) in 2016–2017 (figure 1). For MR, the greatest average increase was observed between 2007/2008 and 2009/2010, at 19.35%/year, in comparison to 1.28%/year between 1997/1998 and 2007/2008 and 6.64%/year between 2009/2010 and 2016/2017. The rate of recorded simultaneous MR and ACLr increased from 0% in 1997/1998 to 35.6% (95% CI 34.1% to 37.1%) of MR cases (2.6/100 000 population; 95% CI 2.5 to 2.8) in 2016/2017 (online figure S1 in supplementary appendix 2).
MR was most commonly performed in the 20–29 and 30–39 age groups and increased considerably in all age groups over time (figure 2B). In the under 20 age group, the rate increased 5.2 times from 1.3/100 000 (95% CI 1.1 to 1.5) in 1997/1998 to 6.7/100 000 (n=878; 95% CI 6.3 to 7.1) in 2016/2017. In the 20–29 age group, the rate increased 3.8 times from 5.2/100 000 (95% CI 4.7 to 5.8) to 19.8/100 000 (n=1474; 95% CI 18.8 to 20.9). In the 30–39 group, the rate increased 2.4 times from 4.8/100 000 (95% CI 4.3 to 5.3) to 11.3/100 000 (n=826; 95% CI 10.5 to 12.1). In the 40–49 age group, the rate increased 1.3 times from 4.1/100 000 (95% CI 3.6 to 4.5) to 5.3/100 000 (n=393; 95% CI 4.8 to 5.9).
Surgery was performed at a higher rate in male patients and the rate of surgery increased in both male and female patients (figure 3B). In male patients, the rate of surgery increased from 4.6/100 000 (95% CI 4.3 to 4.8) in 1997–1998 to 10.4/100 000 (95% CI 10.0 to 10.8) in 2016–2017. In females, the rate increased from 1.5/100 000 (95% CI 1.3 to 1.6) in 1997–1998 to 4.3/100 000 (95% CI 4.1 to 4.6) in 2016–2017.
Regional variation
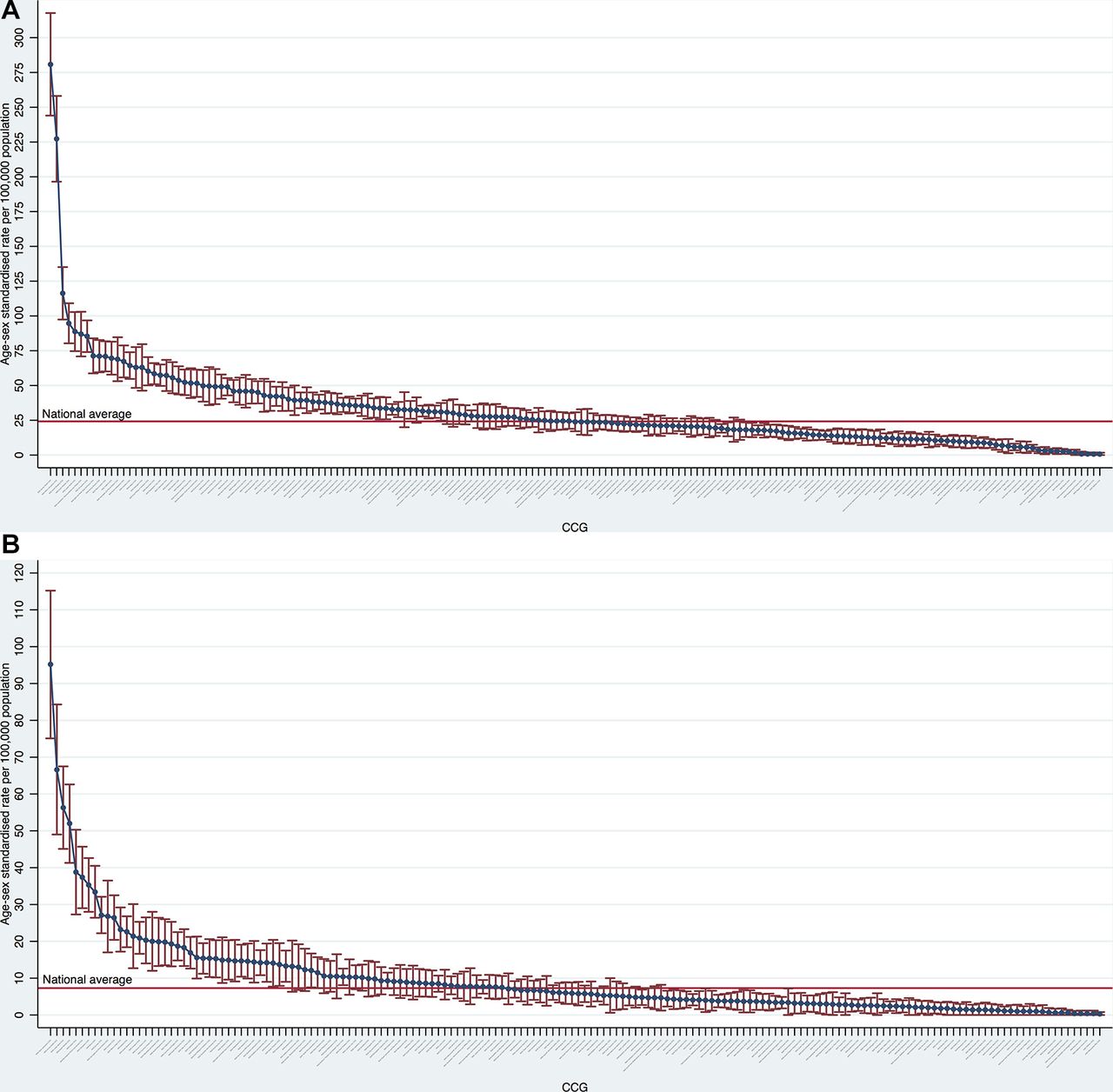
Regional variation in the rate of ACLr over time, by CCG, is shown in figure 4A, and for MR in figure 4B. In 2016–2017, 14.5% (30/207) CCGs performed more twice the national average rate of ACLr (figure 5A) and 15.0% (31/207) performed more than twice the national average rate of MR (figure 5B).
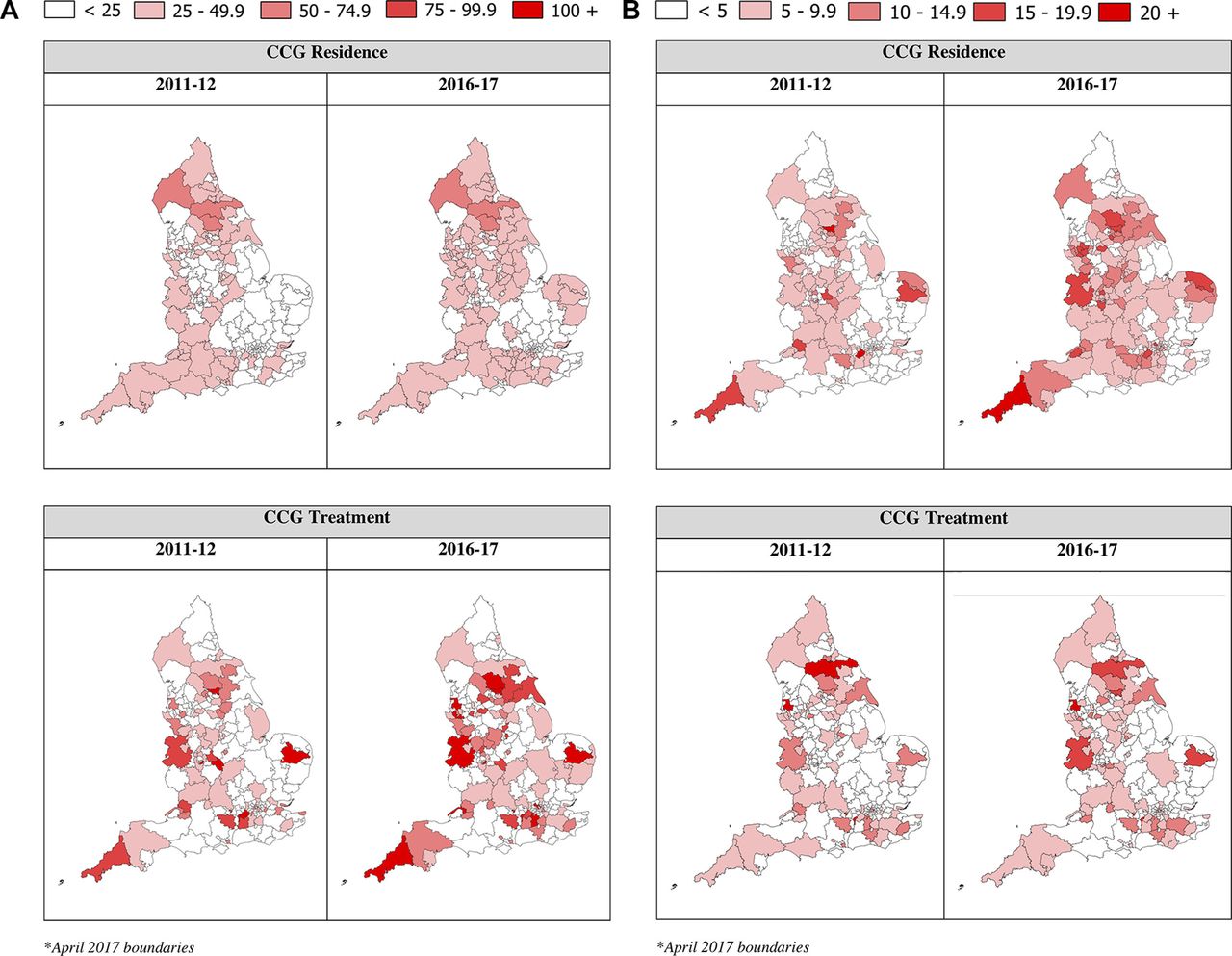
(A) Regional variation in age-standardised and sex-standardised rate of ACL reconstruction per 100 000 population by NHS CCG*. (B) Regional variation in age-standardised and sex-standardised rate of meniscal repair per 100 000 population by NHS CCG*. CCG treatment=region where the surgery was undertaken. CCG residence=region where the patient lived, irrespective of where surgery was undertaken. ACL, anterior cruciate ligament; CCG, clinical commissioning group.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Caterpillar plot of variation of age-standardised and sex-standardised rate of ACL reconstruction per 100 000 population by treating NHS clinical commissioning group (CCG) in 2016/2017. (B) Caterpillar plot of variation of age-standardised and sex-standardised of meniscal repair rate per 100 000 population by treating NHS CCG in 2016/2017. ACL, anterior cruciate ligament; NHS, National Health Service.
Discussion
Temporal trends
Between 1997 and 2017, the age-standardised and sex-standardised rate of ACLr increased 12 times and MR by 2.4 times. The most rapid period of an increase was observed between 2005/2006 and 2008/2009 for ACLr and between 2007/2008 and 2009/2010 for MR. The underlying reasons for the increase are unclear but could include an appropriate adjustment in intervention rates from a level of previous service under provision, increasing injury rates, increasing surgeon numbers or specialist training, changes in healthcare commissioning or evolving patient treatment preferences.
Despite the increases, the absolute rate of surgery in England (24.2/100 000 in 2016/2017) does remain lower than rates that have been reported in other countries and therefore the ‘correct’ intervention rate is unknown.2 For example, in studies published between 1999 and 2011, the national rate of ACL surgery was 52/100 000 in Australia, 38/100 000 in Denmark, 37/100 000 in New Zealand, 34/100 000 in Norway, 32/100 000 in Sweden, 28-52/100 000 in the USA and 8/100 000 in Scotland.2 24 Regarding changes in intervention rate over time, in the USA, the rate of ACLr in patients under the age of 65 rose from 61.4/100 000 in 2002 to 74.6/100 000 in 2014 and similar increases have been reported in Australia and in previous years in the USA.24–26 The rate of MR observed in our study in 2016/2017 was comparable to that recently reported in Japan, but lower than the a rate of 20/100 000 reported for 2011 in the USA.14 27 Many factors which may explain these differences and it is important to note that privately funded procedures were not included in our dataset, as discussed later. In our study, the observed rate of simultaneous ACL reconstruction and MR increased from 0% in 1997/1998 to 11% of ACLr and 36% of MR cases in 2016/2017, respectively. In other series, the reported proportion of ACLr patients undergoing simultaneous MR varies from approximately 6% to 21%.28 29
One factor that might underlie the observed increase in intervention rate is an increase in injury rate. Our dataset did not include injury data and there are conflicting data regarding changes in knee injury rates in the literature. In some patient groups, especially some young sportspersons, rates appear to be rising, but in others rates may be falling and, although limited, no overall increase has been observed in national series in the USA or Sweden.26 30–32 Male patients have previously been found to be at increased risk of ACL injury and, as in our study, also ACL surgery.33 Age group-specific rates of ACLr have been reported as high as 160/100 000 in males and 80/100 000 in females in New Zealand.33 Different sporting groups are also at variable risk and annual injury rates greater than 1000/100 000 have been reported in certain professional athletes but occupation and sport participation data were not available for our cohort.2
In our study, although ACLr was most commonly performed in the 20–29 age group, the greatest increase in intervention rate was observed in the 50–59 age group. The reasons for this are unclear and may reflect increasing sporting participation and injury rates in older age groups or changing patient selection and treatment practices. For MR, the most common age group was also 20–29 years but the greatest increase was observed in the under 20 age group. This increase may reflect a general drive towards meniscal preservation surgery, especially in younger patients.10–13
For ACLr, the rate of intervention has increased despite the publication of clinical trial evidence and a Cochrane review indicating that many patients may avoid the need for reconstruction following a period of structured physiotherapy.4 5 For MR, no comparably high-quality evidence exists and only one small randomised study has been published.11 34–37 Although cohort studies have indicated patients undergoing MR rather than meniscectomy may be at decreased risk of developing osteoarthritis, these studies were not randomised.9 10 12 13 35 Nevertheless, MR is now strongly advocated and recent clinical studies have focused on investigating strategies to improve MR healing rates.11 12 34 35 Further work is required in this area to refine appropriate indications for surgery and guide treatment decisions.
Regional variation
Regional variation in the rate of both ACLr and MR was detected, as has recently been observed for other types of knee arthroscopy in England.15 For other orthopaedic procedures, comparable regional variation has been reported for shoulder arthroscopy and hip arthroscopy in England.38 39 Within the UK, rates of knee arthroscopy have previously been reported to be lower in England than in Scotland.40
Factors underlying variation in practice have been extensively investigated and underlying causes may include service or population differences, patient or surgeon belief in the procedure, surgeon numbers or specialist training and improvements to surgical techniques making procedures more accessible to be undertaken by non-specialists.41 42 There are many ways to address variation in the use of surgery including education, treatment guidelines, and also provision of individual clinician feedback on outcomes and facilitating comparison with peers.42 For ACLr, clinical practice and outcome feedback is available in the UK through the National Ligament Registry, but this is a voluntary registry and no such initiative exists for MR.43
Intervention rates of some other surgical procedures have been evaluated based on ‘appropriateness criteria’, which have been used to standardise treatment decisions and identify potential overuse.44 45 A trial of treatment strategies for ACL injured patients is ongoing in England and may lead to a change in practice.46 For meniscal surgery, a national clinical treatment guideline is under development.47 To inform regional healthcare commissioners, it may be possible to use the clinical trial evidence concerning the effectiveness of rehabilitative strategies in ACL injury to estimate an anticipated intervention rate from injury data. For appropriate shared decision-making, in addition to a further investigation of benefits, the short-term and long-term adverse outcomes associated with undergoing these procedures following ACL or meniscal injury also require further definition.48 For example, it is important for patients and clinicians to understand the true risk of complications, the rate of reoperation and revision surgery, and the long-term rates of osteoarthritis and knee arthroplasty.
Strengths and limitations
There are some limitations to our study. These data are observational only and the causative factors underlying the increased rate of ACLr and MR cannot be determined. Hospital trusts rely on the accuracy of HES data reporting for payment for the surgical procedures performed and this provides a strong incentive for procedural coding data accuracy, but the absolute accuracy cannot be proven. Although the specific codes used in this study have not been formally validated, for reference, HES comorbidity field coding and serious vascular diagnoses have both been shown to correlate strongly with primary care records.49 50 It is also important to acknowledge that the OPCS-4 code used to identify ACLr procedures may also have captured some posterior cruciate ligament reconstruction procedures. Posterior cruciate ligament reconstruction is, however, comparatively rare in other series and is unlikely to have materially altered the observed changes in intervention rate.51
Due to the distribution of hospitals and service, not all CCGs perform knee arthroscopy within their region and it is likely that these CCGs commission this treatment elsewhere. Regional treatment rates may, therefore, be overestimated or underestimated when there is a high level of migration in or out of one region to another. Both the CCG of patient treatment and the CCG of patient home residence is reported in this study for completeness and to ease interpretation of the potential impact of these factors.
It is important to note that HES does not include private sector procedures, unless funded by the NHS or privately funded but performed in an NHS hospital. The number of ACLr and MR procedures performed in the private healthcare sector is unknown but private healthcare expenditure as a proportion of total private and public expenditure has remained relatively stable over time, suggesting this is unlikely to explain the observed changes in the rate of surgery in England.52
Conclusion
There has been an increase in the rate of ACLr and MR performed in England over the last two decades with variation in surgical practice. Rates of surgery may be influenced by service availability, patient treatment preferences, surgeon numbers and specialist training. Standardised treatment guidance is required to reduce this variation.
References
Footnotes
Contributors SGFA: concept, methodology, analysis, writing and editing paper, guarantor. AJP: concept, methodology, editing paper. AJ: methodology, analysis, editing paper. DJB: concept, methodology, editing paper.
Funding This report is independent research supported by the National Institute for Health Research (NIHR Doctoral Research Fellowship, SGFA, DRF-2017-10-030) and NIHR Oxford Biomedical Research Centre (BRC). AJ is supported by the NIHR Biomedical Research Centre at the University Hospitals Bristol NHS Foundation Trust and the University of Bristol.
Competing interests AJ has received consultancy fees from Freshfields Bruckhaus Deringer (on behalf of Smith & Nephew Orthopaedics), and is a member of the data safety and monitoring board (which involved receipt of fees) from Anthera Pharmaceuticals.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.