Article Text

Abstract
To examine the effects of regular participation in recreational soccer on health profile, 36 healthy untrained Danish men aged 20–43 years were randomised into a soccer group (SO; n = 13), a running group (RU; n = 12) and a control group (CO; n = 11). Training was performed for 1 h two or three times per week for 12 weeks; at an average heart rate of 82% (SEM 2%) and 82% (1%) of HRmax for SO and RU, respectively. During the 12 week period, maximal oxygen uptake increased (p<0.05) by 13% (3%) and 8% (3%) in SO and RU, respectively. In SO, systolic and diastolic blood pressure were reduced (p<0.05) from 130 (2) to 122 (2) mm Hg and from 77 (2) to 72 (2) mm Hg, respectively, after 12 weeks, with similar decreases observed for RU. After the 12 weeks of training, fat mass was 3.0% (2.7 (0.6) kg) and 1.8% (1.8 (0.4) kg) lower (p<0.05) for SO and RU, respectively. Only SO had an increase in lean body mass (1.7 (0.4) kg, p<0.05), an increase in lower extremity bone mass (41 (8) g, p<0.05), a decrease in LDL-cholesterol (2.7 (0.2) to 2.3 (0.2) mmol/l; p<0.05) and an increase (p<0.05) in fat oxidation during running at 9.5 km/h. The number of capillaries per muscle fibre was 23% (4%) and 16% (7%) higher (p<0.05) in SO and RU, respectively, after 12 weeks. No changes in any of the measured variables were observed for CO. In conclusion, participation in regular recreational soccer training, organised as small-sided drills, has significant beneficial effects on health profile and physical capacity for untrained men, and in some aspects it is superior to frequent moderate-intensity running.
Statistics from Altmetric.com
It is well established that endurance training, such as jogging and bicycling, improves the physical capacity of inactive subjects and promotes health. Thus, epidemiological studies indicate that greater physical activity or fitness is associated with a lower blood pressure (BP), and meta-analyses of randomised controlled trials show that dynamic aerobic endurance training is able to reduce BP.1 2 3 4 With regard to the characteristics of the training programme, these meta-analyses conclude that there were only minimal or no effects of exercise frequency, type, duration and intensity of training on the BP response.1 2 3 4 5 Reduced total peripheral resistance has been suggested to contribute to the antihypertensive effects of exercise. However, although muscles represent a significant part of the total body mass, few studies seem to have looked for a possible relationship between changes in blood pressure and alterations in muscle vascular structure.
A significant number of studies have demonstrated a loss of fat mass after a period of regular physical activity and exercise training seems to produce favourable changes in plasma lipids and lipoproteins. Plasma triglyceride concentrations are usually but not always lowered, and this decrease is related to baseline concentrations.6 7 8 Some studies also find lowered cholesterol levels after an exercise training programme but it appears to require a reduction in body weight, body fat, or dietary fat intake during the training period.9 10 HDL-cholesterol (HDL-C) is generally responsive to aerobic training and increases in a dose-dependent manner with increased energy expenditure if the exercise training lasts longer than 12 weeks, but this is not always the case.11 12 Several other factors, such as the exercise training volume, body weight and composition changes, do also appear to play a role.9 11 13 14 LDL-cholesterol (LDL-C) is a powerful coronary artery disease (CAD) risk predictor, but is usually not lower after aerobic exercise training.7 15 16 17 18 However, LDL-C has been observed to decrease,19 and the effect on LDL-C appears to be related to the distance run per week and the reduction in body fat.20
Most studies looking at the effect of physical activities on health have used exercise such as walking, jogging, running and cycling with a rather constant training intensity in the range of 30 to 90% of maximal oxygen uptake (VO2max). No studies appear to have looked at the effect on the health profile of regular training with frequent and marked changes in exercise intensity, as occurs in soccer. Although more than 500 million people worldwide are believed to play soccer, little is known about the beneficial effects on health profile of participation in regular soccer activities. Recent studies reveal that the heart rate response in small-sided games, such as 3v3, 4v4, 5v5 and 7v7 in recreational soccer, is roughly similar to that in elite soccer training with periods of near-maximal values.21 22 23 24 It has furthermore been shown that the activity profile during small-sided games is highly intermittent, with multiple turns, jumps and sprints which provide a high impact on muscles and bones.23 24 25 26 On that basis, it would be of great interest to know how soccer training on a regular basis affects cardiovascular and musculoskeletal factors related to health. Soccer training is highly motivating and appeals to a significant part of the population and therefore has the potential to be implemented as a permanent health-promoting activity.
Thus the aim of the present study was to examine the effect of regular participation in recreational soccer on health profile in relation to cardiovascular and musculoskeletal adaptations. The response was compared with the adaptations occurring after a similar period and duration of moderate-intensity running in order to evaluate whether an intermittent sport activity is as efficient as running in promoting health.
Methods
Subjects
Thirty-six healthy untrained men aged 20–43 years with a body mass, body mass index, fat percentage and maximal oxygen uptake (VO2max) of 84.4 (SEM 2.4) kg, 25.6 (0.6), 24.5% (1.1%) and 39.4 (0.9) ml/min/kg, respectively, took part in the study. The participants were non-smokers, did not take medication and had not been involved in any type of physical training for at least 2 years. The study was approved by the local ethical committee of Copenhagen (14606; H-C-2007-0012).
Design
The subjects were matched and randomly assigned to a soccer group (SO; n = 13), a running group (RU; n = 12) or a control group performing no physical training (CO; n = 11). Four subjects dropped out due to injuries occurring during training or testing: one soccer player (ankle sprain), two runners (tibial periostitis and achilles tendinopathy) and one control subject (hamstring strain). For the participants who completed the study no group differences were present in preintervention values for age, body mass, fat percentage or VO2max. The participants in SO and RU carried out a 12 week soccer and running training programme, respectively, whereas the participants in CO continued their daily life activities during the period.
Training intervention
Outdoor training was performed two or three times per week for 12 weeks. Each training session lasted 1 h. The soccer sessions consisted of ordinary five-a-side, six-a-side or seven-a-side matches on a 40×60 m natural grass pitch and the running sessions consisted of continuous moderate-intensity running at the same average intensity as the soccer group (82% of individual maximal heart rate). Each training session was initiated by a 5 min low-intensity warm-up period. As the running group had problems coping with 1 h of continuous running, both groups had their training sessions split into three or four segments over the first 6 weeks. The total number of training sessions was 27.6 (2.3 per week) and 30.2 (2.5 per week) for the participants in SO and RU, respectively.
Measuring and test procedures
Subjects were familiarised to all test procedures on one to three occasions. Fasting blood lipoproteins, resting heart rate and blood pressure were determined from 8 to 10 a.m. under standardised conditions after an overnight fast. Blood pressure was measured at least six times by an automatic upper arm blood pressure monitor (HEM-709; OMRON, Illinois, US), and an average value was calculated. Whole body and regional fat, muscle and bone mass were determined by DXA scans (LUNAR, GE Medical Systems, US). Muscle biopsies were obtained from m. vastus lateralis under local anaesthesia using the Bergstrom technique. Pulmonary gas exchange (CPX MedGraphics, US), heart rate (Polar Team System, Polar Electro Oy, Kempele, Finland) and arm vein blood sampling were performed during a standardised treadmill test with submaximal running at 9.5 km/h for 6 min followed by a 15 min rest period and an incremental test to exhaustion.25 Respiratory exchange ratio (RER) was calculated over the last 3 min of running at 9.5 km/h. VO2max and maximal heart rate were determined as the peak value reached in a 30 and 15 s period, respectively, during the last part of the incremental test. Heart rate was determined during all training sessions. Perceived exertion was recorded immediately after training sessions in weeks 4 and 6 by visual analogue scale questionnaires (VAS).26 DXA scans were made prior to and 2 days after the 12 week training period. All other tests were performed after 0, 4 and 12 weeks.
Muscle analyses
Approximately 30 mg wet weight muscle tissue was mounted in an embedding medium (OCT Tissue-Tek, Sakura Finetek, Zoeterwoude, The Netherlands), frozen in precooled isopentane and analysed histochemically for capillaries.27
Blood analyses
Blood samples were obtained in 2 ml syringes with and without heparin. Within 10 s of sampling, 100 μl of heparinised blood was haemolysed in an ice-cold 100 μl Triton X-100 buffer solution and stored on ice until analysed for lactate (YSI 2300, Yellow Spring Instruments, OH, US). Plasma was collected from centrifuged non-heparinised samples, after which LDL, HDL and total cholesterol were determined fluorometrically on an automatic analyser (Cobas Fara, Roche, France) using enzymatic kits (Roche Diagnostics, Germany).
Statistics
Within-group data for 0, 4 and 12 weeks were evaluated by one-way analysis of variance on repeated measurement (RM ANOVA). When a significant interaction was detected data were subsequently analysed using a Newman–Keuls post-hoc test. Between-group changes over 12 weeks were evaluated by one-way analysis of variance (ANOVA). VAS scale scores were evaluated by a Wilcoxon Signed Rank test. A significance level of 0.05 was chosen. Data are presented as means (standard error of the mean (SEM)).
Results
Physiological response to training
The average heart rate during the training sessions was similar for SO and RU (82% (2%) and 82% (1%) of HRmax, respectively). However, during training, the time above 90% of HRmax was higher (p<0.05) for SO than for RU (20% (4%) vs 1% (1%); fig 1). The perceived exertion during training was lower (p<0.05) for SO than for RU (3.9 (0.4) vs 6.0 (0.5)) using a 0–10 VAS scale.
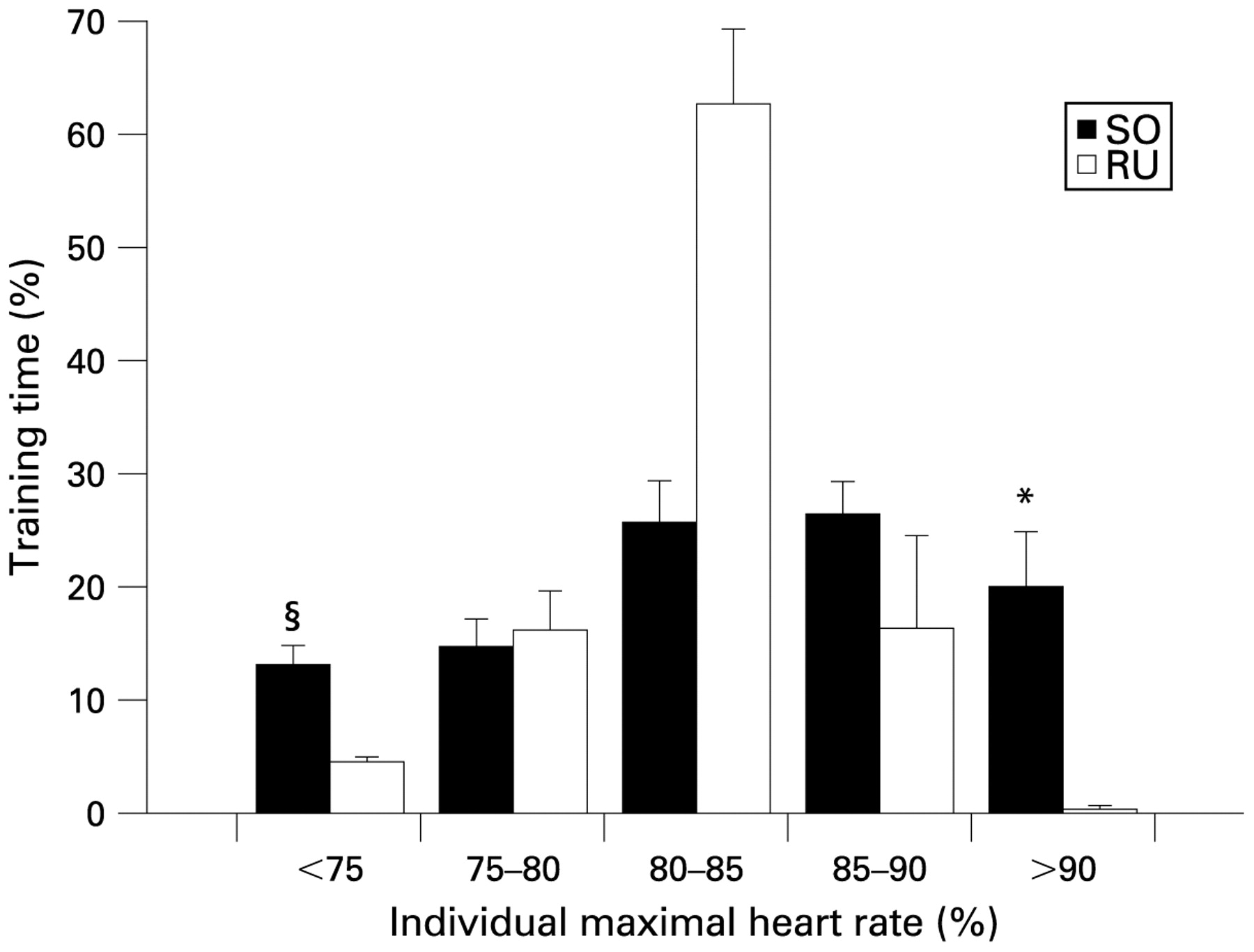
Heart rate distribution, expressed in percentage of total training time in selected heart rate zones, during 25–32 training sessions for untrained men in the soccer group (SO, n = 12) and the running group (RU, n = 10). Means (SEM) are presented. *Significant difference from RU.
Physiological response during treadmill running
Over the 12 week period, VO2max was elevated (p<0.05) by 13% (3%) and 8% (3%) for SO and RU (fig 2), respectively, with no change for CO (fig 2). In SO, VO2max increased (p<0.05) by 7% (3%) over the first 4 weeks and further (p<0.05) by 6% (2%) from 4 to 12 weeks, whereas VO2max was elevated (p<0.05) by 6% (2%) in RU over the first 4 weeks with no further increase from 4 to 12 weeks (table 1). After 12 weeks peak ventilation was higher (p<0.05) in SO and RU, but not in CO (table 1). In SO, respiratory exchange ratio (RER) during running at 9.5 km/h was lower (p<0.05) after both 4 and 12 weeks of training, whereas no significant changes were observed for RU or CO over 12 weeks (table 1). Changes over 12 weeks in VO2max and peak ventilation as well as blood lactate and RER at 9.5 km/h were greater (p<0.05) in SO than in CO, but not significantly different between SO and RU. Changes in VO2max and peak ventilation over 12 weeks were greater (p<0.05) for RU than in CO, whereas the 12 week change in RER at 9.5 km/h was not (p>0.05).

Maximal pulmonary oxygen uptake before and after 12 weeks of soccer practice (SO, n = 12) and running (RU, n = 10) for untrained men, or continuation of an inactive lifestyle (CO, n = 10). Mean and individual values are presented for 0 and 12 weeks. *Significant difference from 0 weeks.
Blood pressure, heart rate, blood lipoproteins, muscle capillaries and exercise response before and after 4 and 12 weeks of soccer practice (SO, n = 12) and running (RU, n = 10, except LDL cholesterol, n = 9) for untrained men, or continuation of an inactive life-style (CO, n = 10; except capillaries, n = 8)
Resting heart rate and blood pressure
After the 12 week training period resting heart rate was lowered (p<0.05) by 6 (1) beats/min for SO (55 (1) vs 61 (2) beats/min) and by 6 (2) beats/min for RU (53 (2) vs 59 (2) beats/min), but was not altered in CO (table 1). In SO, systolic and diastolic blood pressure were lowered (p<0.05) by 8 (3) and 5 (2) mm Hg, respectively, after 12 weeks, with the corresponding values for RU being 7 (3) and 5 (2) mm Hg, respectively (fig 3). No significant changes were observed for CO in systolic or diastolic blood pressure (fig 3). Changes in resting heart rate, systolic blood pressure and diastolic blood pressure over 12 weeks were greater (p<0.05) in SO than in CO, but not significantly different between SO and RU. Changes over 12 weeks in systolic blood pressure were not significantly different between RU and CO, whereas changes in resting heart rate and diastolic blood pressure were greater (p<0.05) for RU than in CO.
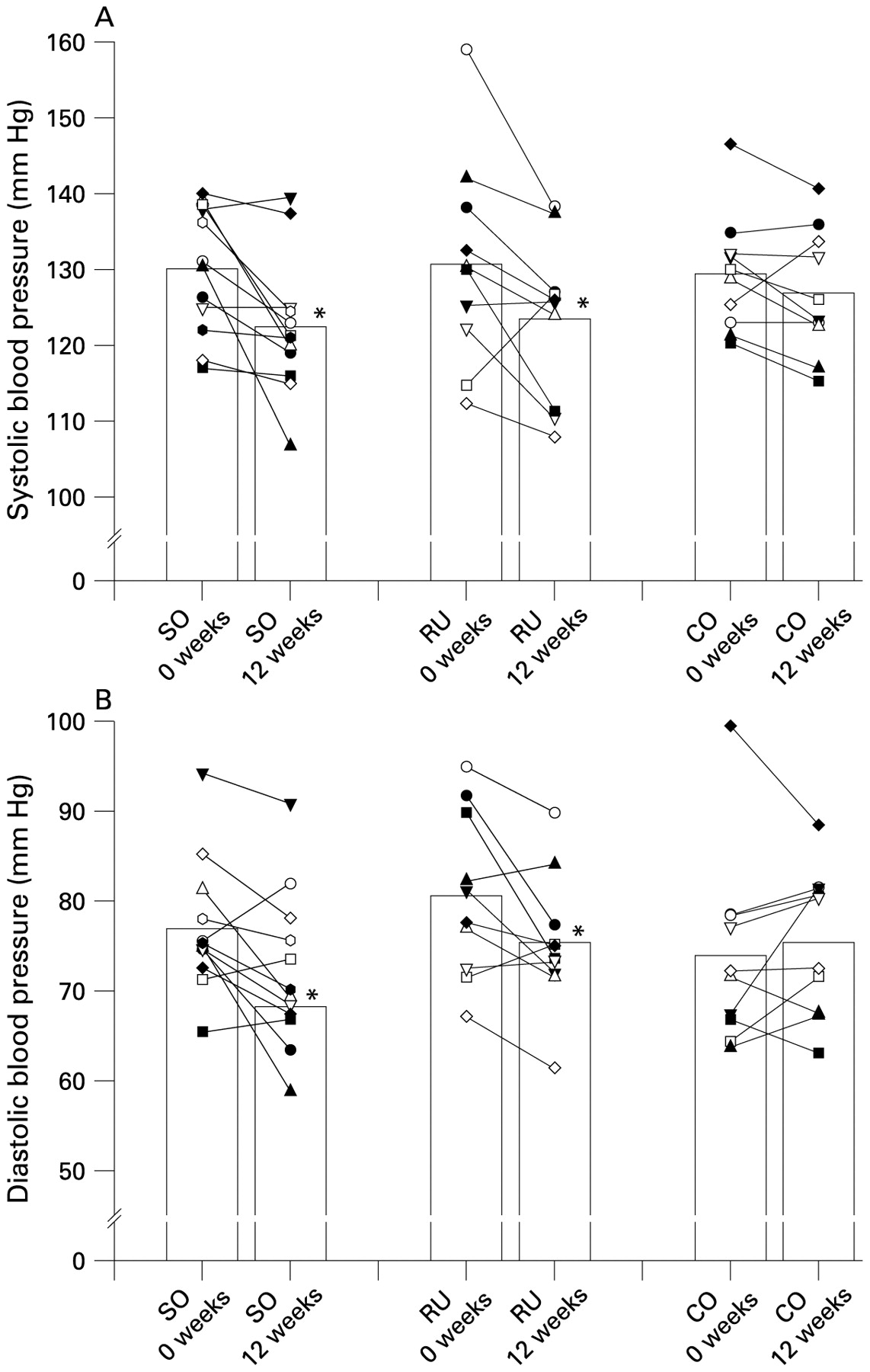
Systolic (A) and diastolic blood pressure (B) before and after 12 weeks of soccer practice (SO, n = 12) and running (RU, n = 10) for untrained men, or continuation of an inactive lifestyle (CO, n = 10). Mean and individual values are presented for 0 and 12 weeks. *Significant difference from 0 weeks.
Body composition
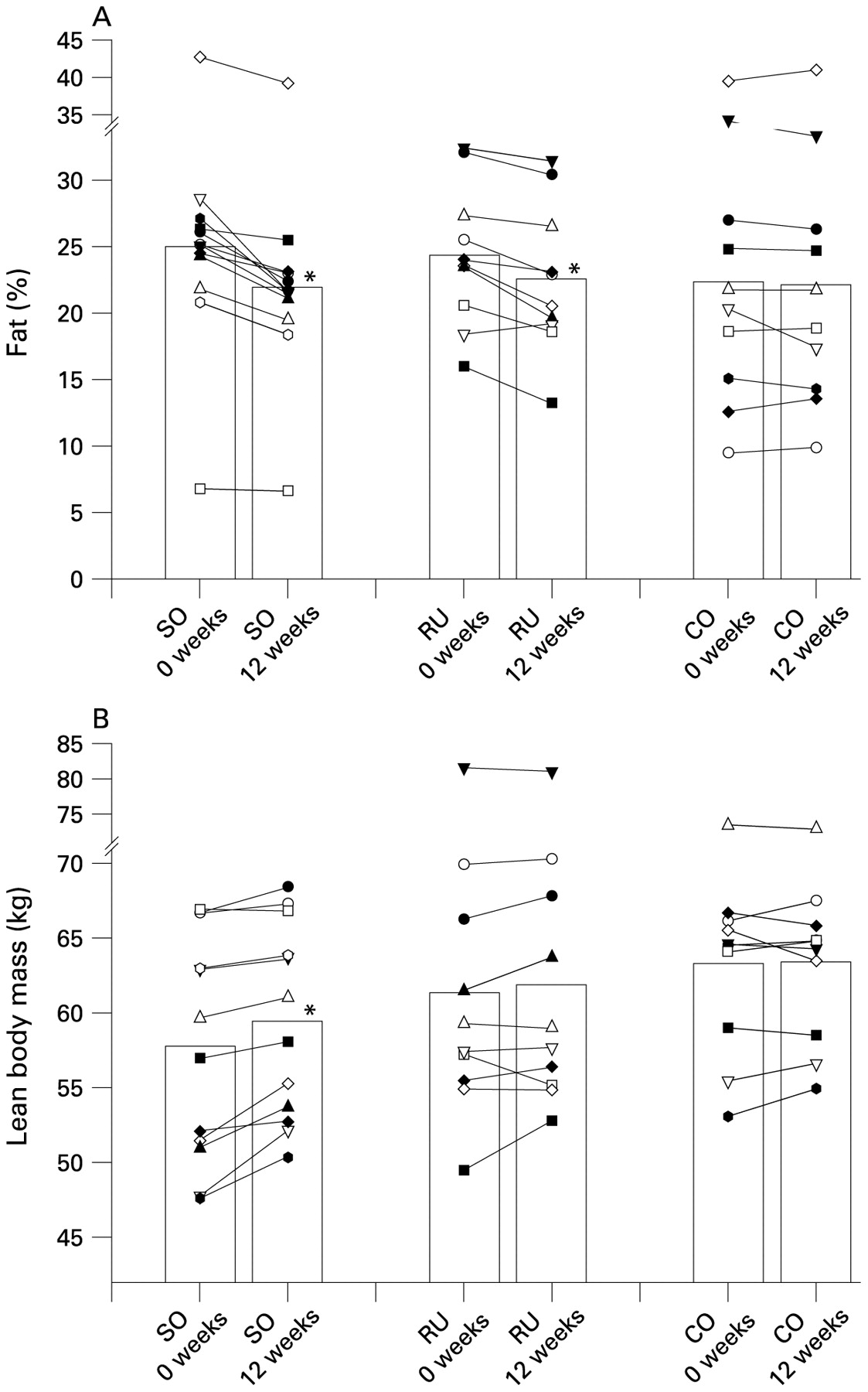
Total body mass was lowered (p<0.05) by 1.1 (0.2) and 1.0 (0.3) kg, respectively, for SO and RU over 12 weeks, whereas no change occurred for CO (table 2). Fat mass and fat percentage for SO were 19.9 (2.4) kg and 24.9% (2.3%) prior to the training period and were lowered (p<0.05) by 2.7 (0.6) kg or 3.0% (0.6%) after 12 weeks (fig 4a; table 2). Seven of the participants in SO had a fat percentage >25% before the training period, with only two after the training period (fig 4a). For those subjects the average decrease in fat mass and fat percentage was 3.6 (0.8) kg and 3.8% (0.8%), respectively. Fat mass and fat percentage were also lowered (p<0.05) in RU over the 12 weeks (1.8 (0.4) kg or 1.8% (0.4%)), whereas no changes occurred for CO (table 2). In SO lean body mass was 57.7 (2.2) kg prior to the training period and 1.7 (0.4) kg higher (p<0.05) after the 12 weeks, whereas no significant changes occurred for RU and CO (fig 4b). Bone mineral density was not significantly altered for any of the three groups (table 2). In SO, lower extremity bone mass was elevated (p<0.05) by 41 (8) g after 12 weeks, whereas no change was observed for RU and CO (table 2). Changes in lean body mass and lower extremity bone mass over 12 weeks were greater (p<0.05) in SO than in RU and CO, with no significant difference between RU and CO. Changes in fat percentage over 12 weeks were greater (p<0.05) in SO than in CO, but not significantly different between SO and RU (p = 0.09) or between RU and CO.

Fat percentage (A) and lean body mass (B) before and after 12 weeks of soccer practice (SO, n = 12) and running (RU, n = 10) for untrained men, or continuation of an inactive lifestyle (CO, n = 10). Mean and individual values are presented for 0 and 12 weeks. *Significant difference from 0 weeks.
Body composition before and after 12 weeks of soccer practice (SO, n = 12) and running (RU, n = 10) for untrained men, or continuation of an inactive lifestyle (CO, n = 10)
Blood lipoproteins
After 12 weeks of training, fasting serum LDL cholesterol was lowered (p<0.05) in SO (2.3 (0.2) vs 2.7 (0.2) mmol/l), but unaltered in RU (2.4 (0.3) vs 2.5 (0.2) mmol/l) and CO (2.7 (0.2) vs 2.7 (0.2) mmol/l) (fig 5). Serum HDL cholesterol was not significantly altered in any of the three groups (table 1). Changes in HDL and LDL cholesterol over 12 weeks were not significantly different between groups.
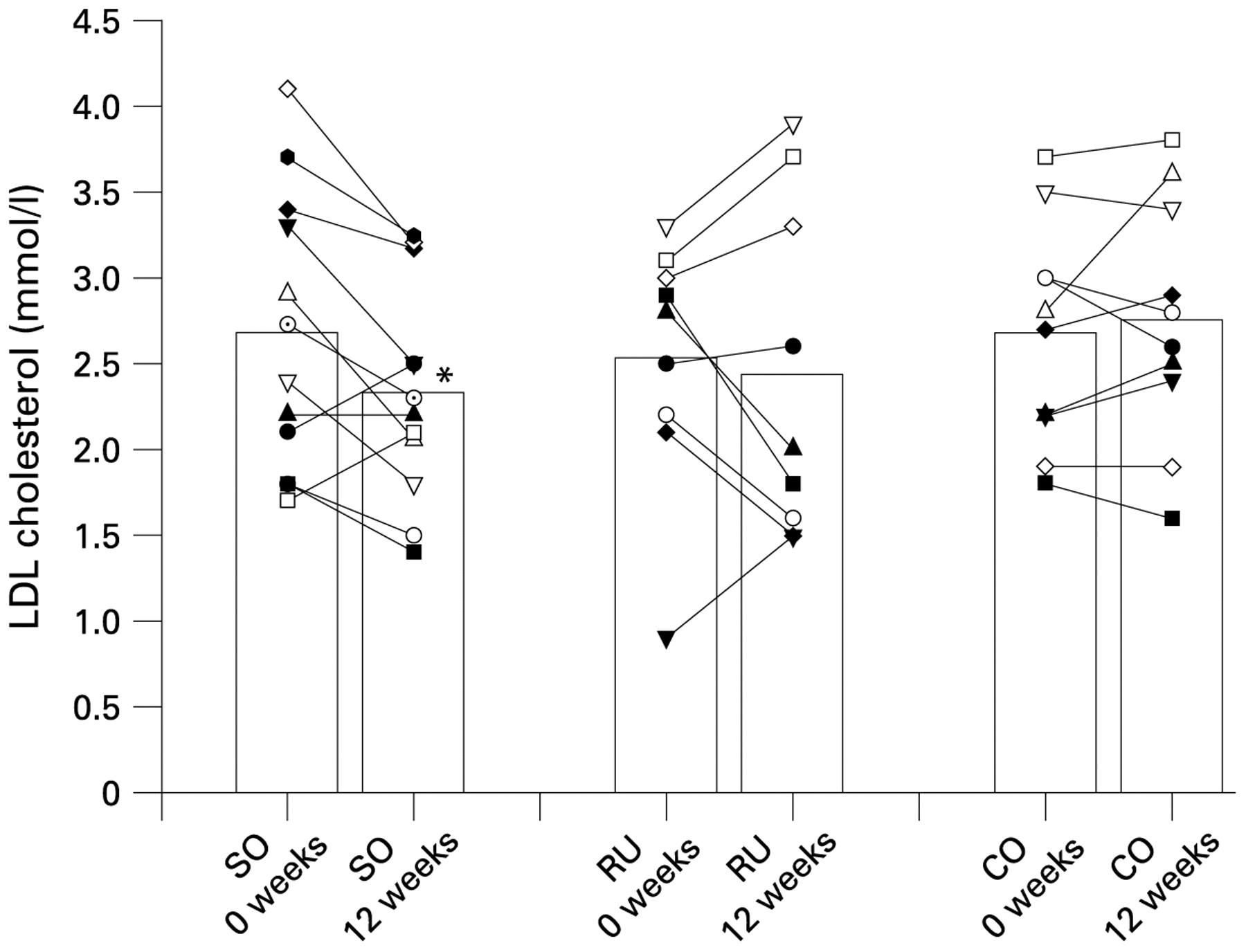
LDL cholesterol before and after 12 weeks of soccer practice (SO, n = 12) and running (RU, n = 9) for untrained men, or continuation of an inactive lifestyle (CO, n = 10). Mean and individual values are presented for 0 and 12 weeks. *Significant difference from 0 weeks.
Muscle capillaries
After 12 weeks, the number of capillaries per fibre was 23% (4%) and 16% (7%) higher (p<0.05) in SO and RU, whereas no change occurred in CO (fig 6). Changes in muscle capillaries over 12 weeks were greater (p<0.05) in SO than in CO, but not significantly different between SO and RU or between RU and CO.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Muscle capillaries before and after 12 weeks of soccer practice (SO, n = 12) and running (RU, n = 10) for untrained men, or continuation of an inactive lifestyle (CO, n = 8). Mean and individual values are presented for 0 and 12 weeks. *Significant difference from 0 weeks.
Discussion
The present study showed that a 12 week period of regular recreational soccer training lowered resting blood pressure, heart rate and fat percentage. In addition, in contrast to the running group, the soccer group elevated lean body mass and leg bone mass, increased fat oxidation during running and had a significant reduction in LDL cholesterol. These results suggest that the intermittent exercise with periods of near-maximal heart rates and multiple intense actions during soccer training effectively stimulates musculoskeletal and cardiovascular adaptations throughout a 3 month training period.
The reduction in systolic and diastolic blood pressure of 8 and 5 mm Hg, respectively, after the 12 weeks of soccer training is of a magnitude that has been suggested to have significant health-beneficial effects.28 Thus, the risk of cardiovascular death was shown in a meta-analysis of 61 prospective studies to decrease linearly with decreasing blood pressure until a systolic pressure of 115 mm Hg and a diastolic pressure of 75 mm Hg.29 Blood pressure changes similar to those for the soccer group were observed for the running group, which also had a response which was greater than normally seen after 12 weeks of training. In a meta-analysis including healthy sedentary normotensive or hypertensive adults with an intervention duration of at least 4 weeks, involving 72 trials, 105 study groups, and 3936 participants, Cornelissen and Fagard found that training induced significant net reductions in both resting systolic and diastolic blood pressure of about 3 mm Hg.29 Furthermore, in accordance with the present study (fig 3), the reduction of resting blood pressure was more pronounced in the 30 hypertensive study groups (6.9/4.9 mm Hg) than in the normotensive study groups (1.9/1.6 mm Hg). The lowered blood pressure was associated with a reduction in resting heart rate, which may reflect a reduction in sympathetic outflow and thereby reduced systemic vascular resistance. In addition, muscle capillarisation was considerably elevated in the soccer group (23%) after the 12 weeks of training (fig 6). It is possible that other vascular structural adaptations may have occurred.30 These include vascular remodelling, that is, increased length, cross-sectional area, and/or diameter of already existing arteries and veins, as has been observed in endurance-trained rats.31 Furthermore, a lowered precapillary vascular resistance of hindquarters isolated from trained normotensive32 33 and spontaneously hypertensive rats has been demonstrated.34 Together, the elevated number of capillaries and these other possible training-induced alterations in vascular structure may have lowered the peripheral resistance and in part explain the reduced resting blood pressure.
In the soccer group fasting serum LDL-C was lowered by 15%, which is of great importance, since LDL-C is a powerful CAD risk predictor. The running group had no change in LDL-C, which is in accordance with most studies using aerobic exercise training,7 15 16 17 18 except for a few studies.19 In the present study HDL-C was unaltered in both training groups. HDL-C is generally responsive to aerobic training and increases in a dose-dependent manner with increased energy expenditure.9 11 13 14 However, it requires at least 12 weeks of training and not all studies have shown an effect.11 12 Thus, despite the fact that the extra total energy turnover, estimated from HR measurements during training and an individual relationship between oxygen uptake and heart rate, of about 3000 kJ per training session was high for both the soccer and running groups, it may have been that the training period was too short in the present study to demonstrate an effect on HDL-C.
Fat mass in the soccer group was lowered by 2.7 kg after 12 weeks of training, with the major part lost from the upper body (table 2). In association, the oxidation of fat during a standard intense running exercise bout (9.5 km/h) was six times higher, determined on the basis of the measured RER values. It should be noted that the fat loss for the soccer group was more pronounced than in the running group, which had a decrease in fat mass (1.8 kg) which is similar to a number of other studies using running as an intervention.35 36 In contrast to the running group, the soccer group had an increase in lean body mass after the training period, suggesting that the soccer practice led to muscle hypertrophy. The observed increase in lean body mass of 1.7 kg over 12 weeks is of similar magnitude to that observed for strength training.35 36 The present study also showed that lower extremity bone mass was elevated by short-term soccer training but unaltered in the running group, which is in line with the conclusions from cross-sectional studies that long-term participation in soccer results in a high bone mineral density and bone mass.37 38 Together, the present findings provide evidence that soccer training effectively stimulates musculoskeletal adaptations to an extent that is likely to benefit the participants in a number of daily activities and may result in a lowered risk of bone fractures.
The soccer group had a 7% increase in VO2max during the first 4 weeks of training and a further increase of 6% during the next 8 weeks. The running group had a 6% increase in the first period, but no further improvement during the last period, suggesting that the stimulus of factors determining VO2max during the running was not large enough.21 39 The two groups had the same average heart rate during the training, but with a much greater distribution of the heart rate in the soccer group, reflecting the marked and frequent changing in exercise intensity when playing soccer (fig 1). For example, in the soccer group heart rate was above 90% of HRmax for 20% of the training time in comparison to only 1% for the running group. Thus, it is likely that it is the high-intensity periods which make soccer training superior to running training in creating further improvement in VO2max. In agreement, studies have demonstrated that elevating the running speed during training can improve VO2max in endurance-trained runners.39 Interestingly, even though the soccer players had more frequent and longer periods with a heart rate above 90% of HRmax than the runners, the perceived exertion was lower in the soccer group. It should be noted that both groups had high attendance rates, but psychological analysis revealed that the soccer players, in contrast to the running group, did not express any type of resistance against training and were highly motivated for the sport itself (data not shown). The soccer training was self-controlled and the players developed social interactions (data not shown), also leading them to ask about the possibility of continuing to play after finishing the study. Apparently, soccer can be used as a health-promoting activity with potential for permanent implementation. Future studies using physiological, psychological and sociological data collection can provide valuable information about the impact of soccer training for adult female players, youth players and elderly players with elevated risk of lifestyle diseases. Additionally, it would be of interest to study the health effects of other intermittent sports with multiple intense actions and periods of near-maximal heart rates, such as basketball, team handball, floorball and rugby.
In summary, regular soccer training organised as small-sided drills was shown to have significant health-beneficial effects for untrained men. It elevated maximal oxygen uptake and fat oxidation during exercise and lowered blood pressure, fat mass and blood LDL cholesterol. In contrast to the running group, lean body mass and leg bone mass were increased in the soccer group. Furthermore, the perceived exertion during the soccer training was lower than that observed during running.
What is already known about this topic
The positive cardiovascular effects of regular continuous exercise training, such as running, cycling and swimming, are well documented.
What this study adds
The present findings provide evidence that soccer organised as simple 5v5 and 7v7 games has significant cardiovascular and musculoskeletal effects for untrained men, including overweight players with limited football experience and skills. Soccer is a popular team sport with more than 400 million active players worldwide, and due to motivational and social factors it may have great potential for long-term health promotion for inactive but football-passionate individuals.
Acknowledgments
We thank all the participants and Rikke Leihof, Mihai Ursta Relu, Rasmus Bischoff, Mads Bendixen and Thomas Gunnarsson for excellent technical assistance. The study was supported by the Danish Ministry of Culture (Kulturministeriets Udvalg for Idratsforskning) and by the Danish Football Association.
REFERENCES
Footnotes
Competing interests None.