Article Text

Abstract
Objective: To summarise the best available evidence to determine if facial protection reduces head injury in ice hockey.
Data Sources: MEDLINE and Cochrane databases through January 2009.
Review Methods: Utilising terms: “head injuries,” “craniocerebral trauma [MeSH]”, “head injuries, closed [MeSH]”, head injuries, penetrating [MeSH]”, “face mask”, “face shield”, “visor” and “hockey”, 24 articles were identified through our systematic literature search. Of these, six studies met the inclusion criteria. Three independent reviewers reviewed the articles. The study results and generated conclusions were extracted and agreed upon.
Results: Studies reviewed suggest that facial protection reduces overall head injuries in ice hockey. Facial protection showed a statistically significant (p<0.05) reduction in the number and type of facial injuries. In studies evaluating full facial protection (FFP) versus half facial protection (HFP), FFP offered a significantly higher level of protection against facial injuries and lacerations than HFP (relative risk (RR) 2.31, CI 1.53 to 3.48). There was no significant difference in the rate of concussion (RR 0.97, CI 0.61 to 1.54) or neck injury (CI 0.43 to 3.16) between full and partial protection. In those who sustained concussion players with FFP returned to practice or games sooner than players with partial facial protection (PFP) (1.7 sessions, CI 1.32 to 2.18).
Conclusions: There is good evidence that FFP reduces the number and risk of overall head and facial injuries in ice hockey compared with PFP and no facial protection. PFP, while not as protective as FFP, appears to offer more risk reduction than no protection.
Statistics from Altmetric.com
Worldwide, ice hockey is a popular sport with a participation of over 1 million players in the USA and Canada alone.1 2 It is anticipated that this number will continue to grow as the popularity of ice hockey increases. As participation increases, the number of injuries seen in ice hockey will also increase. The risk of injury in ice hockey is high, with players travelling up to 30 mph and a puck exceeding 100 mph.3 Ice hockey provides an environment extremely conducive to the occurrence of head and facial injuries, with multiple opportunities for high speed collisions with other players, fast moving objects, sticks and unforgiving surfaces.
Early investigations performed before the mandatory facemask and helmet rules demonstrated a high incidence of facial injury and lacerations.4 5 Stick-related head and facial injuries have been the cause of up to 14% of injuries in other studies, especially studies reporting injuries from European teams, whose players are often not required to wear facemask protection.3 5 Concussion also remains a serious concern in this population and accounted for nearly one out five injuries in ice hockey.6 Not surprisingly, head injuries constitute 10–40% of all hockey-related injuries, with traumatic brain injuries accounting for 10–15%.7 The annual incidence of concussions seen in German ice hockey has been reported as 3.7 per 100 athletes.8 In the 1970s and 1980s, full face masks became mandatory for secondary school and collegiate hockey players because of concerns for ocular and dental injuries.
With the increase in head injuries as hockey evolved, further protective headgear recommendations followed, and helmets are now required at all levels of play. The widespread use of helmets with face masks has essentially eliminated ocular, facial, dental and extracranial head injuries in amateur leagues, but brain injuries remain a serious concern. With the increased utilisation of protective gear, there appears to have been an associated increase in the level of aggressive play and a concomitant rise in the occurrence of concussions and spinal injuries.7 Until recently, there was speculation that the added mass and area of a helmet and full face shield (FFS) may increase the rotational acceleration of a player’s head following impact, producing greater neuronal shearing forces and increased severity of concussion.9 10 It has also been hypothesised that increased facial protection may lead to more aggressive play and actually lead to more head and facial injuries in hockey.
While wearing a helmet is now required by the National Hockey League (NHL), facial protection remains optional. It is unknown to what degree face visors influence concussion, other head injury and eye injury rates in hockey. The purpose of this systematic review was to evaluate the best available evidence to determine if facial protection provides additional benefit in the prevention of head injuries in ice hockey.
Materials and methods
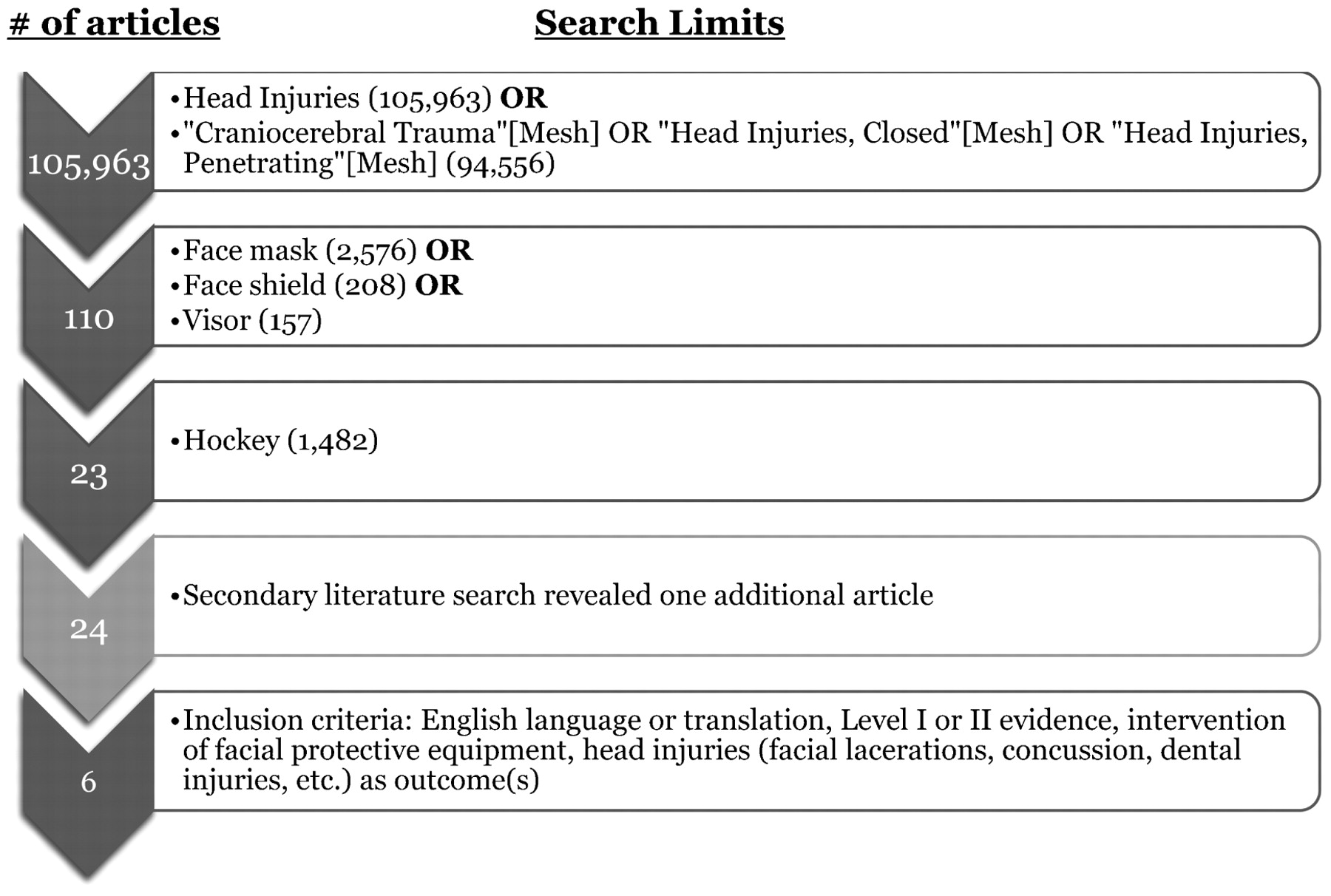
A literature review was completed using MEDLINE and Cochrane database searches to January 2009 to identify all English language or translated clinical papers that assessed the impact of the use of facial protective gear on the prevention of head injuries in ice hockey. Head injuries were defined as any injury to the head, face or teeth. Injury was defined as any event requiring attention from medical personnel. Several key search terms were used to narrow our literature search (fig 1). Initially, “head injuries” was used, with 105 963 articles identified. Re-entering “head injuries” as a MeSH term yielded no additional articles. Key terms used for protective headgear included “face shield”, “face mask” and “visor.” These terms were run through the databases independently and then collectively, generating 2910 articles. When combined with “head injuries”, a total of 110 articles was identified. The term “hockey” was added to narrow the literature to 23 relevant articles.

{kind=link}
Diagrammatic illustration of systematic literature search. Primary search terms and results (blue), secondary search results (light grey), and applied inclusion criteria and results (dark grey) are shown. The number of articles identified by each search term is noted in parentheses.
A secondary search of references from relevant articles was also performed, yielding one additional article. Further criteria for inclusion in this review were then applied to the 24 articles. Articles had to be of level I or II evidence for prognostic studies (prospective study, systematic review of level I studies, retrospective study, study of untreated controls from a previous randomised controlled trial, or systematic review of level II studies).11 Articles must also have included the use of facial protective equipment as an intervention and head injuries (facial lacerations, dental injuries, concussions, etc) as a clinical outcome. Applying these criteria, a total of six articles was identified as meeting our criteria for systematic review (fig 1). Of the 24 articles, 11 were excluded because they were not of level I or II evidence. Another five were excluded because head injury outcomes were not assessed and two were excluded because facial protective gear was not used as an intervention.
Three independent reviewers, using predetermined methodology, as described by Spindler et al,11 reviewed and scored the six articles included in this systematic analysis and reached consensus through discussion. The study methods and demographic data were first identified with attention to the study type, objectives, outcome measures and examined cohorts. The study results and generated conclusions were extracted and agreed upon.
Results
Results for the six studies meeting inclusion criteria for this systematic review are summarised in tables 1 and 2.
Systematic review demographics and methods
Systematic review results and conclusions
Studies
Amateur hockey
Stuart et al,12 using a prospective study design, evaluated the effect of facial protection on head, neck and facial injuries in elite amateur ice hockey players. The results of this study showed that the use of full and half-face shields reduce the risk of eye and facial injuries compared with no facial protection (NFP). In addition, there was no increase in the incidence of concussion or spinal injuries in the players wearing facial protection. As in similar studies, facial, dental, eye and head injuries were reported regardless of time lost. In comparison to other studies, the principal difference in injury definition in this study was the inclusion of neck injuries that did not result in time lost from play.
Limitations of the study include restricted data collection for playing time and injuries, which were only recorded during home games. Therefore, injuries from away games were not included in the analysis and this limits the study results. Also, players under the age of 18 years had to wear mandatory full facial protection (FFP), whereas players above the age of 18 years could choose to wear a full shield, half shield, or no shield. It is unclear if the injury pattern for those under 18 years differed from those over 18 years. Varying styles of play, such as more aggressive or conservative play based on age, may have skewed the results. These age-related differences may bias the study results. It is also unknown if there are variables among players that influence the choice of FFS use or not. It is possible that these variables could confound the study results.
Collegiate hockey
In a study of 642 Canadian college hockey players, Benson and colleagues,13 14 looked at the use of FFS versus half face shields (HFS) regarding head and neck injuries and the incidence of concussion.13 14 A power analysis and sample size calculation was performed, and the study was appropriately powered for the primary outcome. The study revealed that the use of FFS significantly reduced the risk of facial and dental injuries compared with the use of HFS without an increase in the risk of neck injuries, concussions, or other hockey-related injuries. Concussion risk in this cohort was similar among players, regardless of the type of face shield use (FFS vs HFS). Interestingly, those players wearing a FFS returned to play sooner following a concussion than those players wearing a HFS. Moreover, the use of a mouth guard allowed for a faster return to play following concussion regardless of face shield type.
This study used an injury surveillance system to collect nearly 100% of injury data for this cohort while controlling for between-group variables. Despite the accuracy of data collection, the relative severity of injury between the groups (FFS vs HFS) was not determined. Injury severity was defined only by time lost due to injury and those injuries without time lost were not recorded. Also, there may have been differences between team therapists and physicians in their return to play protocol, which may have further skewed the injury severity data. Other limitations of this study include lack of generalisability to high-school age or younger skeletally immature players.
LaPrade et al4 prospectively evaluated almost 800 practice hours and 163 games of US division 1 hockey players to assess the effects of wearing a face shield on facial lacerations and head and neck injuries in collegiate hockey. The results of this study showed that there was a dramatic decrease in head and neck injury and facial lacerations in both games and practices after the introduction of a FFS compared with the use of NFP. Injuries were only recorded if they caused a player to miss a game or practice. This definition could have excluded a significant number of less severe injuries such as facial lacerations. Data analyses included all players on the ice during practices and games, including the goalie. It is not clear if there was a difference in injury rates among goalies before and after mandated FFS use. This could have biased the results as the goalie was required to wear FFP throughout the entire study period.
This study differed from the study by Benson and colleagues13 14 as it used a historical cohort of players with NFP as a control group for comparison. The use of this historical cohort instead of an actual control cohort is a relative limitation in study design. Sample size calculation and power analysis were not performed so it is unclear if this study was appropriately powered to show statistical significance for the primary outcome. Despite the difference in methodology and the study limitations, the findings support the results of the study by Benson and colleagues.13 14
Professional hockey
Stevens et al10 followed over 800 NHL players prospectively over the course of one complete season to evaluate the impact of face visors on concussions, other head injuries and eye injury rates at the professional level.10 Results from this prospective cohort showed that the use of facial protection (FFS or HFS) significantly reduced the risk of facial and eye injuries in comparison with NFP. There was no increased incidence of neck injuries or concussions in the players wearing facial protection compared with those not using facial protection. In addition, FFS use reduced the risk of facial and eye injuries significantly more than the use of HFS.
Limitations of this study included the method of data collection. Injury data were recorded from a hockey register and not prospectively by an investigator. The type of facial protection wear was determined by a review of sports cards and NHL photographs, which may not be representative of the players’ actual use during the entire season. This methodology of review for facial protection had been validated in a much smaller study but it remains unknown if it is accurate and truly representative of facial protection used by players. Finally, power analysis or sample size calculation was not performed.
Minor league hockey
Bunn15 evaluated the use of HFS compared with NFP in reducing the severity of facial injuries and eye injuries over the upper half of the face in East Coast Hockey League players.15 Injury data were collected in a prospective fashion but were evaluated retrospectively. Results of this study showed no difference in injury risk between players using HFS compared with those using NFP. Limitations of this study include the use of a non-validated injury severity score, which was weighted heavily towards eye injuries compared with other head injuries. The study was also influenced by selection bias as the study groups were limited and not all players with injuries were included for analysis. It is unclear whether the results of the study would be different if all players with injuries were included for analysis.
Discussion
Overall head and neck injuries
It has previously been hypothesised that added facial protection (FFS or HFS) may increase the risk of head and neck injuries in ice hockey. One reason for this concern is that the use of facial protection in ice hockey may give players an increased sense of invincibility, leading players to take excessive and unwarranted risks. This hypothesis has been supported in previous studies. Gerberich et al16 reported that 66% of surveyed high school hockey players from Minnesota felt that the requirement of the face mask allowed them to be more aggressive in their style of play. This perception of increased aggressive play with the use of facial protection leading to increased head and neck injury is not consistent with this systematic review (table 3).
Impact of facial protection on head (non-concussive) and neck injuries
Results from our systematic review support the protective effect of FFS use in reducing the severity of concussion and facial, eye and dental injuries, without increasing the risk of other head and neck injury. Results also show that the lowest overall rate of injury was seen in the FFS cohorts compared with the HFS and NFS cohorts. The use of half face shields did prove to be more protective than NFP. There was no significant difference in neck injury between the cohorts, suggesting that facial protection does not lead to an increase in the overall risk of head and neck injury compared with the use of NFP. The hypothesis that facial protection in ice hockey increases the potential for the overall risk of head and neck injury compared with NFP is inconsistent with the findings of this systematic review and should not be used as a reason to discourage the use of facial protection in ice hockey.
Concussions
Historically, helmet use alone has not been found to be protective against concussions in either football or hockey.17 As with the overall risk of head and neck injury, there has been concern that the use of FFS or HFS in ice hockey would lead to an increased risk of concussion. The results of our systematic review suggest that there is no increased risk of concussion in ice hockey players using facial protection (table 4). Our systematic review further reveals that there is no difference in the risk of concussion in ice hockey players regardless of facial protection used (FFS vs HFS vs NFS). There does appear to be a faster return to play from concussion in players wearing a FFS compared with those wearing a HFS, which suggests that the severity of concussion may be less in players wearing FFP. Overall, the results of our systematic review suggest that the use of facial protection in ice hockey does not lead to an increased risk of concussion, and that the use of a FFS may actually decrease the severity of concussion and allow for fewer missed practices and games with a faster return to play.
Impact of facial protection on concussion
Although the benefits of mouth guard use in protecting athletes from dental injury is supported in the literature, controversy exists as to whether mouth guard use can reduce athletes’ risk of concussion.18 At this time, there is no clear association between mouth guard use in ice hockey and reduced concussion risk, but there may be less time lost following concussion in those players wearing a mouth guard and a FFS compared with those wearing a FFS alone. This potential benefit, along with the decreased risk of dental injury, supports the use of mouth guards in ice hockey.
Facial lacerations and dental injuries
There is good evidence that the use of a FFS in ice hockey reduces the number of facial lacerations compared with the use of a HFS or NFS (table 5).
Impact of facial protection on lacerations and dental injuries
Our systematic review illustrates that the mandatory use of FFS in ice hockey results in a reduction in the number of facial lacerations and dental injuries among ice hockey players. It appears that use of a HFS does not confer the same protection from facial lacerations as the use of a FFS. There is also a significant increased risk of dental injury with partial facial protection (PFP) compared with FFP. Moreover, the use of a HFS has been associated with more severe facial lacerations when compared with a NFS control. This result is influenced by the use of a non-validated injury-grading tool, which preferentially gave lacerations closer to the eye a higher injury score than other facial lacerations. Our systematic review found that the use of a FFS results in a decreased risk of facial lacerations and dental injuries compared with the use of a HFS or NFS. Whether there is a difference in the risk of facial laceration or dental injury in players wearing a HFS compared with NFS remains unclear.
What is already known on this topic
Ice hockey is a fast, high impact sport with a high propensity for head and facial injuries.
What this study adds
FFP reduces the number and risk of overall head and facial injuries in ice hockey.
PFP, although not as protective as FFP, appears to offer more risk reduction than no protection at all.
Limitations
This systematic review does have several limitations. The pre-hoc search strategy and inclusion criteria employed for this review were limited to high level clinical outcomes studies and only produced six studies meeting criteria sufficient for review. There are studies of lesser levels of evidence that address this topic, but their results are limited by study methodology and a lack of control groups. Although we recognise that these studies may contribute to the overall body of literature on this topic, our purpose was to examine the best clinical outcomes evidence to arrive at our conclusions regarding facial protection in hockey.
A second limitation of this systematic review is the definition of head injury used for this review. Although we tried to be inclusive in our definition of head injury to include any injury to the head, face or teeth, all of the studies used various definitions of head injury. The lack of a uniform definition of head injury and the severity of injury among these studies is a limitation and makes generalisation of the results more difficult in this review.
The results of this review are limited to the populations represented in the studies; specifically men in amateur, collegiate or professional hockey. The results of this review do not consider women’s or youth hockey and may not be generalisable to these populations. It should be noted that FFS are mandatory in youth and women’s hockey and we would suggest that the benefits noted in this review from the use of a FFS are also present in these populations even if they are not specifically included in this review.
The final limitation of this review is related to the lack of uniformity among the reviewed studies with respect to data collection and the definition of injury severity. All of the studies reviewed used various forms of data collection and this is a potential limit to the conclusions of this review. Because most studies used time lost to play to estimate injury severity, it is possible that this could lead to misclassification of injuries and bias the overall recommendations of this review. It would be preferable to have a uniform method of data collection and a more objective definition of injury severity in individual studies to strengthen this review.
Conclusion
Based on the results of our systematic review, we strongly recommend FFS protection with a mouth guard to reduce the number of head injuries and time lost from practice or games across all levels of ice hockey. The lowest overall rate of injury was seen with FFP, whereas PFP had a lower rate of injury than NFP. FFS have been shown to decrease concussion severity and rates of facial, eye and dental injuries, without increasing the risk of other head and neck injury. Half face shields, although not as protective as FFS, have been shown to be more protective than NFS. Mouth guards, while not decreasing the number of concussions in ice hockey, have been shown to allow for a faster return to play following concussion, suggesting milder head injury in those wearing mouth guards. Despite these results, more prospective evidence is needed to evaluate further the role of protective equipment and injury reduction in ice hockey. The results of this systematic review should prompt administrators in hockey leagues at all levels to consider strongly mandatory FFS use.
REFERENCES
Footnotes
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.