Article Text

Abstract
Objective To investigate the risk of new meniscal tears after treatment for anterior cruciate ligament (ACL) injury, in children and adults with and without ACL reconstruction.
Design Prognosis systematic review (PROSPERO registration number CRD42016036788).
Methods We searched Embase, Ovid Medline, Cochrane, CINAHL, SPORTDiscus, PEDro and Google Scholar from inception to 3rd May 2018. Eligible articles included patients with ACL injury (diagnosis confirmed by MRI and/or diagnostic arthroscopy), reported the number of meniscal tears at the time of ACL injury diagnosis/start of treatment and reported the number of new meniscal tears that subsequently occurred. Articles with fewer than 20 patients at follow-up, and articles limited to ACL revision surgery or multi-ligament knee injuries were excluded. Two independent reviewers screened articles, assessed eligibility, assessed risk of bias and extracted data. We judged the certainty of evidence using the Grading of Recommendations Assessment Development and Evaluation (GRADE) working group methodology.
Results Of 75 studies included in the systematic review, 54 studies with 9624 patients and 501 new meniscal tears were appropriate for quantitative analysis. Heterogeneity precluded data pooling. The risk of new meniscal tears was 0%–21% when follow-up was <2 years, 0%–29% when follow-up was 2 to 5 years, 5%–52% when follow-up was 5 to 10 years and 4%–31% when follow-up was longer than 10 years. The proportion of studies with high risk of selection, misclassification and detection bias was 84%, 69% and 68%, respectively. Certainty of evidence was very low.
Conclusion New meniscal tears occurred in 0%–52% of patients between 4 months and 20 years (mean 4.9±4.4 years) following treatment for ACL injury. The certainty of evidence was too low to guide surgical treatment decisions. This review cannot conclude that the incidence of new meniscal tears is lower if ACL injury is treated with surgery compared with treatment with rehabilitation only.
- ACL injury
- ACL reconstruction
- non-operative treatment
- non-surgical treatment
- active rehabilitation
- rehabilitation
- physiotherapy
- secondary meniscal injury
- ACL injury treatment
Statistics from Altmetric.com
- ACL injury
- ACL reconstruction
- non-operative treatment
- non-surgical treatment
- active rehabilitation
- rehabilitation
- physiotherapy
- secondary meniscal injury
- ACL injury treatment
Introduction
Meniscal tears, especially those resulting in meniscal loss or dysfunction, are the suspected main culprits for knee osteoarthritis (OA)1 and poor knee health.2 3 Meniscal tears represent a burden for the individual patient and for society. In the short term, patients may experience pain, activity limitations and may need surgery; society bears expenses due to healthcare and sick leave. In the long term, patients and society continue to strain under the same burdens, amplified by time.4 5
Protecting the meniscus must be central to decision-making in anterior cruciate ligament (ACL) injury treatment.6 Having an ACL reconstruction does not prevent knee OA after ACL injury.1 7 Sustaining meniscal tears, either at the time of the ACL injury or subsequent to the ACL injury, increases the risk of OA.8–12 Clearly, avoiding new meniscal tears is a priority for all patients with ACL injury and their treating clinicians. The risk of developing new meniscal tears looms over ACL injury treatment, rehabilitation, return to sport and injury prevention decisions.
Experts agree that all patients should receive quality rehabilitation and secondary injury prevention to reduce the risk of new knee injuries including meniscal tears.13 But there is fierce debate about whether ACL reconstruction should be a mandatory part of treatment algorithms that focus on protecting the meniscus.13–16 Some clinicians advocate early ACL surgery to prevent knee instability, and subsequently, new injuries to the menisci and cartilage.17–21 Others advocate early active rehabilitation to improve muscle function and stabilise the knee, only recommending ACL surgery if knee instability persists despite high-quality rehabilitation, or in the presence of repairable meniscal injuries.14 22–24
Clinicians and patients are challenged because research on new or secondary meniscal tears after ACL injury is inconsistent, and may have methodological shortcomings.13 25 26 Rates of new meniscal tears may differ depending on a patient’s age or the treatment received (ie, ACL surgery or non-surgical ACL treatment), and affording credence to studies with high risk of bias might mislead clinical decisions.25 26
Clinicians need accurate information about the risk of new meniscal tears after ACL injury to help them make quality decisions in practice. Therefore, we aimed to investigate the risk (measured by incidence proportion) of new meniscal tears after ACL injury. We aimed to address three key questions:
What is the risk of new meniscal tears following treatment for ACL injury over time?
Is there a difference in risk of new meniscal tears between patients who had ACL reconstruction and patients who had non-operative treatment?
Is the risk of new meniscal tears different between patients who were skeletally immature and patients who were skeletally mature at the time of treatment for ACL injury?
Methods
This systematic review adhered to the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analysis) guidelines27 28 and the review protocol, which was published prospectively.26 We prospectively registered this systematic review in the International Prospective Register of Systematic Reviews (PROSPERO registration number: CRD42016036788).
Eligibility criteria
To be included in the systematic review, articles had to (1) include patients of any age with ACL injury (diagnosis confirmed by arthroscopy or MRI in all patients), (2) report the number of meniscal tears at the time of ACL injury diagnosis or start of ACL treatment (providing a meniscal baseline, to maximise the likelihood that subsequent meniscal injuries were new injuries) and (3) report the number of patients with new meniscal tears occurring after the defined baseline. We excluded literature reviews, non-English language articles, articles reporting on fewer than 20 patients at final follow-up and articles limited to ACL revision surgery or multi-ligament injuries.26 We did not exclude studies on the basis of design or follow-up.
We defined a new meniscal tear as a meniscal tear that occurred after the ACL injury baseline, but we did not specify criteria for diagnosing a meniscal tear.
Search strategy
We searched the following databases from inception to 3 May 2018: Embase, Ovid Medline, Cochrane Library, CINAHL, SPORTDiscus, PEDro and Google Scholar.26 The search strategy is provided in online supplementary file 1.
Supplemental material
We used three additional search approaches to identify any potentially eligible articles that may have been missed in the electronic database search: (1) we manually searched the reference lists of included studies and relevant systematic reviews, (2) we conducted forward citation tracking using Google Scholar, (3) we manually searched ePublication lists for any articles that may not have been indexed by the electronic databases in the following journals: American Journal of Sports Medicine, Journal of Bone and Joint Surgery, Arthroscopy, Bone & Joint Journal and British Journal of Sports Medicine.26 All search results were exported to an EndNote library and checked for duplicates. All identified articles were uploaded to Covidence29 to manage the article selection process.26
Article selection
Two reviewers (GRE and CA) independently screened titles and abstracts to identify potentially relevant articles (figure 1). All potentially relevant articles were reviewed in full text by GRE and CA. The inter-rater agreement for eligibility was moderate (Cohen’s kappa: 0.57).30 Disagreements were resolved by consensus, and a third author (HG) was consulted if required. If multiple publications reported on the same study, we prioritised the article with the longest follow-up to avoid reporting on the same patients twice. Consequently, eight studies were excluded from the systematic review.31–38

PRISMA flow chart. From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi:10.1371/journal.pmed1000097. ACL, anteriorcruciate ligament; PRISMA, PreferredReporting Items for Systematic reviews and Meta-Analysis.
Data extraction and risk of bias assessment
Data from all included articles were extracted independently and in duplicate.26 GRE extracted data from all included articles; CA and HG each extracted data from 50% of the articles. Disagreements were resolved by consensus, or a third reviewer (either CA or HG), if required. We contacted study authors for clarification, if required.
We assessed the risk of bias with the Newcastle Ottawa Quality Assessment Scale for Cohort Studies (see online supplementary file 2).39 This tool was also appropriate for the randomised controlled trials (RCTs) included in this review because we treated RCTs as cohort studies for the purpose of establishing the risk of new meniscal tears. We combined data from the surgical treatment groups (ie, from patients treated with single or double bundle hamstring grafts).40–44 We rated each study on eight items (domains), and these ratings were subsequently dichotomised as low or high risk of bias (1) for each domain and (2) for overall bias (across studies), based on predefined decision rules (see online supplementary file 3). We pilot-tested the data extraction table (see online supplementary files 4.1–4.3) and risk of bias assessment tool before using them.26
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Data analysis and synthesis
A biostatistician executed the data analysis according to our predefined analysis plan (see online supplementary file 5). All analyses were conducted using Stata 15 (StataCorp. 2017, Stata Statistical Software: Release 15; StataCorp, College Station, Texas, USA).
Supplemental material
The main analysis was a proportion meta-analysis using Stata metaprop syntax to determine the incidence proportion of new meniscal tears following treatment for ACL injury. Studies were stratified by follow-up time categories: <2 years, 2 to 5 years, 5 to 10 years and >10 years. We used a random-effects model because we expected statistical heterogeneity. To ensure a meaningful pooled estimate, we chose not to pool data if statistical heterogeneity was >75%.45 We presented summary estimates for the risk of new meniscal tears graphically in a forest plot.
We assessed publication bias and small study effects with a funnel plot.44 Cohen’s kappa was calculated using Predictive Analytics Software Statistics (V.24.0; SPSS, Chicago, Illinois, USA).30 We used Stata melogit syntax to examine the relationship between follow-up time and new meniscal tears and compare the risk of new meniscal tears between subgroups.
Sensitivity analyses
We conducted sensitivity analyses based on (1) meniscal tear detection methods to assess whether the diagnostic method affected the results, (2) selection bias as determined from the risk of bias assessment, (3) detection bias as determined from the risk of bias assessment, (4) whether all patients had meniscal repair at baseline or not (5) and whether patients had ACL reconstruction or other ACL surgery (eg, ACL repair). Patients who had other ACL surgery had a substantially higher incidence proportion of new meniscal tears (other ACL surgery: 16%, 95% CI: 6% to 29%, I2=87%; all studies combined: 9%, 95% CI: 7% to 11%, I2=85%). There was a substantially lower incidence proportion of new meniscal tears in studies where the meniscus injury diagnosis was based on clinical examination only (studies with clinical diagnosis only: 3%, 95% CI: 1% to 6%, I2=72%; all studies: 9%, 95% CI: 7% to 11%, I2=85%). Therefore, in the main analysis, we excluded studies where patients had other ACL surgery, and studies where the meniscus injury diagnosis was based on clinical examination only.
Finally, we completed an additional post hoc sensitivity analysis to evaluate the effect of the largest study on the results (Davis et al,46 n=4087). When we excluded this study from analysis, the I2 statistic was >75% and the pooled estimate for the 2–5 year follow-up category was not substantially changed. Therefore, we retained Davis et al 46 in the analyses.
Subgroup analyses
Predefined subgroups were (1) patients treated with ACL reconstruction compared with non-operative treatment and (2) skeletally immature patients compared with skeletally mature patients. We accepted skeletal immaturity as defined in the study (method of assessment was extracted, that is, X-rays, Tanner staging, MRI). If skeletal immaturity was not defined in the study, we applied our definition of age under 16 years at injury for all patients.
Strength of recommendations and certainty of evidence
We judged the certainty of evidence using the Grading of Recommendations Assessment Development and Evaluation (GRADE) working group methodology (www.gradeworkinggroup.org).47 We considered potential limitations due to risk of bias, inconsistency, indirectness, imprecision and publication bias, and judged high, moderate, low or very low certainty.47–49 We used GRADEpro (GRADEpro GDT: GRADEpro Guideline Development Tool; McMaster University, 2015; Evidence Prime; gradepro.org) to create the evidence profile. The judgement reasoning is described in detail in online supplementary file 6.
Supplemental material
Results
Seventy-five studies were included in the systematic review for qualitative synthesis (figure 1), and 54 studies (9624 patients) were appropriate for quantitative synthesis (meta-analysis). The reasons for excluding articles from meta-analysis were clinical diagnosis of meniscal tear only (10 studies35 50–58 and 1 additional study arm24), other ACL surgery than ACL reconstruction (4 studies)59–62 or both (2 studies).63 64 We excluded studies if there was an unknown number of patients with new meniscal injuries (four studies).65–68 We made a post hoc decision to exclude one study of patients with partial ACL tears.69
Study characteristics
Twenty-five of 75 included studies (33%) had a prospective design (17 RCTs, 8 prospective case series), and 50 studies (67%) had a retrospective design (50 retrospective case series) (see online supplementary file 7 for characteristics of all included studies). The follow-up period ranged from 4 months to 20 years. Fifty-seven of 75 studies (75%) had at least 2 years of follow-up. The follow-up rate was higher than 80% in 41 of 75 studies (55%).
Supplemental material
The 75 included studies had 11 707 individual patients at inclusion. The smallest study included 20 patients, and the largest included 4087 patients (median 72 patients). At least 4143 (35%) patients were women; sex was not reported in 10 studies. Six studies included only patients who were skeletally immature as defined by remaining growth based on hand X-rays (n=3),52 57 70 open growth plates at X-rays and Tanner staging (n=2)53 71 or open growth plates at MRI (n=1).72 Twenty-seven studies included only skeletally mature patients and 27 studies included a mixed population of patients aged under and over 16 years and did not clarify skeletal maturity. Age at inclusion was unclear in 15 studies. Forty-five studies only included patients with ACL reconstruction. Eleven studies only included patients with non-operative treatment.
In 13 studies (17% of 75), all patients had MRI or arthroscopy at follow-up; the assessor was independent in two studies.73 74 In 32 studies (43% of 75), new meniscus injury was detected by clinical examination followed by arthroscopy and/or MRI on indication (ie, in some patients). In 21 studies (28% of 75), the detection method of new meniscal tears was unclear. In 51 (68% of 75) studies, the authors only reported surgically treated tears and most of these studies (49 studies) only reported surgeries at the study centre. Four studies described the total number of meniscus injuries, but not the number of injured patients. These studies were excluded from meta-analysis.
Risk of bias within domains for individual studies
All included studies had limitations in at least two bias domains (table 1; online supplementary file 8). We judged 51 to 63 studies (68%–84% of 75 studies) at high risk of bias for the domains: representativeness of the exposed cohort (selection bias), demonstration that the outcome of interest was not present at the start of the study (misclassification bias) and assessment of the outcome (detection bias) (table 1). Two studies assessed the outcome in all patients in the study with appropriate measures by an independent examiner. Follow-up time and rate were adequate in 57 (76%) and 41 (55%) studies (defined as long enough for outcome to occur; at least 2 years and follow-up rate at least 80%).
Supplemental material
Risk of bias assessment
Incidence of new meniscus tears after treatment for ACL injury
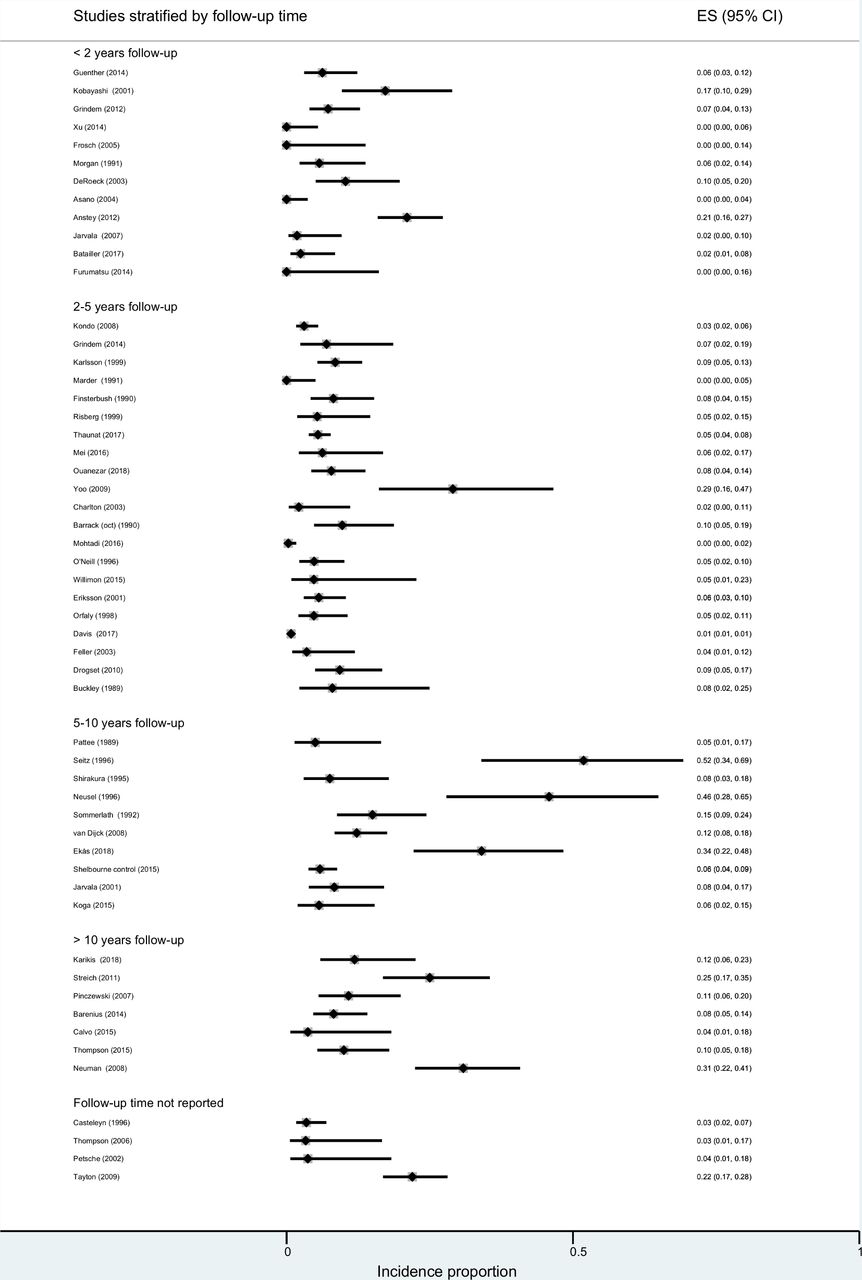
Among the 9624 patients included for quantitative analysis, 501 sustained new meniscal tears. The risk of new meniscal tears varied from 0% to 52% over a follow-up of 4 months to 20 years (mean 4.9±4.4 years) (figure 2). The incidence proportion was 0%–21% when follow-up was <2 years, 0%–29% when follow-up was 2 to 5 years, 5%–52% when follow-up was 5–10 years and 4%–31% when follow-up was >10 years (figure 2). Longer follow-up was associated with a higher meniscal injury incidence proportion: 12% higher odds of meniscal injury per year of follow-up (OR: 1.12, 95% CI: 1.05 to 1.20, p<0.001).
{kind=link}
{kind=link}
Forest plot of new meniscal tear rate in individual studies stratified by follow-up time (no pooled estimate). ES, effect estimate for individual studies.
We intended to use the Stata melogit syntax to compare the risk of new meniscal tears in subgroups of ACL treatment and skeletal maturity. However, substantial heterogeneity, even after exclusion of studies with characteristics that skewed the results, precluded meaningful subgroup comparisons. Descriptive results from the ACL treatment and skeletal maturity subgroups are presented in online supplementary file 9. There was no clear evidence of small-study effects based on the funnel plot (see online supplementary file 10).
Supplemental material
Supplemental material
We downgraded the certainty of evidence due to risk of bias, inconsistency and indirectness (see online supplementary file 6). Overall, the certainty of evidence regarding the risk of new meniscal tears after ACL injury treatment was very low (table 2).
GRADE evidence profile for the question: what is the risk of new meniscal tears after treatment for ACL injury?
Discussion
The incidence proportion of new meniscal tears after treatment for ACL injury varied from 0% to 52% (4 months to 20 years after ACL injury, mean 4.9±4.4 years). Heterogeneity precluded meta-analysis and a meaningful pooled estimate. Heterogeneity also precluded a meaningful comparison by treatment or skeletal maturity. The body of evidence on new meniscal tears after ACL injury treatment has major scientific limitations, which should caution the clinician against relying on this evidence to guide clinical decisions and stimulate high-quality research.
There is insufficient evidence that choosing early ACL reconstruction over non-operative treatment with optional delayed ACL reconstruction helps patients avoid new meniscal tears. The very low certainty of evidence in our systematic review challenges the current clinical dogma that early ACL surgery is necessary to protect the meniscus. While insufficient evidence does not disprove the possibility that meniscal injury risk is lower following early ACL surgery, surgical treatment carries higher risk of harms (eg, complications from anaesthesia, infection) than non-operative treatment. When making decisions, patients and clinicians must consider the balance of benefits and harms, the burdens of surgery and non-operative treatments, the certainty of evidence for the outcome, feasibility and acceptability.
Why are the results so variable?
The results of the included studies may be influenced by clinical or methodological diversity.44 49 In this section, we address four issues that might impact on the certainty of evidence in our systematic review.
Issue 1: The reported number of new meniscal injuries depends on study methodology (eg, meniscal injury detection method) and clinical factors (eg, ACL surgical method). Studies where meniscal diagnosis was performed clinically (no MRI or arthroscopy) underestimated the rate of new meniscal tears. Meniscal injury risk was also substantially higher for patients who had ACL surgery other than ACL reconstruction (ie, ACL repair, ACL repair with augmentation, extra-articular tenodesis). We excluded studies where meniscal diagnosis was performed clinically, and studies where patients had other ACL surgery. However, the heterogeneity remained high. Other explanations for the heterogeneity include clinical factors (age, sex, body mass index, skeletal maturity, activity level, return to sport), surgical treatment (including previous meniscus treatment), rehabilitation, prevention and methodological factors49 (design, patient sample, method of detecting meniscal tears, definition/reporting of meniscal tears, follow-up rate, follow-up time).
Issue 2: Our results suggest selection bias may affect the rate of new meniscal tears. Studies that included patients with non-operative treatment scheduled for ACL surgery dominated the study categories of follow-up <2 years, 2 to 5 years and follow-up length not reported.75–77 Because patients scheduled for ACL reconstruction are a selected group who likely experience symptomatic knee instability, the risk of new meniscal tears may be higher compared with all patients with non-operative treatment. Similarly, the risk of new meniscal tears in selected copers (patients with non-operative treatment who do not experience symptomatic knee instability) is likely lower than in all patients with non-operative treatment. Therefore, translating new meniscal tear rates from selected patient groups to all patients with non-operative treatment may mislead clinicians and patients. To estimate the true risk of new meniscal tears after non-operative treatment, all patients should be followed prospectively from treatment initiation.
Issue 3: Most studies (68%) reported cases of new meniscal surgeries , not meniscal injuries . The number of surgeries is relatively straightforward to extract from a medical record/database—a less time-consuming and cheaper approach to data collection than adequately examining all patients for new meniscal injuries (eg, with diagnostic arthroscopy or MRI). However, reporting only meniscal surgeries and relying on medical charts alone underestimate the number of new meniscal injuries. Injuries diagnosed or treated elsewhere, and injuries treated non-operatively (or that were not detected) are all unlikely to be registered.
Issue 4: Early return to sport 78 and high activity level 79 are important confounders for new knee trauma (eg, new meniscal injuries) after ACL injury. The studies had insufficient information about postinjury activity level and return to high risk sports, and we were unable to account for these factors in our meta-analysis. Between-study differences in risk exposure may have contributed to the high heterogeneity in the results.
How do the systematic review results fit with existing literature?
Retrospective and cross-sectional studies report the number of children or adults with meniscal and/or cartilage injuries at the time of surgery stratified according to whether ACL surgery was performed early or late after ACL injury. Most of these studies,20 80–82 although not all,83 84 concluded there was a higher risk of meniscal injuries if patients had delayed ACL surgery. Because our review question focused on identifying new meniscal tears, we required studies to report meniscal injuries at a minimum of two time points: baseline (close to treatment of ACL injury) and at least one follow-up. We excluded a large number of cross-sectional studies because they either did not provide a baseline number of meniscal injuries (28 studies) or follow-up meniscal status to identify new meniscal injuries (137 studies).
Several narrative reviews17 19 85–87 have focused on timing of surgery and additional knee injuries in children and adults. Because a higher proportion of patients with meniscal and cartilage injuries had delayed ACL surgery, authors of narrative reviews have urged early surgery to prevent new meniscal injuries.17 86 However, research in this field is seriously limited by methodological bias, especially selection bias.13 25 26 The proportion of patients with meniscal tears who have delayed surgery does not provide a credible estimate of the risk of a new meniscal tear in all patients with ACL injury. Patients who seek medical attention may have sustained secondary injuries and present with knee pain and/or instability. As a result, patients may be scheduled for ACL surgery, where a meniscus tear can be detected. Patients who cope with their ACL injury and/or remain non-operatively treated are not included in these studies.
Conversely, there is no definitive evidence that other treatment strategies, such as non-operative treatment with optional delayed surgery, are superior to early surgery for reducing the risk of new meniscal tears. However, non-operative treatment with optional delayed surgery may be a reasonable alternative.14 24 72 88 An RCT can address some of the selection bias problems of non-randomised studies with regard to a question about treatment. One trial randomly allocated patients with ACL injury to receive either primary non-operative treatment or early surgery.14 However, the number of patients with new meniscal injuries was not reported (the total number of meniscal surgeries was reported; no significant difference between treatment groups). We contacted the authors to request data on new meniscal injuries after baseline; these data were unavailable. Early ACL reconstruction may reduce the risk of worsening medial meniscus integrity (but not lateral meniscus integrity) compared with a strategy of non-operative treatment with delayed ACL reconstruction, although these data are uncertain.89
Clinical implications
The very low certainty of evidence regarding new meniscal injuries after ACL injury is a warning to clinicians, patients and policy-makers. The clinical dogma that surgery is necessary to protect the meniscus in all patients with ACL injury is based on literature with serious scientific limitations. However, this does not rule out that ACL reconstruction may reduce meniscal injury risk. The uncertain evidence precludes firm conclusions. There are multiple underlying factors, other than surgery or non-operative treatment that affect new meniscal injury risk. A treatment strategy tailored to the individual patient’s needs and risk profile (activity level, instability/coping ability, additional injuries) may be appropriate. The decision to undergo ACL reconstruction or not, rehabilitation, safe return to sport (or changing sporting career) and continued injury prevention may all be important considerations in the treatment strategy to prevent meniscal injury.
The number of new meniscal tears is underestimated in studies where the diagnosis is only made clinically. Surgical case series and trials may also under-report new meniscal tears because the majority of studies only report on meniscal surgeries performed at the study centre. Consequently, clinicians must interpret results cautiously.
Strengths and limitations
We clearly defined new meniscal tears and required that meniscal injuries were reported at two time points to differentiate new tears from pre-existing tears. However, we could not distinguish new traumatic tears from new degenerative tears. Because we aimed to help clinicians and patients understand the strength of the evidence, we used GRADE methodology to evaluate the certainty of evidence based on assessing internal validity, applicability and generalisability. Despite included studies having more than one examination time point and diagnosing ACL injury based on MRI or arthroscopy, there was high unexplained heterogeneity that precluded meta-analysis, and very low certainty of evidence. Limitations in included studies are summarised in box 1.
Limitations in the included studies
The included studies had high risk of bias including selection bias, misclassification bias and detection bias. Included studies used different methods to detect and report new meniscal injuries (typically only new meniscal surgeries were reported/information based on medical chart reviews), variable follow-up time and variable follow-up rates. The effect of important confounding factors, such as activity level, on the estimate of new meniscal tears is unknown, and patient populations often included potentially skeletally immature patients. Most studies were retrospective and had small sample sizes. Only 13 out of 75 studies (17%) assessed all patients for the study outcome with appropriate measurement tools (MRI or arthroscopy).
Research implications
Key study findings are listed in box 2. More reliable estimates of the risk of new meniscal tears after ACL injury will help clinicians and patients make better decisions in practice. Studies appropriately designed to assess the risk of new meniscal tears after ACL injury in children, adolescents and adults are needed. The following areas must be addressed in future research:
Key findings
The heterogeneity in studies regarding risk of new meniscal tears after anteriorcruciate ligament (ACL) injury was substantial and precluded meta-analysis and comparison between groups.
There was very low certainty evidence that the rate of new meniscal tears varies between 0% and 52%.
Because most studies have high risk of bias and the certainty of evidence is very low, clinicians should be cautious when making decisions about ACL treatment.
Design: Employ prospective designs and approaches to reduce selection bias.
Patient selection: Select a representative study sample and clearly define the population to allow the reader to judge the representativeness of the sample.
Detecting meniscal injuries: Establish the baseline meniscal injury status early (to increase the likelihood of accurately detecting new injuries) after ACL injury with appropriate measures (MRI or arthroscopy) in all patients. Follow all patients up with MRI or arthroscopy. Describe the detection, diagnosis and reporting of meniscal tears in sufficient detail to facilitate replication, and define new meniscal tears versus pre-existing meniscal tears that have progressed since they were diagnosed at baseline.
Reporting meniscal injuries: New meniscal tears should be reported in all patients with appropriate measures, as reporting meniscal surgeries only is likely to underestimate the risk of new meniscal tears.
Consider that every patient has two knees and four menisci. Studies of new meniscal tears should report the number of meniscal injuries (their location should be indicated: medial, lateral or both) and the number of patients with meniscal tears. Describe meniscal tears in the contralateral knee separately.
Conclusion
There was very low certainty evidence, based on data from 9624 patients with ACL injury, that the risk of new meniscus tears following ACL treatment ranged from 0% to 52% at 4 months to 20 years after ACL injury. High heterogeneity precluded a meaningful comparison by ACL treatment approach or skeletal maturity. This review cannot answer the question “Is the risk of new meniscal tears lower when ACL injury is treated with surgery compared with treatment with rehabilitation only?”
What is already known
Preventing meniscus injuries should be a cornerstone in ACL treatment because they are an important predisposing factor for knee osteoarthritis.
There is a common belief that state that early surgery protects the menisci in the ACL deficient knee. Therefore, early surgery following ACL-injury is advocated by many clinicians and is the favoured treatment in many countries.
Retrospective or cross-sectional studies on the relationship between timing of surgery on additional injuries are commonly cited when this topic is discussed. However, patients who cope with their injury are not included in these studies.
What are the new findings
The heterogeneity in studies regarding new meniscal tears after ACL injury is substantial (I2 >93 and precluded a pooled meta-analysis and comparison between groups.
We found very low certainty evidence that the rate of new meniscal tears vary between 0% and 52%.
There is generally high risk of bias in studies reporting new meniscal tears and very low certainty of evidence. Thus, clinicians must be careful not to trust these uncertain estimates.
Acknowledgments
We acknowledge librarians Marte Ødegaard (at the Medical Library at Oslo University Hospital, Rikshospitalet) and Elin Hecker (at the Norwegian School of Sports Sciences Library) for their help with developing and conducting the search strategies. We also acknowledge biostatistician Morten Fagerland at (Oslo University Hospital and Oslo Sports Trauma Research Centre) for conducting the statistical analysis.
References
Footnotes
Twitter @clare_ardern, @hegegrindem, @larsengebretsen
Contributors All authors have contributed to planning, designing, conducting, writing and/or revising this systematic reveiw.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Professor Engebretsen has received fellowship support and research grants from Arthrex and Smith & Nephew.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.