Article Text

Abstract
Prevention of ankle sprain, the most common sporting injury, is only possible once risk factors have been identified. Voluntary strength, proprioception, postural sway, and range of motion are possible risk factors. A systematic review was carried out to investigate these possiblities. Eligible studies were those with longitudinal design investigating ankle sprain in subjects aged ⩾15 years. The studies had to have measured range of motion, voluntary strength, proprioception, or postural sway before monitoring incidence of lateral ankle sprain. Dorsiflexion range strongly predicted risk of ankle sprain. Postural sway and possibly proprioception were also predictors. Therefore the preliminary evidence suggests that people with reduced ankle dorsiflexion range may be at increased risk of ankle sprain.
- lateral ankle sprain
- prediction
- dorsiflexion
Statistics from Altmetric.com
A large number of people do not recover after an ankle sprain and continue to experience disabling consequences such as functional instability, recurrence, and pain six months after injury.1,2 The development of prevention programmes or preventive behaviours is strongly related to the identification of those at high risk of sprain and/or the factors that increase risk of ankle sprain.
Several extrinsic and intrinsic factors may increase the risk of future sprain. Possible intrinsic factors include postural sway, range of motion, muscle strength, proprioception, and previous sprains. A cursory inspection of the research that has attempted to identify predictors of ankle sprains yields confusing results.3 For example, Beynnon and colleagues investigated muscle strength in two separate studies and reported an association between low inversion/eversion ratios and risk of future sprains in one study4 but not in the other.5 The same group5 reported that range of motion was not associated with risk of ankle sprain, but Pope et al6 found a strong association. Tropp et al7 found an association between increased postural sway and risk of lateral ankle sprain, but Beynnon et al5 did not.
The aim of this study was to systematically review evidence that measures of voluntary strength, proprioception, range of motion, or postural sway can predict lateral ankle sprain. A secondary aim was to quantify the risk of lateral ankle sprain.
METHODS
Inclusion criteria
Studies were included if they used a longitudinal design and investigated first or recurrent lateral ankle sprain in subjects aged ⩾15 years. To be included in the review, the study must have measured at least one of the following possible intrinsic predictors before monitoring incidence of ankle sprain: range of motion, any measurement of voluntary strength, proprioception, or postural sway. Use of surgical procedures was an exclusion criterion, although clinical trials of surgical interventions that included a group of subjects who had not undergone surgery were included.
Identification of studies and assessment of methodological quality
Studies were identified through a search of the Medline, Cinahl, Embase and SportDiscus databases from the earliest date to February 2006. The search protocols were specifically designed to identify observational studies (table 1). Key search terms were recurrence, ankle sprain, inversion, supination, and ankle injuries. No language restriction was imposed. All papers identified by the search strategy were screened independently by two researchers, and ambiguities were resolved by mutual consent.
Search strategy for the study
Quality of the studies was assessed by two researchers independently (MdN, KR) using a six item scale developed for prognostic studies by Pengel et al.8 Ambiguities were resolved by mutual consent or by a third researcher (RH) when necessary.
Data extraction and analysis
Data on the following study characteristics were extracted from eligible papers: target population, sample size, specific injury reported, and time of follow up (table 2). Measures of association between range of motion, voluntary strength, proprioception, or postural sway and risk (incidence proportion or incidence rate of ankle sprain) were also extracted when possible. The independent variables considered in the analysis were selected from those measured at baseline, before the monitoring period. All the analyses reported here were of between-individual differences as opposed to between-ankle because that was the approach used in all but one of the available publications.4 We intended to conduct a meta-analysis where more than one study provided measures of the same associations for similar populations.
Characteristics of studies included in the review
RESULTS
The search identified 7624 articles, of which 21 met all the inclusion criteria and were included in this review (fig 1, table 2). Of the 21 studies, nine reported the ankle injuries as “ankle sprains”—that is, they did not specify whether sprains were lateral or medial5,9–15,24—and two studies reported the incidents as “ankle injuries” and did not indicate what proportion of injuries were sprains, fractures, or other injuries.7,16 Only seven studies specified that the injuries were lateral ankle sprains.4,6,17–21 In some studies, subjects had a prior sprain, and recurrences were monitored, and in others subjects had no history of sprain and time to the first sprain was monitored (table 2). Two studies monitored sprain recurrences in subjects who had been admitted to the emergency room for an acute ankle sprain.22,23 One study gave no clear indication of the type of ankle injury sustained.25
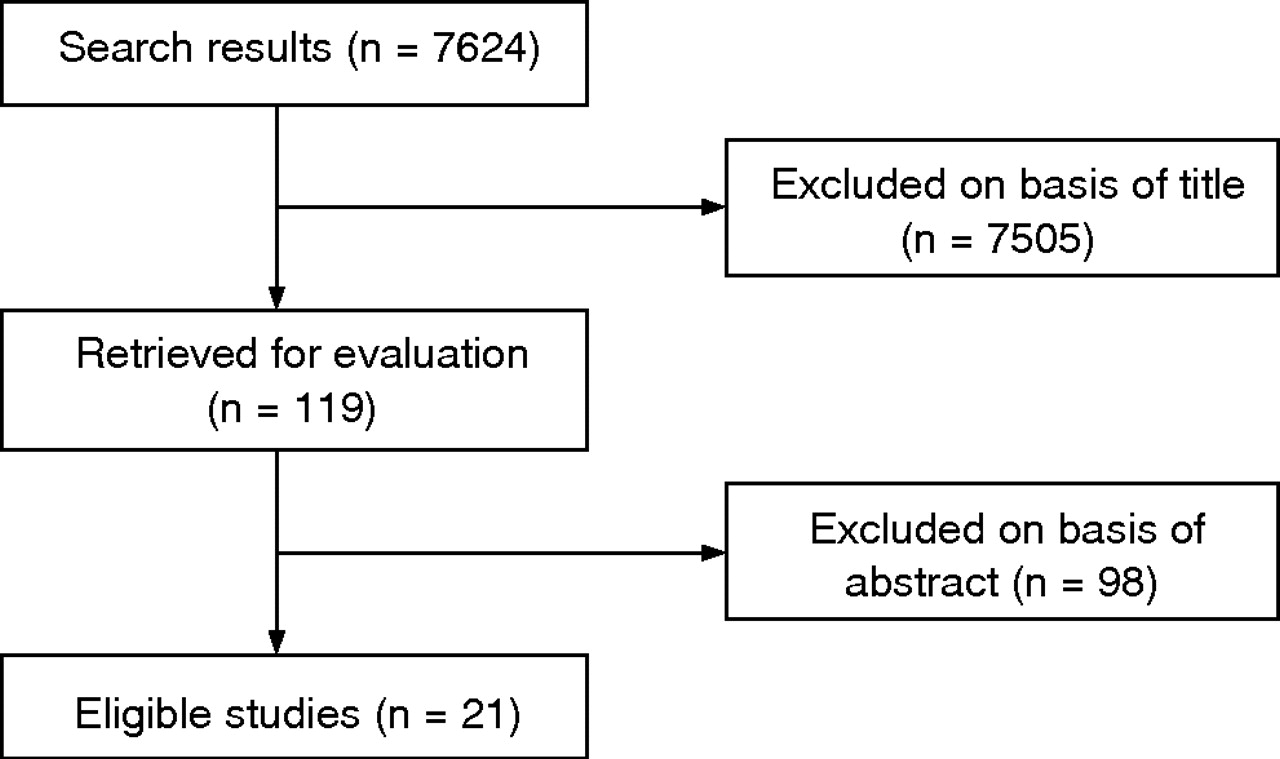
Flow chart of the search process.
The 21 included studies consisted of three randomised clinical trials6,22,23 and 18 prospective cohort studies.4,5,7,9–16,19–21,24,25 In 15 of the 21 studies,4,5,7,9–16,19,20,22,24 participants were athletes. In the other seven studies, participants were students,17,18,25 army recruits,6,21 or recruited from a mixed population.23 Because the studies were heterogeneous and the body of evidence for each outcome was too small, we did not conduct a meta-analysis.
Methodological quality
The two reviewers scored 126 quality criteria and agreed on 93 (73.8% agreement). The intraclass correlation coefficient (ICC2,1) for the total quality score was 0.42. Nine studies (43%) defined the sample, five (24%) clearly described methods for assembling a representative sample, 12 (57%) reported follow up of at least 80%, and most studies (86%) quantified prognosis. No study reported blinded assessment of outcome measures. Seven studies (33%) reported statistical adjustments (table 3).
Assessment of methodological quality
Risk of injury
Cumulative incidence proportions (the proportion of people injured at least once in a defined time) and 95% confidence intervals (CI) were reported or could be calculated for 17 of the 21 studies (fig 2). We grouped the studies according to the specificity of the reported injury (table 2). Cumulative incidence proportions varied from 0.02 at 2.8 months6 to 0.24 at 12 months.5 The remaining four studies17,18,24,25 did not present data in a way that enabled calculation of incidence proportions, although Willems et al17 reported a sprain incidence rate of 0.75 per 1000 hours of sports exposure.

{kind=link}
{kind=link}
Cumulative incidence proportion of unspecified ankle sprains, ankle injuries, lateral ankle sprains, and recurrences from 17 studies. Each data point is the estimated incidence proportion from a single study. The error bars are 95% confidence intervals.
Range of motion
Range of motion was evaluated as a predictor of ankle sprain in 13 studies.4,6,9–11,13–18,23,25 However, five of these4,10,15,18,25 only reported p values for the difference in range of motion between subjects who were subsequently injured or not injured. Baumhauer et al4 (quality score 3) reported a significantly greater baseline range of motion for subtalar eversion in the injured group.
Five studies did not report any data on the strength of the association (predictive accuracy) and therefore could not be included in the analysis.9,11,13,14,23 Two studies reported the strength of the association of ankle range of motion. Pope et al6 (quality score 5) reported that subjects with the most inflexible ankles (34° of dorsiflexion range) had nearly five times the risk of suffering an ankle sprain as subjects with average flexibility (45° of dorsiflexion range). Willems et al17 reported that risk of ankle sprain increased by about 3% per degree of range of the first metatarsophalangeal joint. Thus a subject with 2 standard deviations (30°) more metatarsophalangeal joint extension would have 2.5 times the risk of a person with average metatarsophalangeal range.17
Voluntary strength
The predictive value of voluntary strength was examined in 10 studies.4,5,9,11,15–18,21,22 Five9,11,15,16,22 did not provide data that could be used to assess the predictive value of voluntary strength for lateral ankle sprains. The remaining five studies4,5,17,18,21 presented p values for the difference in means, but not raw data on the effect of voluntary strength as a risk factor. Baumhauer et al4 (quality score 3) reported a significantly higher eversion/inversion strength ratio in the injured group, Willems et al17,18 reported stronger dorsiflexors for the injured group in female students17 but stronger dorsiflexors for the uninjured group in male students.18 No other comparison was significant in any of these studies.
Proprioception
Four studies investigated the predictive accuracy of proprioception.16–18,22 Payne et al16 (quality score 4) reported that position sense predicted left but not right ankle injury. This seems hardly credible, and may well reflect a type I or type II statistical error, so it suggests that one or both of the findings are spurious. They also reported that deficits in joint position sense in right dorsiflexion and right eversion predicted sprains, but not left dorsiflexion or left eversion, creating the same doubts about statistical validity. Holme et al22 (quality score 1) reported the number of recurrences, but did not give the strength of associations between measures of proprioception and risk of recurrence.
Willems et al17 reported better position sense for the uninjured group, suggesting that people with 2 standard deviations (about 11°) more error in sensing inversion passive position at the ankle would have about 2.3 times the risk of a person with average position sense.17
Postural sway
Seven studies measured postural sway using a force platform to determine centre of pressure displacement.5,7,12,17–19,22 Neither Leanderson et al12 (quality score 2) nor Holme et al22 (quality score 1) provided data that could be used to determine the value of postural sway as a predictor of lateral ankle sprain. Beynnon et al5 (quality score 4) compared the mean centres of pressure displacement in groups who were subsequently injured or not, but did not find statistically significant differences. Willems et al18 (quality score 3) compared 16 variables in groups who were subsequently injured or not and did not find any difference between groups except for what they called “limit of stability directional control” which they reported as being higher for the uninjured group. The analysis reported by Beynnon et al5 and Willems et al18 gives no information on the predictive accuracy of the measured variables for lateral ankle sprains.
McGuine et al19 (quality score 4) dichotomised postural sway and found that subjects with high levels of centre of pressure displacement had greater risk of lateral ankle sprain of subjects with low levels of displacement (incident rate ratio 6.7, odds ratio 10.2). They reported that subjects who suffered ankle sprains had a mean (SD) sway of 2.0 (0.32)°/s, whereas healthy subjects had a mean sway of 1.7 (0.31)°/s. Tropp et al7 (quality score 1) also presented the data in dichotomous terms: subjects had either normal or abnormal centre of pressure displacement values. From their data, we calculated that the likelihood ratio for a sprain within 12 months among people with abnormal postural sway was 3.2 (95% CI 1.8 to 5.7), and the likelihood ratio for people with normal postural sway was 0.57 (95% CI 0.37 to 0.89).
Willems et al17 (quality score of 3) measured what they called “limits of stability” (a measure of maximum distance that a person can intentionally displace the centre of gravity in standing), among other variables. They found that, in females, a 2 SD increase in the limits of stability would confer about 45% higher chance of having an ankle sprain.17
Two other studies investigated the prognostic accuracy of balance.20,24 Hopper et al20 (quality score 1) measured static balance, but did not report the type of injuries sustained. Watson24 (quality score 2) also measured balance, which he called “proprioception”. Normal performance was defined as the ability to maintain steady balance on one leg for more than 15 seconds. The likelihood ratio for people with abnormal balance performance was 2.5 (95% CI 1.3 to 4.6), and the likelihood ratio among those with normal balance performance was 0.46 (95% CI 0.30 to 0.73).
DISCUSSION
The studies reviewed here suggest that people with inflexible ankles (34° dorsiflexion range of motion) have nearly five times the risk of ankle sprain of people with an average flexibility (45°).6 Three studies7,17,24 also suggest that postural sway may play a role as a predictive factor, although estimates of the predictive accuracy of postural sway range from weak to strong. Passive inversion position sense may also be a predictive factor for ankle sprains, although only one study presented such findings.17
Few longitudinal studies explicitly stated that their main aims were to study prediction of lateral ankle sprains4,6,19–21, and in some cases prediction was clearly not the main focus of the study.6,22,23 Consequently the methodology of most studies was not the most appropriate for the purpose intended in this review. The predictive validity of predictors can be increased by determining if the predictors perform well on an independent dataset.26 Unfortunately none of the papers in this review validated their predictors on a validation set.
Not all studies treated lateral ankle sprains separately from other ankle injuries. However, two studies reported the number of lateral ankle sprains as a proportion of other ankle injuries.19,20 Hopper et al20 reported that 88.9% of their ankle injuries were lateral ankle sprains, and McGuine et al19 reported that 87% of their ankle injuries were lateral ankle sprains. It seems reasonable to expect that the proportion of lateral ankle sprains in other studies that did not present separate results for ankle sprains would be similar to those presented by Hopper et al20 and McGuine et al.19
We found evidence from two studies that dorsiflexion range of motion predicted future lateral ankle sprain.6,18 One other study investigated the same outcome and did not have the same finding,4 but this study only reported p values (not the strength of the association) and it had a relatively low methodology quality. Baumhauer et al4 also reported that decreased subtalar eversion predicted an increased risk of sprains, but, as the strength of the association was not investigated, the importance of this result remains unclear. Although more studies are necessary to confirm this finding, it appears that ankle dorsiflexion is a strong predictor of risk, at least in army recruits undergoing initial training.
Postural sway was the most widely studied factor of all the predictor variables included in this review, and yet the results are inconclusive. Nine studies5,7,11,12,17–20,22 investigated the predictive value of some form of balance measurement, but owing to inappropriate analysis, lack of data, or difference in the methods used, little can be concluded from these studies. Likelihood ratios calculated from data provided by Tropp et al7 and Watson24 provide preliminary evidence that decreased ability to balance may weakly predict future ankle sprains. Willems et al17 presented hazard ratios of 0.96 (95% CI 0.93 to 1.00) for limit of stability end point excursion and 0.94 (95% CI 0.89 to 0.99) for limit of stability maximum end point excursion. Although the methods for testing were different (standing on one leg for Tropp et al7 and Watson24 and standing on both legs for Willems et al17), this finding supports the findings that decreased ability to balance may predict future sprains. However, because there were 16 different comparisons for balance measures, this finding could be a type I error, and should be interpreted with caution.
We found no evidence that voluntary strength predicts lateral ankle sprain. Three studies4,17,18 each found one comparison to be statistically significant, but predictive accuracy was not reported in these studies, and the direction of the effect was inconsistent. Another two studies5,21 reported statistically non-significant differences between groups. The role of voluntary strength in ankle sprain therefore remains unknown.
Although impaired proprioception is widely considered to cause ankle sprain,27,28 only one study17 presented enough evidence to support such a belief. One of the studies that found sense of movement to be a predictor of ankle sprain reported that this finding held only for left ankles,16 which would appear unlikely. Willems et al17 reported that passive inversion position sense was a strong predictor of ankle sprain. As there is evidence that performance in different proprioception tests is not correlated,29 future investigations may also be directed to other aspects of proprioception, such as movement detection, as predictors of future ankle sprain.
The cumulative incidence proportions for ankle sprains in our review did not increase as the follow up time increased—that is, the incidence proportion appeared to reach a maximum of 24% at 12 months and did not increase further with increasing time (fig 2). In interpreting these findings, it is important to consider that the apparent insensitivity of risk to time could be confounded by study level or individual patient level characteristics.
Our review found that high quality investigations on predictors of lateral ankle sprain are scarce. The factors we found to predict ankle sprains are dorsiflexion range of motion, postural sway, and perhaps proprioception. These findings should be considered preliminary. Dorsiflexion range of motion appears to be the best predictor to date considering the strength of the results and the quality of the respective studies. Perhaps the key for prediction of ankle sprains is the interaction of variables such as range of motion, proprioceptive factors, and postural sway.
Acknowledgments
MdN is a scholarship holder funded by CAPES (Coordenação de aperfeiçoamento de pessoal de nível superior) from the Brazilian government.
REFERENCES
COMMENTARY
The authors have performed a systematic review of the predictors of lateral ankle sprain. As ankle sprains are the most common injury suffered during sport participation, identification of risk factors for this injury are clearly important. The authors have focused on a number of largely modifiable risk factors including range of motion, strength, proprioception, and postural control. Limited dorsiflexion range of motion and impaired postural control were found to be the strongest predictors of injury. More importantly, the weak quality of these prospective studies makes it difficult to draw conclusions. There is a clear need for high quality studies in this area to advance scientific understanding and clinical practice.
Footnotes
-
Published Online First 18 August 2009
-
Competing interests: none declared