Article Text

Abstract
Background Clinical decision-making around intramuscular tendon injuries of the hamstrings is a controversial topic in sports medicine. For this injury, MRI at return to play (RTP) might improve RTP decision-making; however, no studies have investigated this.
Objective Our objectives were to describe MRI characteristics at RTP, to evaluate healing and to examine the association of MRI characteristics at RTP with reinjury for clinically recovered hamstring intramuscular tendon injuries.
Methods We included 41 athletes with hamstring intramuscular tendon injuries and an MRI at baseline and RTP. For both MRIs, we used a standardised scoring form that included intramuscular tendon injury characteristics. We recorded reinjuries during 1-year follow-up.
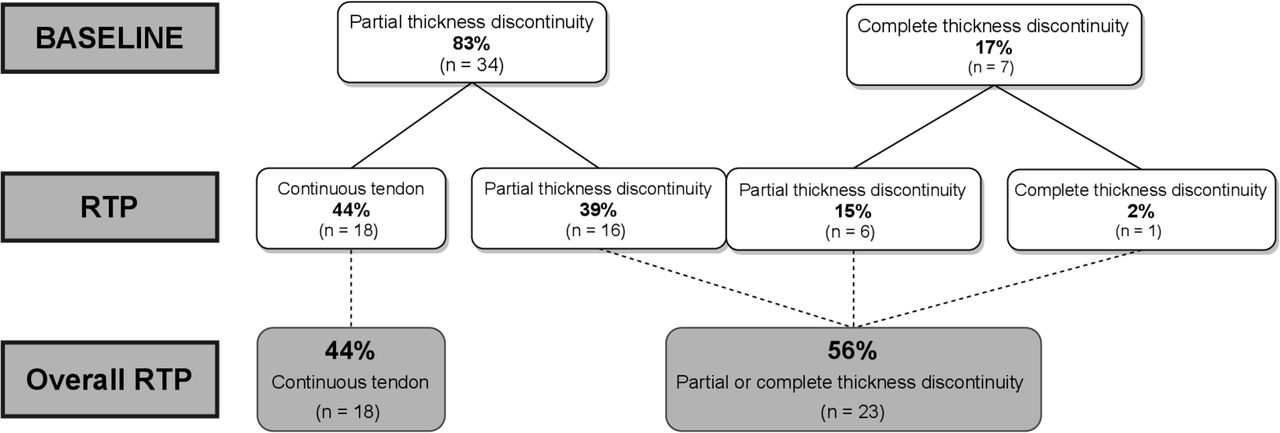
Results At RTP, 56% of the intramuscular tendons showed a partial or complete thickness tendon discontinuity. Regarding healing from injury to RTP, 18 of 34 (44% overall) partial-thickness tendon discontinuities became continuous and 6 out of 7 (15% overall) complete thickness tendon discontinuities became partial-thickness tendon discontinuities. Waviness decreased from 61% to 12%, and 88% of tendons became thickened. We recorded eight (20%) reinjuries within 1 year. Intramuscular tendon characteristics at RTP between participants with or without a reinjury were similar.
Conclusion Complete resolution of an intramuscular tendon injury on MRI is not necessary for clinically successful RTP. From injury to RTP, the intramuscular tendon displayed signs of healing. Intramuscular tendon characteristics of those with or without a reinjury were similar.
- hamstrings
- injury
- MRI
- sports and exercise medicine
- tendon
Statistics from Altmetric.com
Introduction
The clinical relevance of intramuscular tendon injuries of the hamstrings is a controversial topic in sports medicine.1–7 Studies that report return to play (RTP) duration and reinjury rates for this injury subtype vary from a mean of 25.3 (±8.6) to 84 (±49.4) days and reinjury rates from 17% to 57% for the same grade of injury.3 4 RTP decision-making is challenging and MRI at RTP might be of additional benefit in this process.8
The intramuscular tendon is defined as the part of the tendon to which the muscle fibres attach.4 At this time, we cannot clinically differentiate between a hamstring injury with or without intramuscular tendon involvement.9 However, MRI can be used to evaluate the intramuscular tendon and its direct structural changes after a muscle injury.4 5 10 The MRI characteristics of the intramuscular tendon include the affected percentage of tendon cross-sectional area (CSA), length of disruption (in case of partial-thickness discontinuity) or retraction (in case of a full-thickness discontinuity) and ‘waviness’ (indicating a loss of tension) of the tendon.4 5 10
Changes such as oedema and fibrosis are common, indirect findings (ie, sequelae) of a muscle injury on MRI at RTP in athletes who are clinically recovered from an acute hamstring injury.11 12 A recent systematic review of MRI at RTP found no strong evidence for an increased risk of reinjury with the presence of oedema or fibrosis.13 Incomplete resolution of oedema or the presence of fibrosis does not seem to prevent successful RTP. We have also investigated the relationship between MRI findings of the intramuscular tendon and time to RTP and reinjury rates.4 5 However, no studies have evaluated the clinical value of performing MRI at RTP for intramuscular tendon injuries of the hamstrings.
The purpose of this study was to examine the intramuscular tendon’s MRI appearance at RTP after an intramuscular tendon hamstring injury. Our primary aim was to describe MRI characteristics at RTP of hamstring intramuscular tendon injuries in athletes (ie, is the MRI normal?). Our secondary aims were to describe the healing of the intramuscular tendon from baseline to RTP and to compare intramuscular tendon injury characteristics on MRI at RTP of participants with and without a reinjury.
Methods
Participants
We used a combined cohort of two double-blind, placebo-controlled randomised controlled clinical trials (RCT) conducted in Qatar (Growth Factor Study, Clinicaltrials.gov NCT01812564)14 and the Netherlands (Hamstring Injection Therapy study, Dutch Trial Register 2771).15 Our study group previously performed comparable studies concerning MRI at RTP in our emerging Dutch and Qatari cohorts.11 12 The first study described oedema and intramuscular fibrosis at RTP, and its main inclusion criterium was MRI within 3 days of RTP. Participants were from the ongoing Dutch (n=29) and Qatari (n=24) RCTs.11 Since the first study had insufficient power, we did a second study to investigate whether fibrosis was associated with reinjury.12 The main inclusion criterium of the second study was MRI within 7 days of RTP. It included participants from the completed Dutch (n=80) and the still ongoing Qatari RCT (n=45). We did not investigate intramuscular tendon injuries as part of these two studies.
For the current study, we pooled data from the completed Dutch (n=80) and Qatari (n=90) trials. We only included participants with an injury to the intramuscular tendon and a combination of a baseline and an RTP MRI scan. Our study included 26 participants from the Dutch RCT and 15 participants from the Qatari RCT that overlap with our most recent study (100% and 53% overlap, respectively).12As part of the design in both RCTs, a subset of participants received a platelet-rich plasma (PRP), platelet-poor plasma injection, or saline (placebo) injection. All participants underwent standardised rehabilitation for their injury, supervised by experienced sports physical therapists. Both studies reported no significant difference in RTP times or reinjury rates between a PRP injection and a placebo alternative.14 15 These interventions have been described in detail in previous publications.4 14 15 The eligibility criteria are presented in the online supplementary appendix 1 (adapted from Reurink et al.11 12).
Supplemental material
MRI protocol
Baseline MRI was obtained within 5 days of an injury. RTP MRI was obtained within 7 days of RTP in both cohorts. MRI protocols of both RCTs have been described in detail in previous publications, and a description has been provided in the online supplementary appendix 1.4 14 15
RTP clearance
In the Dutch RCT, participants were cleared for RTP if they successfully completed the physiotherapy programme and sports-specific activities.15 In the Qatar RCT, participants were cleared by their treating sports medicine physician if they successfully and asymptomatically completed their criteria-based physiotherapy programme and sports-specific (field-based) training.14 A specialist sports-specific rehabilitator supervised this last sports-specific phase.16 If participants were cleared for RTP, they were advised to complete at least 5 days of team training before returning to partial match play.
Intramuscular tendon injury definition
We used the definition of an intramuscular tendon injury as described previously4 5 10: a partial or full-thickness injury to the intramuscular tendon(s) of the hamstrings. The appearance on MRI is characterised by a (partial or complete) loss of low signal intensity within the tendon, with or without waviness.4 We considered waviness as a part of the spectrum for the definition of an intramuscular tendon injury. The presence of waviness indicates an injury to the intramuscular tendon, but its absence does not necessarily mean the absence of an injury. For the purpose of this paper, we used the MRI appearance of an intramuscular tendon injury, and the loss of signal intensity was denoted as a discontinuity of the tendon.
Outcome measures
MRI assessment
Musculoskeletal radiologists with 15 and 2 years of experience (EA, CB) assessed MRI scans using the same standardised scoring form. Both radiologists were blinded to any clinical data or timing of the MRI (baseline vs RTP). Scoring was done sequentially in Qatar and in a random fashion in the Netherlands.
The radiologists scored the following MRI characteristics, according to previous work4 5 10: (1) most involved muscle (the muscle with the most oedema was scored as most involved), (2) the extent of discontinuity (<50, 50–99, 100% of tendon CSA), (3) the disruption length of the partial tendon thickness discontinuity (in mm), (4) the retraction length of the complete tendon thickness discontinuity (in mm), (5) waviness of the tendon (yes/no) and tendon thickening (yes/no). Tendon thickening is a descriptive umbrella term used for the radiological appearance of a tendon after a fibrotic or remodelling process (see figure 1). We did not consider thickening of the tendon to be abnormal.
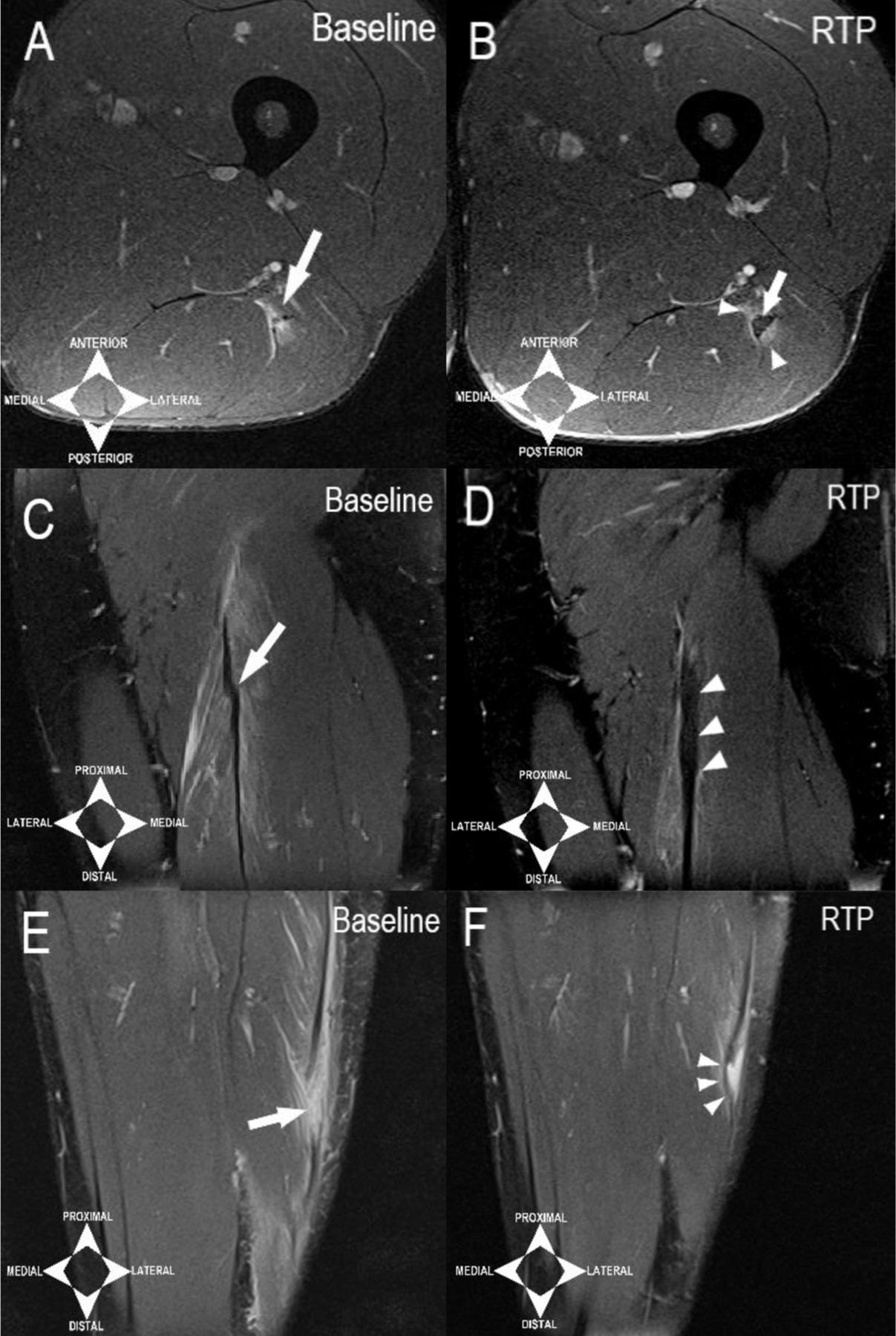
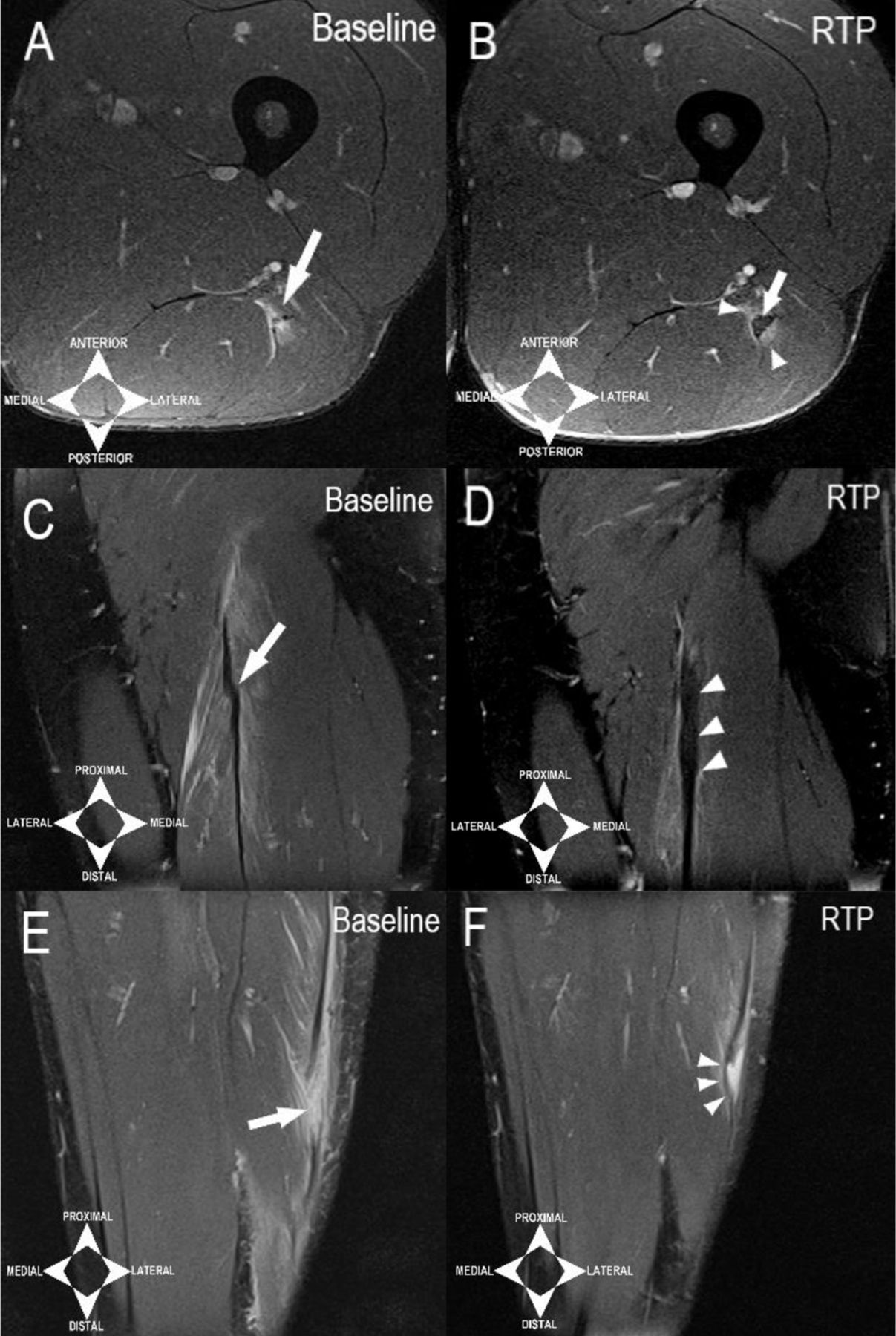
Healing of the intramuscular tendon (proton density fat suppressed (PDFS) axial and coronal MRIs). (A) Axial PDFS image from participant presenting with partial-thickness discontinuity of the intramuscular tendon of the left biceps femoris long head (arrow). (B) At return to play (RTP) MRI (axial PDFS) of (A). Intramuscular tendon appears thickened (arrow) with intermediate signal intensity within the thickened tendon (arrow) and residual peritendinous oedema (arrowheads). (C) Coronal PDFS MRI of participant presenting with partial-thickness discontinuity of the intramuscular tendon of the right biceps femoris long head with waviness and feathery oedema at the proximal myotendinous junction (arrow). (D) At RTP MRI (coronal PDFS) of (C). Intramuscular tendon appears continuous, non-wavy (taut) and thickened (arrowheads). There is minimal residual oedema at the myotendinous junction. (E) Coronal PDFS MRI of participant presenting with complete thickness discontinuity of the intramuscular tendon of the left biceps femoris with retraction and a fluid filled gap of 20 mm. It is non-wavy (arrow). (F) At RTP MRI (coronal PDFS) of (E). Previous retracted gap is being bridged with fibrotic tissue (arrowheads) and is now a high-grade partial-thickness discontinuity. No thickening is seen.
Reinjury
Reinjuries were defined as ‘an acute onset of posterior thigh pain in the same leg’.5 Participants were advised to contact the researcher in case of a (suspected) reinjury. Participants were actively followed up by phone for up to a year in both cohorts. The Dutch cohort was followed up at 1 week, 1 month, 2 months, 4 months, 6 months and 12 months after RTP. The Qatari cohort was followed up every month up to 12 months after RTP.
Statistical analysis
First, we assessed normality of the data through visual inspection of frequency histograms and, if necessary, the Shapiro-Wilk test (p>0.05) before moving forward to parametric or non-parametric testing. To describe the intramuscular tendon characteristics at RTP (primary aim) and to compare the intramuscular tendon changes from baseline to RTP (secondary aim), we used descriptive statistics and paired t-tests (or the non-parametric equivalent Wilcoxon signed-rank test). To explore a potential association between characteristics of the intramuscular tendon at RTP of participants with or without a reinjury (secondary aim), we constructed a one minus survival function (Kaplan-Meier and univariate Cox regression) using intramuscular tendon involvement at RTP as a dichotomous variable (partially/completely involved or now continuous). We used the Log Rank test to determine if there was a difference in the survival distribution of these groups. Furthermore, we constructed a one minus cumulative survival plot from the one minus survival function. We conducted the statistical analysis in SPSS (SPSS, V.21.0 for Windows). The level of significance was set at p<0.05.
Results
We included 41 participants in the analysis. The median age was 27 (IQR 22–31) years and the median RTP time was 31 days (IQR 22–42 days). Two participants were lost to follow-up after RTP: one at 87 days after RTP (no reinjury reported) and one at 51 days after RTP (reinjury reported 4 days after RTP). We excluded the participant with unknown reinjury status during follow-up from our reinjury analysis. A post-hoc sensitivity analysis showed that excluding both participants did not significantly alter any outcomes. The characteristics of the participants are presented in table 1.
Participant characteristics
Is the intramuscular tendon normal at RTP? MRI characteristics at RTP
At RTP, 56% (23) participants still had a partial or complete thickness intramuscular tendon discontinuity on MRI (table 2), with 54% (22) being a partial-thickness intramuscular tendon discontinuity, compared with 83% (34) at baseline, and 2% (1) being a complete intramuscular tendon discontinuity, compared with 17% (7) at baseline. In 44% (18) of participants, the intramuscular tendon appeared continuous at RTP (see figure 2).

Intramuscular tendon injury characteristics at baseline and return to play (RTP).
Intramuscular tendon characteristics at baseline and return to play (RTP)
Tendon healing from baseline to RTP: the changing MRI characteristics of the intramuscular tendon
The distribution of affected muscle at baseline and RTP is shown in table 2. There were no isolated semitendinosus injuries. Overall, waviness was present in 61% (25) of discontinuous tendons at baseline versus 12% (5) of tendons at RTP. Tendon thickening was present in 88% (36) of tendons at RTP and absent in 12% (5) tendons. Thickening of the tendon was seen in all the tendons that were also wavy at RTP and vice versa. We found a difference in the median disruption length from baseline to RTP (p<0.001). Six out of seven complete intramuscular tendon discontinuities at baseline demonstrated a partial thickness tendon discontinuity at RTP and were no longer retracted. One complete intramuscular tendon discontinuity at baseline remained a complete intramuscular tendon discontinuity at RTP. The retraction length of this complete tendon discontinuity reduced from 122 mm to 22 mm and it remained wavy.
MRI characteristics of participants with or without a reinjury
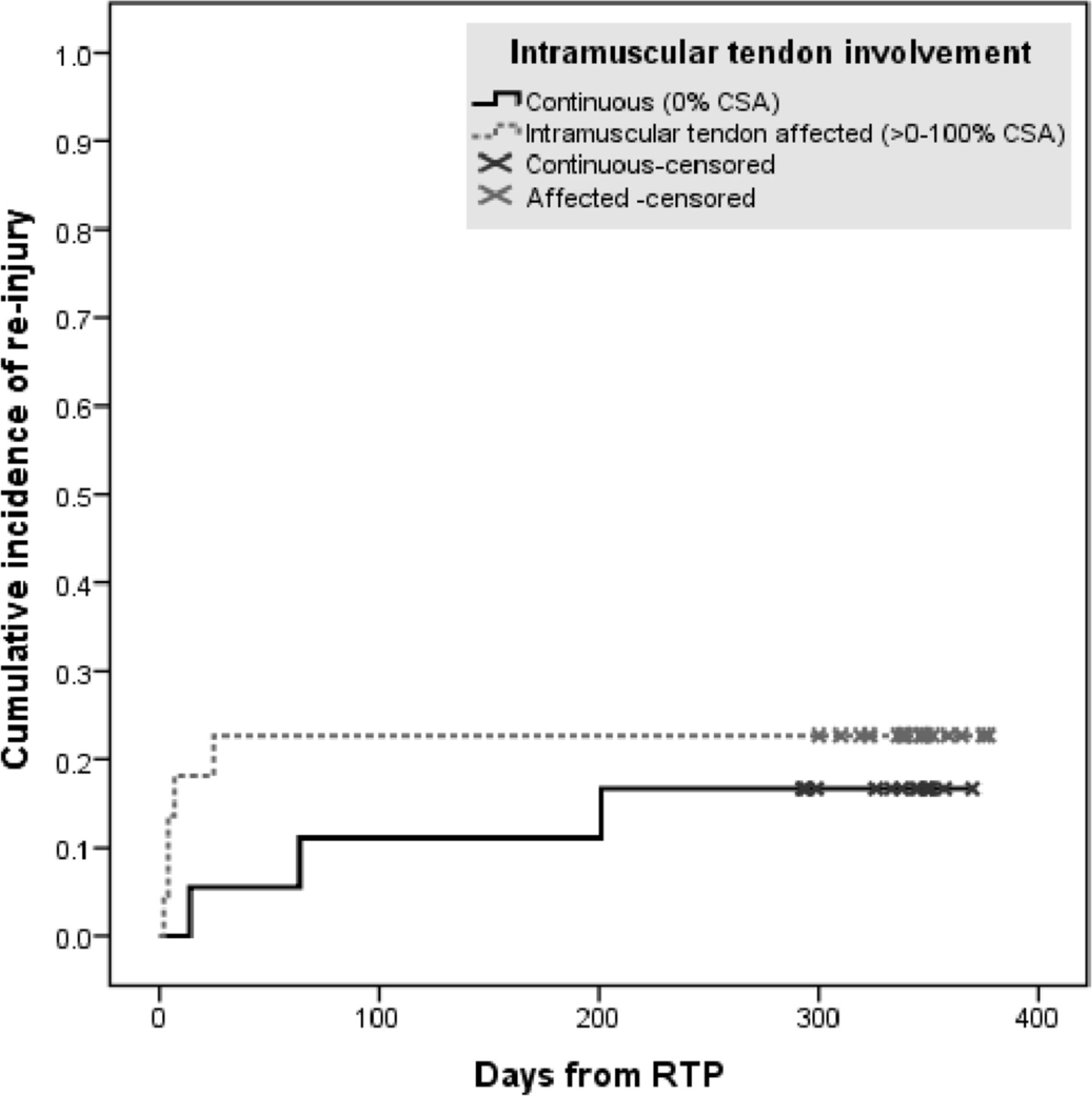
We recorded a 20% (8) reinjury rate within 1 year (with 6 out of 8 within the first 2 months). Of these reinjuries, 62% (5) had a partial thickness tendon discontinuity at RTP and 38% (3) were continuous. In participants without a reinjury, 50% (16) had a partial thickness tendon discontinuity at RTP and 47% (15) were continuous (table 3). We found no difference in reinjury rates between those with or without intramuscular tendon involvement at RTP (HR 0.65, 95% CI 0.16 to 2.73, p=0.56, see figure 3). None of the participants with a complete thickness tendon discontinuity at baseline or RTP had a reinjury in the following year. The median disruption length of the partial-thickness tendon discontinuities was 28 mm (IQR: 22–50 mm) in participants with a reinjury versus 22.5 mm (IQR: 14.1–52 mm) in those without.

{kind=link}
{kind=link}
{kind=link}
Cumulative incidences of reinjury (n=8) with involvement of the intramuscular tendon and with a continuous intramuscular tendon at return to play (RTP). We found no difference in reinjury rates between those with or without intramuscular tendon involvement (HR 0.65, 95% CI 0.16 to 2.73, p=0.56). CSA, cross-sectional area.
Intramuscular tendon characteristics at return to play of participants with or without reinjury
Discussion
The MRI characteristics of clinically recovered hamstring intramuscular tendon injuries changed significantly from baseline to RTP, but 56% of the participants still had partial or complete thickness intramuscular tendon discontinuity. From injury to RTP, the intramuscular tendon healed, with partial-thickness discontinuities becoming continuous, complete thickness discontinuities becoming partial-thickness discontinuities, waviness decreasing and thickening of the tendon. At 1-year follow-up, the overall reinjury rate was 20% (15% in the first 2 months). The proportions of affected tendon CSA, disruption length, waviness and tendon thickening between participants with or without a reinjury were similar.
MRI characteristics of the intramuscular tendon at RTP
Our study was the first to look at the intramuscular tendon and its characteristics on MRI at RTP. Previous studies investigated other, indirect MRI characteristics of acute hamstring injuries at RTP, such as oedema and fibrosis.11 12 17 For example, Silder et al 17 demonstrated that none of their participants with an acute hamstring injury had complete resolution of oedema on MRI at RTP. Similarly, we previously reported that 89% and 39% of the clinically recovered acute hamstring injuries still demonstrated hyperintensity (oedema) and/or fibrosis, respectively, on MRI at RTP.11 Although it concerns different structural changes (direct vs indirect), our current results are comparable as 56% of the participants with a clinically recovered hamstring injury involving the intramuscular tendon still have a partial or complete thickness intramuscular tendon discontinuity on MRI at RTP.
Much like the presence of oedema or fibrosis on MRI at RTP, it seems that the presence of an intramuscular tendon discontinuity on MRI at RTP cannot be reliably used to guide RTP decision-making in this cohort.11 12 18 The median RTP of 31 days in our cohort is shorter than reported in other cohorts.2 3 Reasons for this difference have been explored previously.4
Intramuscular tendon healing: changing characteristics from injury to RTP
There are no studies in the literature evaluating healing, that is, the change of intramuscular tendon characteristics from injury until RTP. Our study demonstrated the changing structural characteristics of the intramuscular tendon during rehabilitation. More than half (18 of 34) of the partial-thickness tendon discontinuities became continuous and the remaining ones (16 of 34) were less disrupted. Similarly, almost all complete thickness tendon discontinuities (6 of 7) became partial-thickness tendon discontinuities at RTP and were no longer retracted. The remaining complete thickness tendon discontinuity was less retracted. Waviness was seen in 12% of the intramuscular tendons at RTP (down from 61% at injury) indicating a restoration of tension of the tendon. Furthermore, thickening of the intramuscular tendon was a common finding (88% at RTP), likely representing a proliferative or early remodelling stage of tendon healing.19 20 This finding strengthens the hypothesis that the intramuscular tendon heals like a free tendon.7 Tendon thickening being a common finding at RTP might be problematic for the blinding in this study—by identifying this characteristic on a scan a radiologist might deduce the timing of the scan and (un)knowingly introduce bias. It remains unclear if this thickening is a persistent feature. The healing pattern of the intramuscular tendon was similar to other hamstring injury subtypes and their characteristics. For example, oedema, despite being present in almost all clinically recovered acute hamstring injuries, improved from a mean of 132 mm (±62 mm) to a mean of 77 mm (±53 mm) in length from baseline to RTP.11
Reinjuries
The overall reinjury rate after RTP of 20% (or 15% in the first 2 months) in our cohort is lower than the reported 33% by Pollock et al and similar to van der Made et al (likely due to comparable cohorts).3 5 This difference has been explored in a previous publication by our group.5 The proportions of the intramuscular tendon characteristics between participants with or without a reinjury are within the same range. This suggests that complete healing of the intramuscular tendon might not be required for successful RTP. None of the seven participants with a complete intramuscular tendon discontinuity, classically regarded as a more severe injury,8 10 sustained a reinjury in the following year. Similar to van der Made et al’s study examining baseline MRI findings of intramuscular tendon injuries of the same cohorts,5 it seemed that the group with intramuscular tendon involvement at RTP tended to reinjure earlier than those with continuous intramuscular tendons (see figure 3). However, due to the low number of reinjuries, our study was underpowered to detect reinjury differences between these groups. Future studies with a sufficient number of reinjuries should be conducted to assess relevant clinical differences.21
Strengths and limitations
The strengths of this study are the relatively high number of intramuscular tendon injuries as compared with existing literature, the prospective designs and standardised criteria-based rehabilitation protocols. The main limitation of this study is the limited amount of reinjuries in this cohort. Most participants were male football players (mixed professional and amateur) with an average RTP of 31 days. These participants were pooled from a cohort used in multiple other publications by our group that investigated different aspects of MRI at RTP but with similar conclusions. Bias due to overlap cannot be excluded. The findings in this population may not be generalisable to women and other (levels of) sports with different biomechanical demands on tendons. Using a pooled cohort of participants from two different countries could be viewed as a limitation (increased heterogeneity) or a strength (increased external validity). A part of our cohort received PRP injections. We found no difference in the healing rate in athletes with or without a PRP injection (not reported). However, our study was not designed or powered to adequately answer this question. Blinding might be compromised due to the frequency of tendon thickening found at RTP. Although most reinjuries happen early and in the same location,22 an MRI of the reinjury was not a standardisable part of the follow-up. Thus, the exact location and extent of most reinjuries were unknown.
Conclusion
At RTP, 56% of the MRIs of clinically recovered acute hamstring injuries involving the intramuscular tendon showed a partial or complete thickness tendon discontinuity. From injury to RTP, the intramuscular tendon showed signs of healing. The intramuscular tendon characteristics of participants with or without a reinjury were similar, but larger cohorts are needed for making a definitive statement regarding reinjury.
What are the new findings?
At return to play, 56% of the clinically recovered hamstring intramuscular tendon injuries showed a partial or complete thickness tendon discontinuity on MRI.
The intramuscular tendon characteristics of patients with or without a reinjury seem similar.
The intramuscular tendon undergoes considerable change from injury to return to play, reflective of healing.
How might it impact clinical practice in the future?
Complete resolution of an intramuscular tendon injury on MRI is not necessary for clinically successful return to play.
At return to play, an MRI of intramuscular tendon injuries seems of limited benefit as a part of the return to play decision-making process.
Acknowledgments
The authors would like to thank the National Sports Medicine Program medical and supporting staff of the Qatar trial and the medical and supporting staff of all the participating Sports Medicine and Radiology Departments of the Netherlands for their gracious contributions to this study.
References
Footnotes
Twitter @rbnvrmln, @RodWhiteley
Contributors RV was involved in the study design, data collection, analysis and interpretation of data and drafting of the manuscript. EA and SB were involved for evaluation of the MRI scans and drafting of the manuscript. WS was involved in data collection and drafting of the manuscript. RW, GR, AW, MM and GMMJK were involved in data interpretation and drafting of the manuscript. JLT was involved in study design, data interpretation and drafting of the manuscript.
Funding The Growth Factor study (Qatar) was internally funded by Aspetar. The Hamstring Injection Therapy (Dutch) study was supported by Arthrex Medizinische Instrumente GmbH and the Royal Dutch Football Association.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Internal Medical Ethics Board of Aspetar and Medical Ethics Committee of South-West Holland.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.