Article Text

Abstract
This review summarises the existing knowledge about pathogenesis, differential diagnosis, conservative treatment, surgery and post-surgical rehabilitation of sports hernias. Sports hernias occur more often in men, usually during athletic activities that involve cutting, pivoting, kicking and sharp turns, such as those that occur during soccer, ice hockey or football. Sports hernias generally present an insidious onset, but with focused questioning a specific inciting incident may be identified. The likely causative factor is posterior inguinal wall weakening from excessive or high repetition shear forces applied through the pelvic attachments of poorly balanced hip adductor and abdominal muscle activation. There is currently no consensus as to what specifically constitutes this diagnosis. As it can be difficult to make a definitive diagnosis based on conventional physical examination, other methods, such as MRI and diagnostic ultrasonography are often used, primarily to exclude other conditions. Surgery seems to be more effective than conservative treatment, and laparoscopic techniques generally enable a quicker recovery time than open repair. However, in addition to better descriptions of surgical anatomy and procedures and conservative and post-surgical rehabilitation, well-designed research studies are needed, which include more detailed serial patient outcome measurements in addition to basing success solely on return to sports activity timing. Only with this information will we better understand sports hernia pathogenesis, verify superior surgical approaches, develop evidence-based screening and prevention strategies, and more effectively direct both conservative and post-surgical rehabilitation.
Statistics from Altmetric.com
Among professional sports players, the estimated incidence of groin pain is 0.5–6.2% and it is more common among ice hockey and soccer players.1–5 Among male soccer players the incidence of chronic groin pain is 10–18% per year.6 7 In sports such as soccer, ice and field hockey, tennis, and Australian Rules football, groin injuries may represent 5–7% of all injuries.8 9 Injury data from the National Hockey League reveals that 13–20 per 100 players per year sustain a groin injury.10
Sports hernia has been described as a common diagnosis in otherwise unexplained chronic groin pain.11 Some authors believe that it is the most common cause of chronic groin pain in athletes, whereas others consider it to be quite rare.12–17 Gilmore18 suggested that the incidence of chronic groin injury has increased with the greater intensity of modern athletic play, but others have suggested that the increased injury frequency is attributable to the heightened awareness among athletic trainers and doctors of the condition .5 19
The sports hernia is one of the least understood, poorly defined and under-researched maladies to affect the human body. The media has popularised the use of this diagnostic term, but the actual injury characteristics are poorly identified.20 The sports hernia reflects a compilation of diagnoses grouped together with a wide range of other pathologies that need to be excluded before this should be considered as a diagnosis.20 There is a paucity of sports hernia verification through surgical textbooks, anatomical drawings or pictures.20 21
The aetiology, onset (chronic versus acute), anatomy involved and terminology used to define a sports hernia varies widely in the literature.22 23 Geographical and sports-specific differences seem to exist for the overdiagnosis or underdiagnosis of a sports hernia, with European soccer players with chronic groin pain more often diagnosed with a sports hernia and Australian Rules Football players with chronic with chronic groin pain more often diagnosed with osteitis pubis.22 24–26 Fredberg et al27 suggested that proper evidence does not exist for the theory that a sports hernia constitutes a credible explanation for chronic groin pain, calling for greater restraint before surgical intervention.
The groin disruption syndrome described by Gilmore, including injury to the internal oblique aponeurosis, conjoined tendon-pubic tubercle attachment and dehiscence between the conjoined tendon-inguinal ligament, have been grouped together as inguinal wall and superficial inguinal ring disorders.2 18 20 28 Posterior inguinal wall deficiency occurs as a result of injury to the transversalis fascia or conjoined tendon, which is formed by the medial portion of the internal oblique and transversus abdominis muscles.8 19 21 29
Many reports define a sports hernia as a bulge or incipient posterior inguinal wall hernia that creates lower abdominal or groin pain, leading to loss of inguinal canal integrity without the presence of a true hernia.4 8 30–32 Other sports hernia descriptions have included abnormalities of the rectus abdominis muscle, avulsion of part of the internal oblique muscle fibres from the pubic tubercle, tearing within the internal oblique muscle, or abnormality in the external oblique muscle and aponeurosis,33–35 as each of these conditions may also dilate or weaken the inguinal wall or ring.11 Anterior inguinal wall defects have also been identified via surgical exploration in up to 80% of athletes who experience chronic groin pain.2 36 37
Most sports hernias occur in male athletes, although they may also occur in female athletes.32 38 Harmon38 may have provided the most accurate sports hernia definition, describing it as “the phenomena of chronic activity-related groin pain that is unresponsive to conservative therapy and significantly improves with surgical repair”. However, surgical success is usually interpreted as return to sports activity timing.9 29 Verrall et al9 reported how misleading the return to sports activity timing can be in assessing patient outcome after sports hernia treatment intervention. Slavotinek et al39 reported that only a small proportion of athletes with groin pain miss games, owing to their high motivation to maintain their position within a team.
The purpose of this systematic literature review paper is to summarise sports hernia pathogenesis, differential diagnosis, conservative treatment, surgical treatment and post-surgical rehabilitation.
LITERATURE SEARCH
We performed a comprehensive Medline literature search to identify all English-language papers on sports hernia between 1950 and the second week of April 2008. Review articles and case series were included to help define the nature of the sports hernia diagnosis and because of the limited number of clinical studies concerning this topic. Search terms included all combinations for “sports or sportsman’s hernia”, “chronic groin pain”, “chronic groin injury” and “athlete”. Retrospective and nonrandomised studies were included as they comprise the majority of literature on the topic of sports hernias. The search term “sports or sportsman’s” hernia with or without the term “athlete” generated 33 papers. The search term “chronic groin pain” with or without the term “athlete” generated 75 papers. The search term “chronic groin injury” with or without the term “athlete” generated 39 papers. Papers that focused on tendon conditions or that were based primarily on true hernias were not included in this review. After correction for redundancies, 104 papers were identified to contribute to this review.
CHARACTERISTICS OF SPORTS HERNIA
Pathogenesis
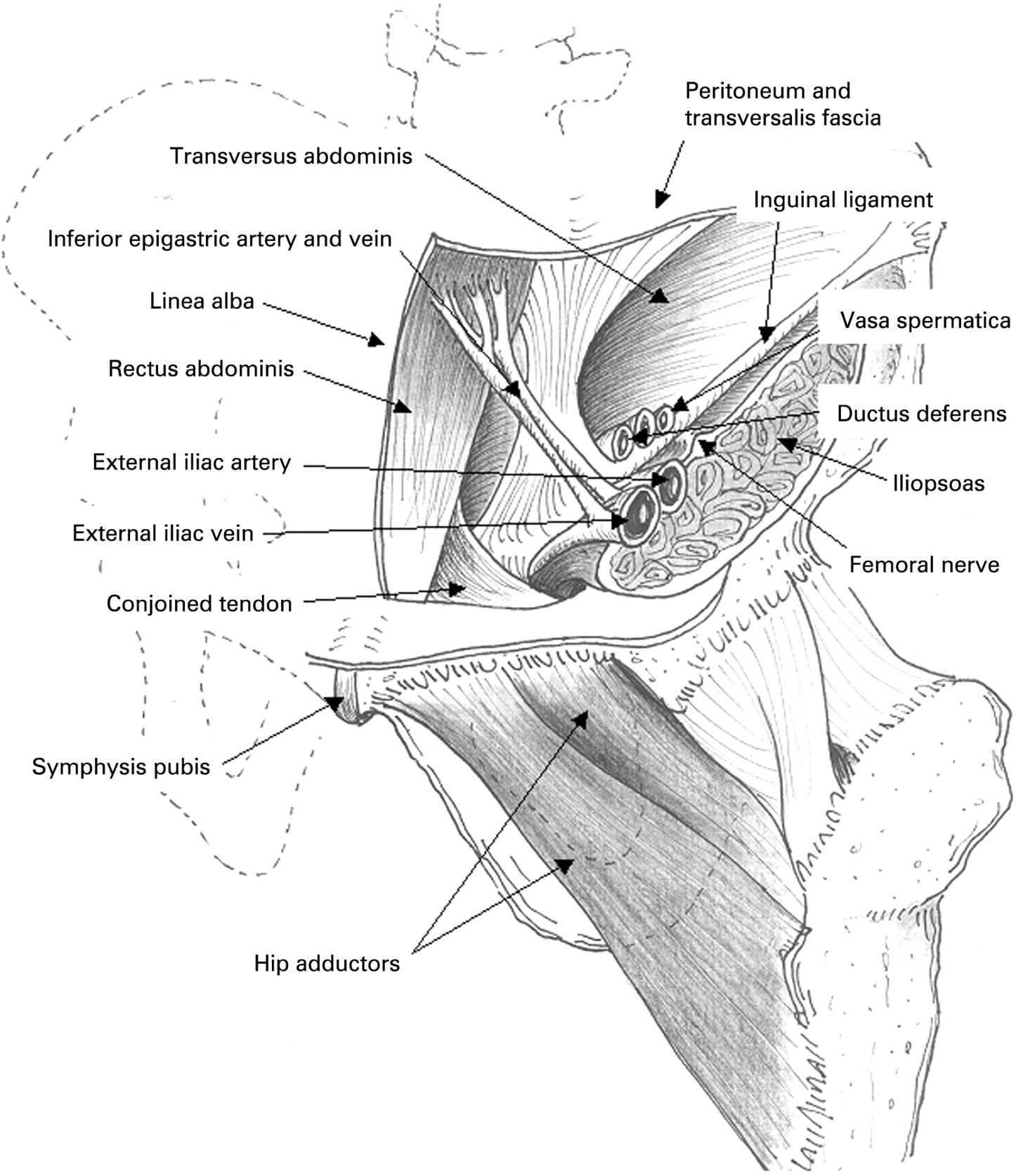
Chronic groin injury may develop from overuse, increased shear forces across the hemipelvis, lumbopelvic and leg muscle strength, endurance, extensibility and coordination imbalances, loss of dynamic abdominal wall rotational stability, or congenital inguinal wall weakness.7 40 The close proximity of numerous anatomical structures in the region in which sports hernias develop results in the strong likelihood of coexisting conditions7 (figure 1). Alternatively, an initial musculoskeletal groin injury may alter delicate hip and groin region musculoskeletal biomechanics, leading to sports hernia onset as a secondary injury.7 23 26

{kind=link}
Repetitive or excessive shear forces applied through the pelvis from the hip adductor muscles pulling against a fixed leg may weaken or injure the internal oblique or transversalis fascia attachments from the inguinal ligament. The transversus abdominis muscle and fascia normally functions as an inguinal canal “shutter” mechanism when the muscle contracts, and the activation onset of this muscle may be delayed in athletes who experience chronic groin pain.20 41
Reduced hip abduction and internal–external rotation range of motion (ROM) has been associated with chronic groin injury and also with transversalis fascia and conjoined tendon attenuation.38 42 43 Verrall et al42 43 hypothesised that hip-joint capsular twisting from Australian Rules Football participation may create motion restrictions similar to those that repetitious throwing creates at the glenohumeral joint. The same mechanisms that create sports hernias may also lead to osteitis pubis, pubic bone oedema or hip adductor tendinosis, supporting the likelihood of coexisting injuries, whether or not a sports hernia exists.38
The pubic symphysis is the centre of rotation between the compression strut that links the posterior pelvis and lumbosacral spine with the femur.42–44 Restricted hip ROM or muscle group strength, endurance, coordination or extensibility imbalances may further increase the stress/unit area in this region. This places excessive loads on the inguinal wall tissue that lies perpendicular to the transversalis fascia, causing pain and/or defects at the inguinal rings.11 42–46 Non-contractile tissue injury from these shearing forces may be particularly problematic for athletes who have developed imbalances between the comparatively stronger hip adductor muscles and the comparatively weaker lower abdominal muscles.11 33 The hip adductor muscles (particularly the adductor longus and gracilis) are important pelvis stabilisers during single leg support. Effective dynamic hip motion control in sports such as soccer, Australian Rules Football or ice hockey requires synergistic abdominal and hip region muscle co-activation to maintain appropriate lumbopelvic alignment.33 Weakness, poor endurance, reduced extensibility or poor coordination of these muscular synergists may precipitate functional instability, overuse and injury at comparatively weaker non-contractile structures.33 Subsequent attenuation or tearing of the transversalis fascia or conjoined tendon,5 47 rectus abdominis insertion,13 15 internal oblique muscle at the pubic tubercle,48 external oblique muscle and aponeurosis,48 nerve entrapment at the external oblique aponeurosis,49 entrapment of the genital branches of the ilioinguinal or genitofemoral nerves,50 or entrapment of the obturator nerve19 have all been reported.
Balduini et al51 suggested that the tenuous nature of the internal and external oblique muscle origins and insertions predisposes them to strain injury. In men, these muscles extend to form the cremaster (internal oblique) and internal and external (internal and external oblique) spermatic fascia, which is the likely reason why lower abdominal injuries may precipitate scrotal pain.38 51 Others have theorised that increasingly rigorous and perhaps misguided off-season conditioning programmes contribute to a imbalance of strength, endurance, coordination and/or extensibility between the stronger leg muscles and the weaker abdominal muscles, increasing shear forces across the pubic symphysis and subsequent tearing of the transversalis fascia, conjoined tendon, inguinal canal or overlying musculature.2 5 6 10 11 16 22 35 38 52 53 58 Hip adductor strains occur 20 times more commonly during professional hockey training camp compared with the regular season, suggesting that off-season deconditioning or inappropriate off-season conditioning practices may both be contributing factors.10 52
Direct trauma, intense abdominal muscle training or the stresses associated with repetitious rotational trunk forces transmitted to the abdominal wall during a hockey slapshot could lead to ilioinguinal nerve entrapment in a similar condition known as “hockey groin syndrome”.34 Hypertrophied internal oblique muscles may increase the shearing forces that are transmitted to the external oblique aponeurosis, leading to fascial tears or thinning.34 Ziprin et al,49 in a study of 25 male athletes (mainly soccer players) identified external oblique aponeurosis defects through which the neurovascular bundles passed. After surgical division of these bundles and primary repair of the aponeurosis tears, chronic groin pain was largely eliminated.
Differential diagnosis
Sports hernias are characterised by insidious onset, gradually worsening, diffuse, unilateral groin pain that may radiate to the perineum and upper medial thigh.11 20 22 35 38 51 53–57 Pain radiation across the midline into the scrotum and testicles is present in approximately 30% of symptomatic individuals.16 17 47 Although the signs and symptoms of chronic groin injury are well described, how they contribute to the differential diagnosis of a sports hernia is less clear.5 11 22 35 A detailed history, focused questioning and clinical examination are the most important aspects of the consultation.48 58–61 The average patient with a sports hernia is a man in his mid-20s, but sports hernias have been diagnosed across a wide age range32 and they are more common in women than previously thought.32 38 62 Between 27% and 90% of athletes with sports hernia-type symptoms have multiple pathologies,5 7 26 34 40 63–66 making accurate diagnosis difficult and supporting the need for a multidisciplinary examination.7 23 62 65 67 68
The underlying aetiology of musculoskeletal chronic groin pain in general is usually attributed to one of four broad categories: (1) adductor longus dysfunction, (2) osteitis pubis, (3) sports hernia (sportsman’s hernia, pre-hernia complex, Gilmore’s groin) or (4) a pathological condition of the hip joint (femoroacetabular impingement, capsulolabral injuries and chondral defects).25 69 70 Holmich et al23 described three musculotendinous causes for chronic groin injury in sportsmen: (1) hip adductor-related dysfunction with palpatory pain at the pubic bone attachment and pain with resisted hip adduction; (2) iliopsoas-related dysfunction with palpatory pain of the muscle at the lower lateral abdomen or immediately distal of the inguinal ligament, in addition to pain during the Thomas test; and (3) rectus abdominis-related dysfunction with palpatory pain at the distal tendon or pubic bone attachment, and pain with a resisted sit-up.23
Acknowledgment of groin pain during the performance of sports-specific movement patterns is considered to be unequivocal for the sports hernia diagnosis.33 Biedert et al33 reported a specific chronic groin pain and “weakness” combination for “symphysis syndrome” consisting of: (1) posterior inguinal wall deficiency with an open external inguinal ring and weak external oblique muscle aponeurosis and transversalis fascia without clinical signs of a hernia, (2) a small rectus abdominus muscle attachment area on the pubis, and (3) chronic hip adductor pain. With symphysis syndrome, pain is generally located lateral to the rectus abdominus muscle sheath, medial to the inguinal ligament and immediately proximal to the pubis, where a smaller than normal rectus abdominus attachment does not adequately cover the weak groin region. They described the pain mechanism as increased intra-abdominal pressure during sports activity that thrusts the peritoneum into the weak groin region.33
Before arriving at a diagnosis of sports hernia, other musculoskeletal aetiologies must be excluded, such as referred synovitis, lumbosacral pain, femoral capital avascular necrosis or slipped epiphysis, femoral neck and shaft stress fracture, degenerative hip disease, rheumatic arthritis, sacroiliac or iliolumbar ligament injury, pelvic joint inflammatory conditions, pubic bone stress reactions, disruption of muscle or tendon and enthesopathy, bursitis (13 in the region) and snapping hip syndrome.62 66 69
Other conditions such as “true” hernias, nerve entrapment or irritation, tumours, regional inflammatory or infection conditions (prostate conditions, urinary infections, gynecological disorders, rheumatoid arthritis, intra-abdominal disorders, genitourinary abnormalities, anklylosis, spondylitis, Legg–Calve–Perthes disease, seronegative arthropathy, Reiter syndrome, gout, osteomyelitis, tuberculosis) must also be excluded, further contributing to the diagnostic dilemma.7 14 31 46 66 71
Importantly, the physical examination of a patient with a sports hernia reveals no detectable inguinal hernia. Unless there are multiple causes, patients can often identify the exact site of pain.12 56 58 72 With a sports hernia the following elements are consistently found on physical examination: (1) inguinal canal tenderness, (2) dilated superficial inguinal ring, (3) pubic tubercle tenderness, and (4) hip adductor origin tenderness.20 The key physical examination finding is pubic tubercle tenderness and an inguinal floor tear that can occasionally be palpated, creating pain inside the external inguinal ring.21 The pain may radiate to a testicle or laterally to the upper thigh.16 17 47 The pain is usually aggravated by sudden movement such as athletic effort, a Valsalva manoeuvre sneezing, coughing or sexual activity, or during a resisted sit-up or hip adduction.11 21 73 Verrall et al74 described three pain provocation tests that if positive indicated a high likelihood for an athlete having MR-detected parasymphyseal pubic bone marrow oedema: (1) having the patient squeeze their knees together while supine with 45° hip flexion and 90° knee flexion, (2) having the patient squeeze their feet together while supine with 30° hip flexion and slight abduction-internal rotation, and (3) hip flexion–abduction–external rotation (FABER) or Quadrant tests. However, Mens et al75 reported that isometric hip adduction is not a hallmark for hip adductor muscle-group injury as pain levels decrease and muscle force levels increase in patients with pelvic ring instability who wear a pelvic belt.
Entrapment of the genital branch of the genitofemoral, ilioinguinal, lateral femoral cutaneous or obturator nerves may also create symptoms that resemble those of a sports hernia.19 76 77 Bradshaw et al50 78 stated that the course of the obturator nerve placed it at increased risk for entrapment between poorly described fascia and the obturator externus and adductor brevis muscles. Adductor magnus and adductor longus receive partial innervation from the sciatic and femoral nerves, explaining why obturator entrapment may create only subtle weakness on physical examination and possibly making the adductor brevis ideal for specific insertional EMG examination of obturator nerve entrapment.7 When sensory nerve compression or entrapment is the cause of groin pain or paraesthesia, the pattern tends to closely follow the sensory distribution of the particular nerve that is entrapped or compressed.19 However, there is considerable anatomical variation in the origin and course of the ilioinguinal, genitofemoral and iliohypogastric nerves.7 For effective treatment of a patient with groin pain of neural origin, it is essential to have a thorough knowledge of regional cutaneous nerve anatomical variability, an appreciation of the pathophysiology of neuroma formation, and a specific surgical approach strategy.79
Hemingway et al64 reported that the hip flexors on the affected side of randomly selected individuals with posterior inguinal wall insufficiency were significantly weaker than those on the non-involved side before surgical repair, possibly due to pain inhibition. Additionally, only 12.5% of patients compared with 100% of non-impaired control subjects could effectively perform a transverse abdominal muscle test to control pelvic tilt during crook lying and only 13% of patients compared with 80% of control subjects could effectively perform an external oblique muscle test to control hip abduction and external rotation while simultaneously controlling pelvic tilt.64 Tests such as these may be useful as screens to identify individuals who are at risk for sports hernia development or who may have a symptomatic sports hernia.
Diagnostic imaging does not generally reveal a sports hernia, but it is useful to exclude other conditions.35 Standard radiographs may reveal pubic symphysis widening or erosion, fractures, healing stress fractures or skeletal disease.21 The “flamingo x ray view” with the patient in an alternating one-leg stance may ascertain pelvic movement shifts across the pubic symphysis.21 Bone and/or CT scans can effectively exclude stress reactions or inflammatory processes. MRI is useful in detecting the location, extent and characteristics of pelvic and/or hip injury such as strains, labral tears, stress reactions, osteitic pubis, iliopsoas bursitis, true hernias or occult stress fractures, and is somewhat useful to predict recovery time and in defining treatment,7 16 60 69 80–82 but it may not be a useful tool for deciding between operative or conservative chronic groin injury treatment.83
The secondary cleft sign on MRI may imply adductor longus, gracilis or conjoined tendon dysfunction.84 This sign should be sought on coronal short inversion time inversion–recovery (STIR) images in athletes who present with chronic groin pain. The presence of the secondary cleft sign on MRI may obviate an extensive search for other chronic groin pain causes, thereby reducing the number of unnecessary diagnostic imaging interventions.84
If the patient has a painful hip Quadrant or FABER test,74 MR arthrography should be considered. If the MR arthrography is positive, hip arthroscopy evaluation should be considered.70 Patients with pre-existing femoroacetabular dysplasia are more susceptible to capsulolabral tears secondary to altered hip joint biomechanics.8 Patients with labral tears often give a history of a sharp, catching pain that is poorly localised, radiating to the groin where it may be the only area of reported symptoms.8 Narvani et al85 reported that MR arthrography showed an acetabular labrum tear in 4 of 18 (22.2%) consecutive athletes who presented with chronic groin pain.
Diagnostic imaging to identify sports hernias has not been particularly useful, with the exception of ultrasonography, which enables a dynamic assessment.7 60 69 As the patient actively strains during the procedure, a real-time convex anterior bulge and ballooning of the inguinal canal can be observed at the superficial inguinal ring.11 86 Posterior inguinal wall deficiency is visible when anterior abdominal wall muscle contraction reveals a loss of the normal valve-like action on the inguinal canal as the posterior inguinal wall is displaced anteriorly rather than becoming taut.8 However, these features are very subtle, and this test is highly operator-dependent.8 86 87 Although this finding is also associated with varicocoeles, spermatic cord lipomas and increasing patient age, the presence of a progressive convex anterior bulge increases the diagnostic specificity for a sports hernia.86 Future advancements in the use of ultrasonography imaging during rehabilitation exercises and physical task performance may enable more accurate, functionally relevant assessment and evaluation of soft tissue inguinal region injuries and treatment effectiveness.88
Herniography (injecting a contrast material into the abdominal or peritoneal cavity) provides an anatomical outline of the pelvic floor and its peritoneal reflections, and can identify small inguinal canal tears,60 69 73 89 90–92 but it is an invasive procedure that lacks specificity and has a high false-positive rate.20 21 35 59 65 81 87 91 Potential risks from herniography include hollow viscous perforation, vasovagal reactions, infections, abdominal wall hematomae and contrast agent reactions. Herniography for the differential diagnosis of a sports hernia is rarely used in the USA.11
In summary, sports hernia is a diagnosis made by a comprehensive physical examination that requires excluding numerous other musculoskeletal and non-musculoskeletal conditions. The typical duration of symptoms before diagnosis can range from 6 weeks to 5 years, with an average of 20 months.47 68 92 Essentially it is a diagnosis that can only be confirmed at surgery.11 The chronic groin-region pain and tenderness that athletes who have a sports hernia display is more directly related to their inability to effectively compete in sports activity than are imaging findings.39
Conservative treatment
Traditional conservative sports hernia treatment has low success rates.16 63 66 Conservative treatment generally includes 6–8 weeks of rest followed by focused progressive resistance hip adductor strengthening and stretching exercises, sports-specific functional tasks, and gradual return to full activities.40 63 66 92 At approximately 10–12 weeks after the start of conservative treatment and when the athlete is pain-free, return to sports competition is generally attempted.33
Like most other chronic groin injuries, sports hernias are also initially treated with non-steroidal anti-inflammatory medication, heat or ice, and massage.5 66 Electrical techniques such as transcutaneous electrical nerve stimulation or interferential current may be used for pain control at any time during the treatment progression. An active programme designed to improve strength, endurance, coordination and appropriate hip and abdominal muscle synergistic balance (including isometric and progressive resistance hip abduction, adduction, flexion, extension exercises, sit-ups, wobble board, sliding board and Pro-Fitter (http://www.fitter1.com) exercises) has been shown to achieve better patient outcomes than a conventional, more passive treatment intervention.6 Only recently have conservative rehabilitation programmes been developed that address the power, endurance and coordination of trunk and hip stabilising muscles.5 64 93–95 The rehabilitation emphasis should be on placed on resolving core strength, endurance, coordination and extensibility deficiencies and imbalances at the hip and abdominal muscles and on dynamically stabilising the pelvic ring.5 11 35 75 93–95
Tyler et al93 reported that pre-season hip adductor strength was 95% of hip abductor strength for uninjured hockey players, but only 78% of hip abductor strength for injured players. Development of a hip adductor injury-prevention plan including stationary cycling, hip adductor stretching, sumo squats, side lunges, kneeling pelvic tilts, ball squeezes, concentric progressive resistance hip adduction exercises, sliding board, unilateral lunges with reciprocal arm movements, “on ice” kneeling adductor “pull togethers”, slide skating, and cable column crossover pulls significantly decreased hip adductor injuries among this group of athletes.94 95
Ashby72 identified entheseopathy at the pubic insertion of the rectus abdominis or adductor longus tendons of 49 patients with chronic groin pain and reported pain relief at 3–15 months after local injection of a long-acting steroid (1% triamcinolone) and local anaesthetic (2% lignocaine). Proliferative injection therapy (prolotherapy) with 12.5% dextrose solution injected into the hip adductor pelvic attachments at the conjoined tendon on the pelvic rim and at the symphysis pubis may facilitate the natural repair process.67 A single entheseal injection of bupivacaine (3 mL of a 0.5% solution) mixed with triamcinolone actetonide (80 mg in 2 mL) provided hip adductor-related groin pain relief for at least 1 year in competitive rugby and soccer athletes.25 In summary, conservative treatment as it applies specifically to a diagnosis of sports hernia is poorly described, and evidence of successful conservative treatment intervention is lacking.6 11 20 22
Surgery
The literature suggests that, unlike most other causes of groin pain, sports hernias rarely improve without surgery.11 35 38 96–98 Surgical exploration and repair should only be considered when rest and non-surgical treatment over a minimum of 6–8 weeks has failed, and when careful elicitation of history and a multi-disciplinary clinical examination has excluded other potential pain sources.21 55 65
When the surgical option is selected, either an open or a laparoscopic approach can provide good results.38 Most sports hernia surgical procedures reinforce the abdominal muscles or fascia near the inguinal ligament in a manner similar to conventional hernia surgery.2 18 28 Meyers et al,13 in reporting successful open procedures on numerous athletes suggested that laparoscopic or “incorrect” open repairs, which did not effectively address the causative pathology, were both unlikely to have a successful outcome. Many reports of sports hernia surgical techniques do not provide sufficient detail, and several “anatomical” repairs do not incorporate the appropriate anatomical layers.20 A wide variety of open-repair techniques are described to reinforce the inguinal canal by reinforcing the existing tissue layers with 21 30 34 58 87 96 98 or without 2 4 13–15 28 33 37 49 55 97 mesh. There is a growing number of surgeons using laparoscopic techniques to repair sports hernias.3 29 31 36 54 58 96 99 100 Regardless of whether the surgical intervention is laparoscopic or open, success rates reportedly vary from 63–97% for both symptom relief and for return to previous sports activity levels.4 11 13 35 47 96 97 Meyers et al12 reported that a success rate of 95% should be expected with carefully selected patients. Our review reveals very good and comparable results between open (mean 92.8 (SD9.9)%) (table 1) and laparoscopic (96.0 (SD 4.5)%) (table 2) repairs based solely on the criterion of return to sports activity. Two reports were not included in these estimates, as both open and laparoscopic techniques were used.58 96 Some have suggested that at least part of the success with either surgical approach for the treatment of sports hernisas can be attributed to the inflammatory reaction and general tissue healing fibrosis that occurs at the repair site.12 13 44 Additionally, surgery seems to be quite effective regardless of whether the technique that is used is open or laparoscopic, when return to sports activity is used as the sole criteria for evaluating patient outcome. However, basing surgical success on return to sports activity alone is insufficient to truly determine the efficacy of treatment intervention.9 39 As with other areas of surgery, improved, more frequent and patient-directed outcome measurements are needed.
Most patients do well with sports hernia repair in the absence of definitive MRI or diagnostic ultrasonography findings.12 83 87 Additionally, surgical release of a portion of the hip adductor muscle group from the pubic bone may help restore the balance between abdominal and hip adductor muscle forces at the pubic bone.13 33 54 55
Several reports suggest that ideally, the injured tissue should first be normalised with an anatomical surgical repair and then be reinforced with mesh.1–3 21 29 30 58 96 98–100 Our review found that on average, 35% of open and 100% of laparoscopic procedures used mesh. Concerns exist that laparoscopic repair may not completely repair the lesion as it does not enable direct visualisation, potentially contributing to greater failure over time.12 13 38 60 On the other hand, a laparoscopic approach may provide better posterior inguinal canal wall exposure, enabling easier bilateral reinforcement of the lower abdominal wall from the pubic bone to the anterior superior iliac spine.31 The relatively “tension-free” laparoscopic technique described by Genitsaris et al31 may enable earlier return to strenuous exercise performance, in contrast to an open repair in which a new inguinal floor is constructed by suturing mobile muscles and non-contractile (aponeurotic elements) structures together under tension.31 However, Meyer et al12 suggested that the tension-free repair provided by the laparoscopic repair does not adequately stabilise the anterior pelvis. Neumayer et al101 reported that laparoscopic repair yielded a significantly higher recurrence rate (10.1%) after direct inguinal hernia repair compared with an open-repair technique with mesh reinforcement (4.9%) concluding that the open mesh repair was superior. Conceivably, an open technique with sufficient anatomical sports hernia repair and mesh reinforcement might provide the most durable repair, but it is difficult directly extrapolate the findings of Neumayer et al101 to the strictly sports hernia condition. Canonico et al102 reported good preliminary results for using human fibrin glue to secure mesh to achieve tension-free open inguinal hernia repair in soccer athletes with chronic groin pain.
Laparoscopic repair may enable athletes to progress more quickly during rehabilitation and ultimately to return to unrestricted sports activities faster than open repair.38 53 Srinivasan & Shuricht et al,103 reported that approximately 87% (13 of 15 patients) of sports hernia cases treated with laparoscopic repair could return to training within 4 weeks of surgery and to full activity within 6 weeks, and did not have recurrent symptoms at a mean follow-up if 12.1 months (range 6 to 60). In a similar report, Ingoldby et al96 reported that 13 of 14 (92.9%) athletes who underwent laparoscopic surgery for sports hernia repair returned to training within 4 weeks.
In using open repair to treat a group of 12 recreational athletes with sports hernias Ahumada et al104 reported that 83.3% (10 of 12 patients) had excellent results at follow-up at 4 months, but open repair required athletes to be relatively inactive over the initial four postoperative weeks. Only after these 4 weeks were athletes allowed to begin even mild activities such as walking in a swimming pool and gentle stretching. Athletes who underwent open repair were generally returned to full activity at 6 months postsurgery.104 Kumar et al30 reported that open inguinal wall repair was associated with a marked improvement in patient median pain scores, and approximately 93% (25 of 27 patients) had returned to full activity by 14 weeks. Malycha and Lovell4 reported an approximately 93% (41 of 44 survey respondents) return to pre-injury sports activity level at 6 months follow-up among sports hernia cases that were treated with open repair.
Therefore, it seems that both laparoscopic and open repair techniques for sports hernias can be effective, but laparoscopic repair offers the advantage of a faster rehabilitation progression, earlier return to unrestricted activities of daily living and earlier return to pre-injury sports activity levels. Part of the difficulty in assessing the superiority of a particular surgical approach is the heterogeneity of the patient populations.20 22 Well-designed prospective, randomised, controlled studies are greatly needed to establish the true efficacy of these different surgical approaches.11 20 66
Post-surgical rehabilitation
Post-surgical rehabilitation has been described to varying extents by several reports,2 4 30 33 34 37 47 49 54 55 63 64 104 but detailed descriptions are generally lacking. Early, sharp, sudden movements after surgery are avoided, and core and leg musculoskeletal inflexibility, weakness, poor endurance or poor coordination are identified and corrected. Walking is encouraged early in the postoperative period, with progression to jogging or running by 3–4 weeks.4 47 63 Straight-line running while avoiding cutting movements and select sport-specific activities may be started after postoperative day 21.63 Sprinting without cutting can generally be started by the third postoperative week and runners subsequently return to full activity within 2–4 months.35 Recovery after laparoscopic repair generally takes 6–8 weeks before full return to competition is permitted.30 47 54 64 104
Hemingway et al64 described a 6-week post-open sports hernia repair rehabilitation programme. Week 1: isometric abdominal and hip exercises, walking increased by 5 min/day and stair climbing; week 2: active hip exercises, active transverse and oblique abdominal exercises and stationary cycling; week 3: flexibility work, resistance-band hip exercises, active transverse and oblique abdominal exercises, jogging and swimming; week 4: forward running, abdominal training with progressive resistance, upper body exercise with light resistance; week 5: sprinting, multi-directional running, light ball skills, kicking, progressive resistance abdominal exercises and gradual return to sports; and week 6: unrestricted exercise training and return to competitive sports.
van Veen et al54 also described a 6-week post-laparoscopic sports hernia repair rehabilitation programme. Weeks 0–1: walking 5 km/h; weeks 1–2: aquatic training, 20 minutes power walking (adding 5 minutes each session to a 50-minute maximum), 4 sets of 10 minutes stationary cycling at 80–90 rpm, 2 minutes break between sets to a maximum of 15 minutes, isometric rectus abdominis training and step-ups with knee flexed at 60°; weeks 2–3: sit-ups, progressive interval and speed running and lunges; weeks 3–5: weight training, normal activities within pain-free limits; and week 6: normal, unrestricted training.
Overall we found that post-surgical recovery time (based on return to sports activity) for patients who underwent open repair was 17.7 (13.1) weeks, compared with 6.1 (4.5) weeks for laparoscopic repairs. Developing evidence-based post-surgical rehabilitation and conditioning progressions and more standardised patient outcome and activity level assessments (with patient-generated items and item weighting) are needed. Serial measurements should be made at key functional time points and milestones based on specific criteria such as pain, strength and function levels. This needs to take place in addition to the extremely limited and often misinterpreted “return to play” factor and widely varying follow-up periods. Well-designed studies are greatly needed.9 11 20 66 68
What is already known about the topic?
The differential diagnosis of a sports hernia is difficult to make from physical examination and it is thereby largely determined only at the time of surgery.
Both open and laparoscopic surgical approaches have been reported to effectively eliminate symptoms and enable patients to return to previous sporting activity levels.
What this study adds
Sports hernia anatomy, surgical procedures and rehabilitation strategies are poorly described.
Intervention success should be based on serial patient outcome measurements rather than relying exclusively on return to sports activity timing.
Well-designed research studies will help to better elucidate pathogenesis, verify intervention efficacy, develop evidence-based prevention strategies and more effectively direct conservative and post-surgical rehabilitation.
CONCLUSION
Sports hernias most often occur in males who participate in sports that involve cutting, pivoting, kicking and sharp turns and although their onset is usually insidious, with focused questioning a specific incident or “onset mechanism” may be recalled.13 58 We currently do not know the precise sequence of events that lead to sports hernia development, but the combination of abdominal and hip adductor muscle strength, endurance and coordination imbalances, lumbopelvic and hip ROM deficits, poor tissue extensibility and intense or high-repetition hip adductor muscle shearing forces through their pelvic attachments may be the primary factors.5 7 11 13 23 26 33 42–44 Poorly designed off-season conditioning programmes that focus on leg muscle strength–power development while neglecting synergistic abdominal and core muscle group strength, endurance, coordination and extensibility balance may be related to the increasing number of sports hernias that are being reported. Although numerous injuries may contribute to the sports hernia diagnosis, the most common surgical finding is posterior inguinal wall insufficiency that creates an occult hernia that is not apparent on physical examination.16
As it can be difficult to make a definitive diagnosis based on conventional physical examination, diagnostic imaging techniques such as MRI, use of CT scans and diagnostic ultrasonography is recommended. To date the most effective use of various imaging techniques has been to exclude other groin-region injuries. Innovative rehabilitative ultrasonography imaging methods may have considerable potential for directing conservative and post-surgical sports hernia treatment.66 86 88
The literature suggests that sports hernia surgery is considerably more effective than conservative treatment.11 35 98 Unfortunately, information regarding specific conservative treatment interventions, particularly as they apply to strength, endurance and coordination training and flexibility exercises, manual treatment and electrotherapy are poorly described, and well-designed studies are lacking. When the decision is made to proceed with surgery, laparoscopic repair, in addition to providing a minimally invasive exploratory diagnostic method, also enables a faster rehabilitation progression and potentially a quicker return to unrestricted sporting activities than open repair. However concerns exist regarding the capacity for this surgical method to completely evaluate and repair all sports hernia lesion types.60
In summary, sports hernias remain a misunderstood and poorly researched problem that affects many athletes at all levels of competition. There is currently no consensus as to what specifically constitutes its diagnosis. Well-designed research studies are needed to better understand the pathogenesis of sports hernia, to aid in its prevention and to more effectively direct conservative treatment. The high incidence of groin/abdominal strain injury early in the competitive season for sports such as soccer and ice hockey has significant implications for further investigation of risk factors such as non-existent or poorly designed off-season sports training programmes.
REFERENCES
Footnotes
Competing interests: None.