Article Text

Abstract
This systematic review set out to identify randomised controlled trials and controlled intervention studies that evaluated the effectiveness of preventive strategies in adolescent sport and to draw conclusions on the strength of the evidence. A literature search in seven databases (Medline, SportDiscus, EMBASE, CINAHL, PEDro, Cochrane Review and DARE) was carried out using four keywords: adolescent, sport, injury and prevention (expanded to capture any relevant literature). Assessment of 154 papers found 12 studies eligible for inclusion. It can be concluded that injury prevention strategies that focus on preseason conditioning, functional training, education, balance and sport-specific skills, which should be continued throughout the sporting season, are effective. The evidence for the effectiveness of protective equipment in injury prevention is inconclusive and requires further assessment.
- adolescent
- injury
- prevention
Statistics from Altmetric.com
Sport is the main cause of injury in adolescents.1 2 Young people are at particular risk of sports injury because of high levels of exposure at a time of major physiological change.3 4 Prevention of injury is important for several reasons not least the initial impact on health and long-term outcome—that is, early development of osteoarthritis.5
Although most sports injuries are not severe enough to require hospitalisation, they are frequent and have a major economic impact through direct medical costs, treatment and rehabilitation, and indirect costs, including parents taking time off to care for injured offspring.2 6 In addition, injury prevents future involvement in physical activity, and about 8% of adolescents drop out of recreational sporting activities annually because of injury.7 There are long-term public health consequences associated with inactivity in terms of cardiovascular disease, obesity, etc, but injury may also interfere with the potential benefits of greater self-esteem, relaxation, socialisation, teamwork and fitness associated with sport participation at this age.8
Injury prevention generally focuses on modifiable risk factors: extrinsic factors, such as equipment, playing surface, rule changes and playing time, or intrinsic factors, such as fitness, flexibility and balance. This is based on adult research, but is now supported by studies of sports injury prevention in children and adolescents.
There are few systematic reviews of sports injury prevention in adolescents,6 and none focusing specifically on the adolescent age group. The aim of this review is to examine prevention strategies in adolescent sport, focusing specifically on sports that are available in schools. The specific objectives of this systematic review are:
(a) To identify randomised controlled trials and controlled intervention studies that evaluate the effectiveness of preventive strategies in adolescent sport.
(b) To make conclusions on the strength of the evidence supporting methods used to prevent injury.
METHODS
Search strategy and selection of studies
Relevant studies were identified using a computer-based literature search in seven databases (Medline 1966–January 2006, SportDiscus, EMBASE (1974–January 2006), CINAHL (1982–January 2006), PEDro and Cochrane Databases: Cochrane Review and DARE) using four keywords: adolescent, sport, injury and prevention. These keywords were expanded to capture any relevant literature:
(1) Adolescent OR youth OR (high+school+student) OR school age OR school+pupil
(2) Injury
(a) wounds AND injuries exp.
(b) sport$ injur$ OR athletic$ injur$
(c) sprain$ OR strain$ OR twist$ OR tear$ OR pull OR break$ OR fracture$ OR
(d) soft tissue injur$ Or acute injury
(e) chronic injur$ OR overuse injury OR cumulative trauma OR repetitive trauma OR tendonitis OR tendinopathy
(f) concussion OR head injury
(g) major trauma OR catastrophic injury OR death
(3) Sport
(a) explode sports
(b) sport$ OR exercise OR athletic$ OR physical education OR school games
(c) hockey OR rugby OR football OR soccer OR swim$ OR tennis OR squash OR badminton OR basketball OR netball OR Gaelic football OR GAA OR camogie OR hurley OR hurling
(4) Prevention
(a) primary+prevention
(b) protective+equipment OR protective device OR safety device OR taping OR brace$
(c) supervision OR rule enforcement OR rule change$ OR competition+rules
(d) sport$+facilities OR sport$+grounds
(e) size+matching OR age-matching
(f) warm-up OR warm-down OR pre-season+preparation OR pre-season+training OR resistance+training OR weight+training OR strength+training. The Cochrane Filter was applied.
In the first stage of selection, the titles and abstracts of all studies were assessed for the criteria below. Full text articles were retrieved for potentially relevant studies where no abstract was available, where the cohort age was unclear from the abstract, and where the abstract suggested selection. There was no blinding to study author, place of publication or results. Hand searches of study bibliography identified a further 62 potentially relevant publications that were subsequently retrieved and assessed. The primary reviewer (LA) assessed the content of all full text articles, making the final inclusion/exclusion decisions on the basis of criteria described below.
Selection criteria
Types of study
Randomised controlled trials, non-randomised intervention studies and cohort studies, published in English, were considered.
Types of participants
Adolescents (12–18 years) involved in supervised physical education and sport. This includes the usual range of school sports in Ireland (athletics, hockey, rugby, football, swimming, tennis, squash, badminton, basketball, handball, netball, gaelic football, camogie, hurling and lacrosse). It excludes sports that only a minority have the opportunity to experience—for example, equestrian sport, water sports, snow boarding, skiing, ice hockey, skating and motorised sport. It excludes unsupervised sports—for example, roller-blade and skate sports—and “extreme sport” activities. Both acute (fractures, soft-tissue injuries, concussion, head injuries, major trauma, death) and chronic injuries were included. Studies that included both adult and adolescent participants were included if the adolescent age group could be identified and studied separately.
Types of intervention
Studies examining the effect of any preventive intervention—for example, protective equipment, specialist coaching, conditioning or neuromuscular training—were included. Control interventions included no intervention or other interventions.
Types of outcome measured
Injury was the outcome measured and defined as:
(1) Injury rate (per participant, per 1000 exposures or per 1000 exposure hours).
(2) Injury severity (time missed from sport participation, training practice or match because of injury).
(3) Where possible, individual study effect estimates were calculated—that is, risk ratios (RR) each with 95% CI.9
Note that recording of injury by participants or observers was acceptable for inclusion purposes.
Validity assessment
The two authors (LA and CB) independently assessed the methodological quality of each study. We were not blinded to the identity of authors, institutions and journals. Agreement was reached by consensus regarding the methodological quality of all studies. As no validated tools exist to evaluate or rate studies that are not randomised controlled trials, we developed a quality assessment key to score the studies (table 1). This key was based on keys used by the Cochrane Collaboration Injuries Group and the Cochrane Collaboration Bone, Joint and Muscular Trauma Group. We piloted the key independently, modified it by consensus, and used it to score all included studies. For the purposes of this review, studies were rated for quality by application of a system described by MacKay et al6 whereby a score for overall quality was converted into a percentage value—that is, 0–49% is poor, 50–89% moderate, and >90% good (table 2).
Data extraction
We (LA, CB) independently extracted data on the study characteristics, study population, interventions, analyses and outcome. Studies were first assessed for homogeneity with respect to the nature of the intervention, control group, and the type and timing of outcomes and follow-up.
Study characteristics
Tables 3–5 summarise the study characteristics.
Quantitative data synthesis
Table 6 gives quantitative data synthesis with results.
RESULTS
Trial flow
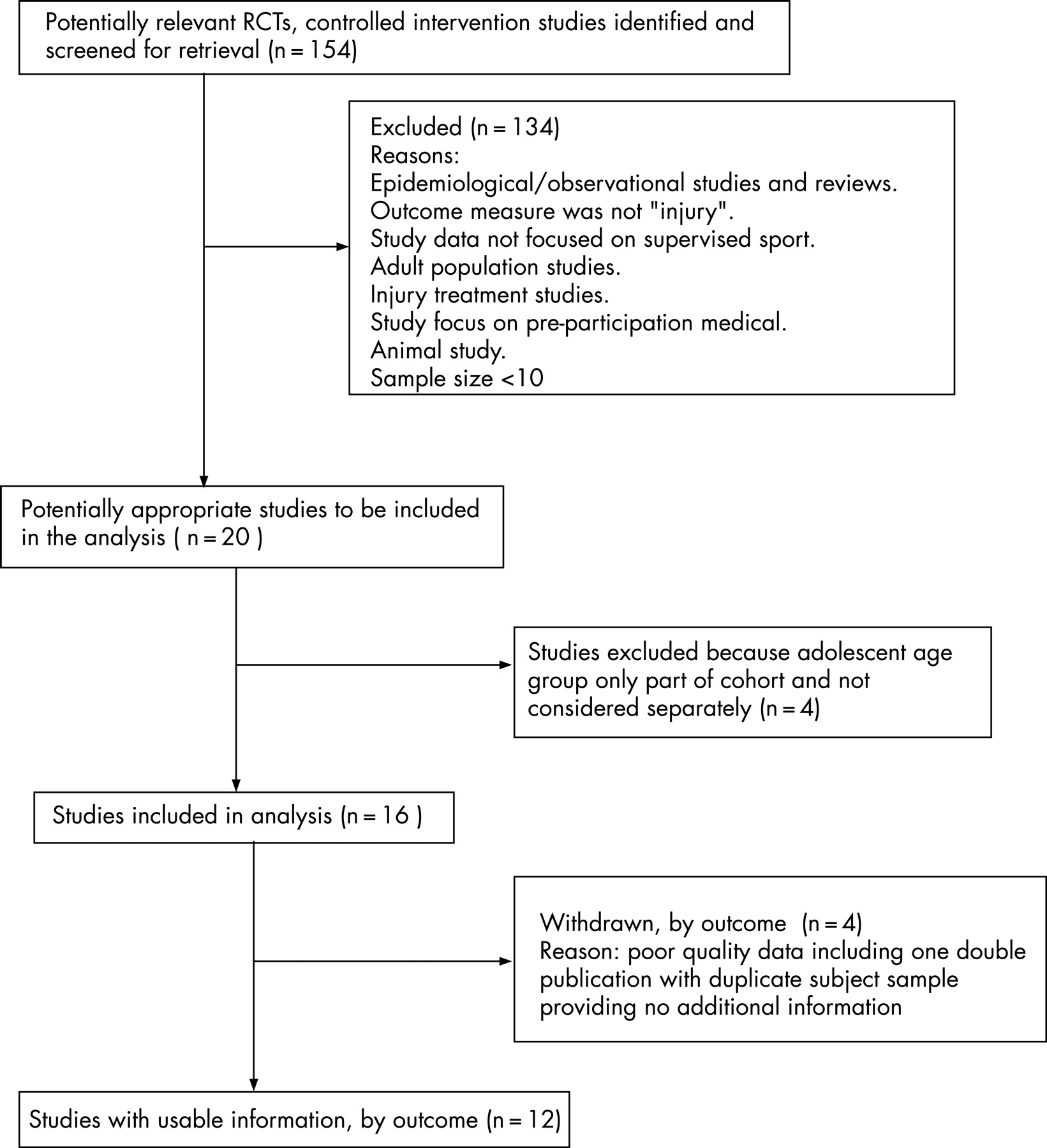
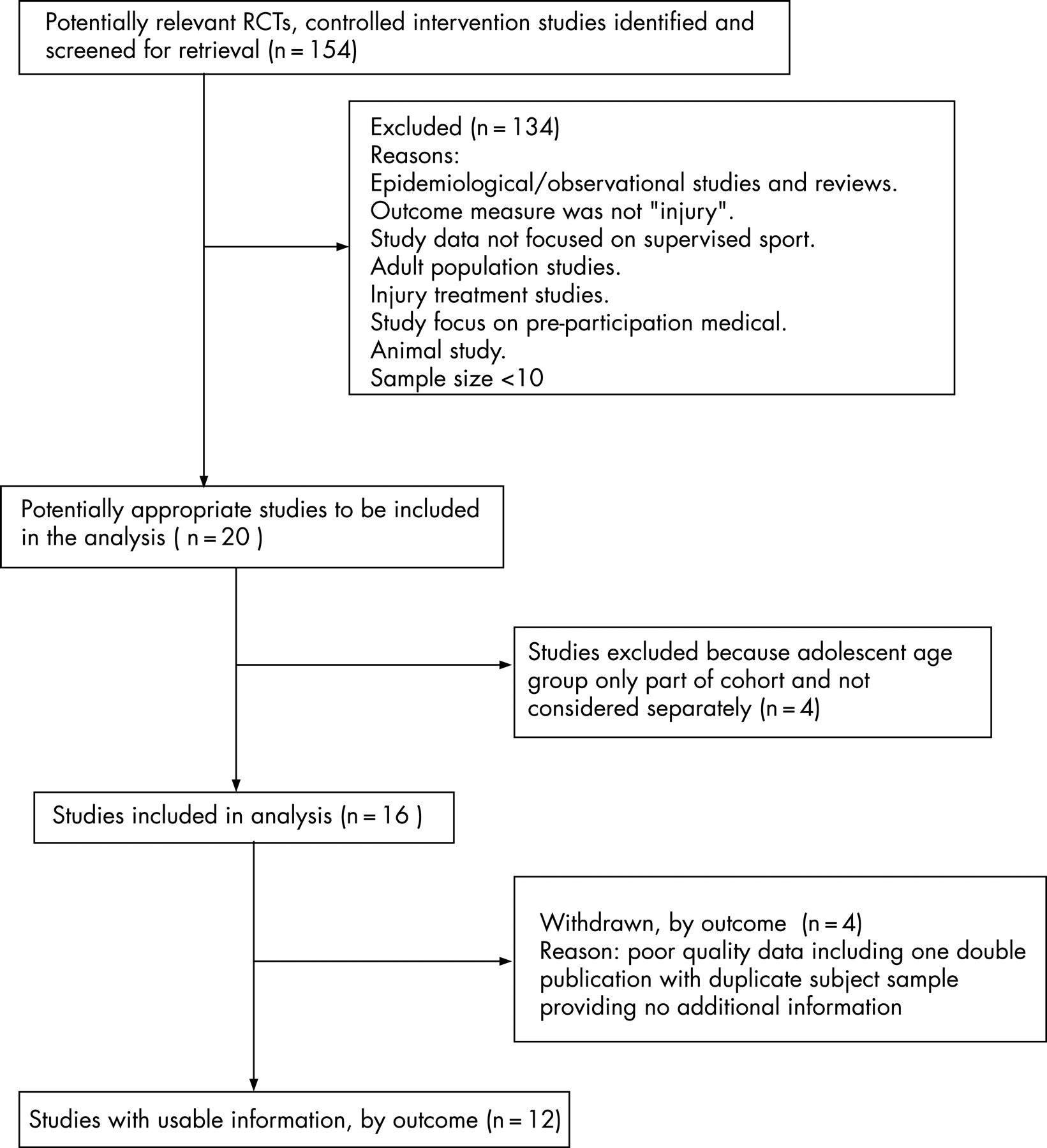
The process of study selection and explanations of exclusions at each stage are reported according to the Quality of Reporting of Meta-Analysis (QUORUM) statement flow diagram10 (fig 1). From the initial list of citations yielded in the literature search, 154 studies were included. After review of the complete texts, 142 studies were excluded, leaving 12 eligible studies for inclusion in this review.
{kind=link}
Study characteristics
Injury-prevention studies fell into two groups: the effect of use of protective equipment; the effect of preseason conditioning programmes and injury-prevention strategy that continued throughout the season. Results will be discussed in these study groupings.
Outcome measures
The definition of injury varied across studies. In certain cases “injured subjects” could still have been actively involved in their sport; for example, Yang et al11 used the definition “any new injury that required medical attention or restricted participation on the day after the injury”, whereas Webster et al12 used the definition “any injury involving the head or face”, and Grace et al13 used the simple definition “any lower limb injury that limited participation”. In the majority of studies,14–18 however, only subjects that missed one or more days’ participation in sport were described as sustaining an injury. Two studies19 20 focused solely on the incidence of knee injuries, with one19 counting only knee injuries significant enough to seek care from an athletic trainer and leading to >5 days lost time from practice. Mandlebaum et al20 focused on anterior cruciate ligament (ACL) injuries, using diagnostic confirmation from MRI and arthroscopy.
The methods used to collect injury data and verify the injury lacked consistency. In the majority, athletes subjectively reported their injury, by using questionnaires or by relaying information to a nominated reporter, coach, investigator, physiotherapist, nurse or doctor. Only half of the studies followed up subjective reports with a physical examination by a doctor, physiotherapist or athletic trainer,13 16 17 19 21 22 and only one study opted to use further diagnostic imaging.20
Protective equipment
Four studies11–13 17 monitored the benefits of various forms of protective equipment throughout a range of sporting environments. All of these studies achieved a poor rating on quality score (<50%). A 2-year study13 found that hinged knee braces were not effective at reducing knee injury in high school American footballers, and were even associated with an increase in ipsilateral ankle and foot injuries. A larger study by Yang et al11 using athletes from 12 different sports also found that both knee and ankle braces increased lower limb injury rates, but the use of knee pads was associated with a significant reduction. McIntosh and McCrory17 found that headgear (scrum caps) could not reduce the incidence of concussion occurring in junior rugby union players over a single playing season, whereas the cohort study of Webster et al12 on lacrosse players over two seasons found that eye goggles reduced the number of head and face injuries, particularly during competition.
In summary, there is limited evidence that eye goggles and knee pads can reduce the incidence of head and face (RR = 0.52)12 and knee (RR = 0.44)11 injuries, respectively, and there is currently no evidence to suggest that headgear (RR = 1.05)17 and knee braces (RR = 2.24)13 have a positive effect on injury prevention.
Preseason conditioning
Hewett et al19 used a preseason conditioning strategy to develop flexibility, strength, power and landing mechanics. Using a sample of female soccer, volleyball and basketball players, he found that 6 weeks of this preventive intervention (three sessions a week) decreased the number of serious knee injuries over the next sporting season. Although this study used a large sample size (n = 1263), it scored poorly on the quality scale (<50%), and subjects entered into either the intervention or control group on a voluntary basis. Moreover, the effect of this strategy on other lower limb injuries is not clear.
Heidt et al15 carried out a similar study, but used a randomised controlled study design with moderate quality (11/18), using a smaller group of female soccer players. The study randomised subjects to either a 7-week conditioning programme designed to improve sports-specific cardiovascular fitness, lower limb strength, flexibility and power or to a control group receiving no preseason intervention. A 1-year (two seasons) follow-up showed that the injury rate of the conditioning group was significantly lower than that of the control group.
In summary, there is poor evidence from one cohort study and moderate evidence from one randomised controlled study that 6 weeks of preseason conditioning can significantly reduce injury rate in female athletes (RR = 0.2519, RR = 0.4215).
Injury prevention strategies throughout the playing season
Proprioceptive training
Three studies14 21 22 using cluster randomisation and scoring moderately (10/18) on the quality scoring scale examined the effectiveness of various balance-training protocols. Emery et al14 found that a home-based proprioceptive balance-training programme (daily for 6 weeks, then weekly for a further 5 months) using a wobble board improved static and dynamic balance in healthy adolescents and reduced the incidence of self-reported injury over a 6-month period. Similarly, Wedderkopp et al21 found that female handball players using an ankle disc in conjunction with functional strengthening at each practice session were less likely to be injured than a control group (training as normal). A follow-up study by the same group22 using similar methods and population provided evidence that the combination of ankle disc training and functional strengthening is more effective at reducing injury incidence than functional strengthening alone.
Structured warm-up
Three trials16 18 20 of moderate quality studied the cumulative effect of using a range of injury-preventive strategies during the playing season. Olsen et al18 block-randomised handball clubs in Norway to either a control intervention (training as normal) or an intervention group that used a structured 20-min warm-up before each training session. The warm-up consisted of lower limb proprioception, strengthening exercises and technical training, with all athletes encouraged to maintain optimal lower limb alignment and control. This study, which scored highest on methodological quality rating (13/18), found that fewer knee and ankle injuries occurred in the intervention group during the one-season follow-up period. Furthermore, a prospective cohort study20 found that a structured warm-up emphasising strengthening, stretching, plyometrics and soccer-specific agility was significantly more effective than a traditional warm-up at reducing ACL injuries in female soccer players. A more generic preventive programme (including education, warm-up, cool-down, taping, rehabilitation, flexibility and stability) delivered in the 1-year cohort study of Junge et al16 was also effective in reducing male soccer injuries.
In summary, there is moderate evidence that all the reviewed injury-prevention strategies carried out throughout the playing season prevented injury (RR 0.2–0.73, table 6).
Quantitative data synthesis
Tables 1 and 2 describe the quality scoring key and study quality scores respectively. These tables illustrate that there was no good quality study scoring 16 or more, but seven moderate studies scoring between 9 and 15, and five poor quality studies scoring less than 9. There were several criteria that consistently limited the quality of studies: none of the included studies carried out allocation concealment, and only one was considered to have performed sufficient randomisation; however, six additional studies demonstrated acceptable “cluster randomisation”.
We assessed the treatment effect by (1) considering preventive strategy in relation to the risk, type and severity of injuries, (2) considering the feasibility of replicating the intervention used, and (3) calculating the number needed to treat (NNT) to prevent one injury. Treatment effect in terms of NNT was calculated where there were sufficient data and is given in table 6.
DISCUSSION
Protective equipment
Headgear
Headgear is designed to attenuate the impact energy of an insult to the head. In this review, McIntosh and McCrory17 found an increase in the rate of head injury with the use of protective headgear. It may be that the type of material used in headguards cannot withstand the high impacts associated with collision sports. Alternatively the findings may reflect the competitive nature of sport and the potential influence of protective equipment on behaviour. It has been proposed that wearing pads or headguards can cause “risk compensation” or “risk homoeostasis” whereby athletes act in a riskier manner than usual because of the sense of increased protection.23 24 Although a recent case-controlled study (n = 674)25 seems to refute this theory, finding no association between the use of protective equipment and risk-taking activity in children, the inclusion of younger children (8–18 years) may have led to bias.
The use of mouthguards is another commonly used preventive strategy in contact sports. Studies on adults have shown that mouthguards can prevent injury in rugby union26 27 and other contact sports.28 Similar studies on adolescents have been undertaken, but they failed to meet the inclusion criteria for the current review. High-quality studies are therefore required to make definitive conclusions on the effectiveness of headgear and mouthguards and their influence on risk-taking behaviour in adolescents.
Bracing
We found an increase in injuries associated with the use of protective external bracing, whereas kneepad use was associated with a reduction in lower limb injury.11 13 Primarily, it must be noted that the included studies scored poorly on study quality rating, and both failed to use any form of randomisation. Brace use in all included studies was based purely on individual preference, therefore a number of other confounding factors may have contributed to the injury incidence. Indeed it has been suggested that subjects opting not to wear a brace are more likely to be risk takers, whereas “brace users” might be more risk adverse.29 Other personality traits—for example, type A personality or levels of exercise dependence—can also act as a precursor to sustaining injury,30 and although this conjecture may not explain the present results, it does highlight the importance of using adequate randomisation procedures in future studies.
Notwithstanding the methodological flaws, an increase in injury was associated with the use of protective bracing, which agrees with earlier reports.31 Although there is some evidence from cadaver studies that knee bracing does offer protection to knee ligaments under external load,31 32 this effect may not carry over to the high-velocity, multidirectional forces encountered during sporting activity. Others have found that bracing can lead to increased muscle fatigue,33 and it has also been linked to decreased athletic performance,33 factors that may cumulate to increase the injury risk.
What is already known on this topic
Sport is the main cause of injury in adolescents.
Adult studies have identified that injury can be prevented by using protective equipment and improving fitness, flexibility and balance.
However, injury-prevention strategies that focus specifically on the adolescent age group have not been reviewed.
What this study adds
There is significant and consistent evidence in the literature to support the use of injury-prevention strategies in adolescents that include preseason conditioning as well as functional training, education, strength and balance programmes that are continued throughout the playing season.
The evidence for protective equipment in injury prevention in adolescents is inconclusive and requires further assessment.
Pragmatists argue that the potential benefits of taping and bracing are related to enhancing sensorimotor control rather than providing mechanical constraint, but the evidence to support this remains contradictory. There is some evidence to show that knee bracing can enhance sensorimotor control in subjects with a history of knee injury,34 35 but the effect is lessened with more demanding functional tasks, and the clinical benefits of such small changes have also been questioned.35 A review by Beynnon et al36 found that the application of an elastic bandage can enhance joint positional sense in knees with an ACL tear, and a cohort study also supports the use of knee bracing in preventing re-injury during skiing.37 Generally, however, the effects of bracing on sensorimotor control seem less definitive in healthy subjects,38 and a systematic review39 found no consistent evidence of effectiveness for knee bracing in reducing knee injury in adult and adolescent sports people. Further randomised studies must assess the effectiveness of bracing in preventing primary injury in adolescents.
Preseason conditioning and preventive strategies continued throughout the playing season
Conditioning programmes that include strength, flexibility, balance, and sport-specific fitness and technique training prevent lower limb injury. This benefit appears to be optimised when the preventive programme is continued throughout the playing season. This finding is consistent with adult studies that showed significant reductions in ankle sprain on introduction of preventive programmes in volleyball.40–42 Similarly preventive programmes in football (soccer) produced a 50–75% reduction in injuries in general43 and a significant reduction in ACL injuries.44
Conversely our findings do not agree with a review of the impact of stretching on sports injury risk.45 Studies that focus on stretching alone or stretching plus warm-up and cool-down strategies—for example, a stretching protocol performed during pre-exercise warm-up—did not produce clinically meaningful reductions in risk of exercise-related injury in army recruits,46 47 and half-time stretching exercises performed by high school footballers did not reduce the incidence of match injuries.48 Furthermore, research on running injuries49 50 indicates that injury incidence is not reduced by preventive strategies such as stretching, warm-up and cool-down. This could be explained by the pre-study practice of participants—that is, they were already undertaking some form of pre-exercise programme that included these aspects and therefore the intervention studied was not sufficiently different to demonstrate an effect change. An additional consideration may be that recreational and distance runners are not an equivalent population group, and caution should be exercised in extrapolating results to this setting.
It may be that the functional components of the preventive programme—that is, conditioning, proprioceptive balance training and skills training—are responsible for producing the physiological adaptations that help to prevent injury in the adolescent population.
In summary, we found that the evidence for using protective equipment—that is, bracing, taping and headgear—is inconclusive and hampered by confounding factors that are difficult to control for. There is poor evidence to support the protective effect of knee pads and eye goggles. However, there is significant and consistent evidence to support injury prevention strategies that include a combination of the following elements: preseason conditioning, functional training, education, strength, and proprioceptive balance training programmes that are continued throughout the playing season. The risk reduction is broadly similar for all strategies studied. The NNT to avoid an injury ranged from 4–10 for all injuries (table 6) to 66 for serious injury—that is, ACL injury.19 Clearly no “one value” for NNT can be deemed worthwhile.9 However, it would seem acceptable that 10 adolescents should be trained in such a way as to avoid one minor injury. Similarly a training programme that could prevent a season-threatening, if not career-threatening, injury such as an ACL rupture with a NNT of less than 100 would normally be considered acceptable. Furthermore, the intervention programmes described could easily be reproduced and applied across many sports. A significant proportion of the programmes are probably current practice in many training sessions, and adaptation to include aspects such as proprioception does not carry a major educational or financial implication.
CONCLUSION
The development and application of injury prevention strategies that focus on preseason conditioning, functional training, education, proprioceptive balance training and sport-specific skills, which should be continued throughout the sporting season, are effective. The evidence for protective equipment in injury prevention is inconclusive and requires further assessment.
Acknowledgments
We thank Diurmuid Kennedy and Angela Thompson, Queens University Medical Library, for advice and help with database searches, and Domhnall MacAuley for editorial advice.
REFERENCES
Footnotes
Competing interests: None.
- Abbreviations:
- ACL
- anterior cruciate ligament
- NNT
- number needed to treat