Article Text

Abstract
Objective To investigate the regulation of blood pressure in response to an orthostatic challenge in athletes running a marathon.
Methods 10 experienced male runners (mean (SD) age 29 (4) years) were tested on the day prior to the 2004 London Marathon, and again immediately postrace (race time 210 (36) min). In addition, 6 of the subjects were retested 24 h postrace. During each examination, beat-to-beat systolic arterial blood pressure (SBP) and heart rate (HR) were measured, and stroke volume (SV), cardiac output (CO) and total peripheral resistance (TPR) were estimated via arterial transmural pressure waveforms during 3 min in a supine position and then during 3 min of upright, unsupported standing. Data were averaged over 20 s epochs, and the final 20 s of each posture were compared prerace and postrace via repeated measures 2-way ANOVA.
Results Prerace SBP in standing increased only moderately when compared with supine values (2 (9) mm Hg, NS). This was accompanied by an increase in HR (13 (7) beats/min, p<0.05), as well as a decrease in SV (16 (9) ml, p<0.05). However, there was little change in CO (−0.13 (0.97) litres/min, NS) or TPR (0.047 (0.280) medical units (MU), NS). Postrace SBP significantly decreased from supine to standing (−15 (20) mm Hg, p<0.05). The change in SBP was accompanied by an increase in HR (19 (6) beats/min, p<0.05) and a reduction in SV (26 (14) ml, p<0.05) and CO (−1.02 (1.39) litres/min, p = 0.05). Postrace there was no change in TPR (0.366 (0.607) MU, NS) upon standing. The orthostatic adjustments in SBP, HR and CO were greater than at prerace (p<0.05). The postrace orthostatic challenge resulted in only one subject experiencing presyncopal symptoms. At 24 h postrace, cardiovascular responses to an orthostatic challenge mirrored those at prerace.
Conclusions Following prolonged exercise, a fall in systolic blood pressure during orthostasis results from an inadequately compensated decrease in SV and resultant CO during standing.
Statistics from Altmetric.com
Movement from a supine or seated to a standing position provides a significant orthostatic challenge as it causes blood to be displaced from the central circulation to the periphery and thus transiently reduces blood pressure. The associated fall in cerebral blood flow may be sufficient to provoke syncopal symptoms (dizziness, disorientation, blurred vision, yawning and collapse) or event (abrupt, sudden and complete loss of consciousness and postural tone). Generally, compensatory responses such as increases in heart rate (HR)1 and/or total peripheral resistance (TPR)2 prevent a sustained decrease in blood pressure during an orthostatic challenge, hence maintaining blood pressure at the level necessary to maintain appropriate cerebral perfusion.
Exercise can provide a significant challenge to homeostatic regulation and maintenance of blood pressure immediately following intermittent3 and maximal exercise.4 5 In ultraendurance events (>12 h), Finlay et al6 and Lucas et al7 reported episodes of presyncope and orthostatic intolerance (OI) (the inability to stand upright, motionless and unaided, culminating in the desire to return to a supine/seated position) following exercise and suggest that this is due to venous pooling in the lower limbs and inadequate compensatory responses in CO leading to impaired cerebral perfusion.7 The postexercise period itself is characterised by hypotension,8 9 which, when combined with gravitational stress, may exacerbate OI. Scott et al8 used Lower Body Negative Pressure (LBNP) postexercise to address this issue, and found that the cardiovascular responses to LBNP were attenuated postexercise.
Whilst there is a link between postural orthostatic hypotension and the onset of syncope1 following a bout of high-intensity exercise and ultraendurance events, we know less about the impact of the completion of a marathon upon orthostatic tolerance, i.e. potential “orthostatic weakening” and alterations in BP regulation. Given that this is a mass participation event, the aim of this research was to describe the effects of this form of exercise upon blood pressure and other indices of cardiovascular function during an orthostatic challenge before and after a marathon race in orthostatically tolerant runners.
Methods
Participants and design
Ten male athletes were recruited in the weeks preceding the 2004 London Marathon. Each individual provided written informed consent, and study approval was obtained from Liverpool John Moores University Ethics Committee. All participants (mean (SD) age 29 (4) years, body mass 75.8 (8.2) kg, height 175.4 (7.8) cm) were examined on the day prior to the race and immediately following (within 60 min) race completion (race finish time 210 (36) min). In addition, six of the participants were tested 24 h postrace. Throughout the 26.2 miles of the race, and during the postrace period, participants ingested fluids ad libitum. The temperature range over the period of time the athletes took to complete the marathon was 10–11°C, and the conditions were mostly cloudy with light rain.
Protocols
Each protocol was repeated three times: prerace, immediately postrace and 24 h postrace. All tests were conducted in a room at constant temperature (22–24°C). Body mass was recorded at all test times using portable electronic scales (Model A3JJT1K, Hansen, UK). During each assessment period participants initially rested in the supine position whilst blood pressure monitoring equipment was attached to the third and fourth fingers of the right hand, which had been placed in a standard glove to maintain hand temperature. Following this, arterial pressure pulse wave (PortAPres, Amsterdam) recording commenced, and continued over a 3 minute period whilst the subject remained stationary and quiet in a supine position. Participants were then instructed to move to a motionless standing position for a further 3 minutes whilst breathing normally, weight equally supported on both feet. The PortAPres finger cuffs were maintained at heart level throughout the orthostatic challenge. This was achieved in standing via the support of a sling so there was no local muscle activity. Participants were monitored for signs of presyncope (dizziness, unsteadiness, facial pallor, diminished pulse, blurred vision). The trial was terminated following the 3 minutes of standing, or if the participant demonstrated significant presyncopal signs and/or became orthostatically intolerant.
The PortAPres allowed continuous and non-invasive recording of arterial blood pressure measurements on a beat-to-beat basis and has been shown to provide accurate measures of both absolute pressures at rest and change during interventions.10 These were downloaded to a computer using the BeatScope software package (version 1.1 — TNO BMI, Amsterdam). The inflatable pneumatic cuffs incorporate an infrared plethysmograph, which alters the cuff pressure. Pulse wave analysis from the finger pressure waveform enables the measurement and interpretation of haemodynamic parameters11: systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR) and cardiac output (CO), and subsequently calculations of stroke volume (SV) and total peripheral resistance (TPR). These estimated values have been shown to be reliable during interventions similar to those used here.12 13 The measurements were taken from the mid-phalanx of the third and fourth fingers of the right hand. Data collected for all variables were collected continuously over the supine and standing periods and then during analysis averaged over 20 second epochs.
Data analysis
All data are presented as mean (SD). The absolute mean data values for all cardiovascular variables recorded during the final 20 seconds in the supine and standing periods both prerace and postrace were analysed via repeated measures 2-way ANOVA. The difference (Δ, delta score) between supine and standing positions was calculated and compared between prerace, postrace and 24 h postrace via paired t test analysis. Post-hoc comparisons were made where significant F values were obtained using paired t tests with a Bonferroni correction. A critical alpha of 0.05 was selected throughout the analyses. All statistical analysis was undertaken with the use of SPSS (version 14.0 for Windows).
Results
Prerace orthostatic challenge
Cardiovascular measurements remained stable throughout the 3 min supine period. Baseline cardiovascular parameters were 136 (14) mm Hg (SBP), 73 (11) mm Hg (DBP), 5.50 (1.44) litres/min (CO), 65 (18) beats/min (HR), 92 (20) ml (SV) and 1.098 (0.406) MU (TPR). At the end of the 3 minutes of standing both SBP (137 (19) mm Hg, p = 0.58) and DBP (76 (11) mm Hg, p = 0.19; see fig 1) remained stable. The maintenance of BP occurred despite a significant decrease in SV from supine values (supine: 92 (20) vs standing: 78 (11) ml, p<0.05) as a result of a significant increase in HR (supine: 65 (18) vs standing: 91 (12) beats/min, p<0.05; see fig 2), in combination with a maintained values of TPR, such that CO was unaltered by posture. There were no signs of presyncope in any subject during the prerace orthostatic challenge.

Blood pressure responses to an orthostatic challenge prerace. Data were presented as mean (SD). No significant differences between supine and standing BP values.

Heart rate and stroke volume responses to an orthostatic challenge prerace. Data were presented as mean (SD). * p<0.05 Significant change in HR and SV following 3 minutes of standing when compared with supine values.
Postrace orthostatic challenge
Upon completion of the marathon, mean body mass decreased by 2.1 (2.7) kg. Postrace hypotension in the supine position was not evident (prerace: 136 (14) vs. postrace: 132 (23) mm Hg, p = 0.47), due to an increased HR (prerace: 65 (18) vs postrace: 82 (9) beats/min, p<0.05) offsetting a small decline in SV (prerace: 92 (20) vs postrace: 81 (16) ml, p = 0.08), creating a small but significant rise in CO (prerace: 5.50 (1.44) vs postrace: 6.55 (1.16) litres/min, p<0.05). A significant reduction in postrace supine TPR was noted (prerace: 1.098 (0.406) vs postrace: 0.794 (0.274) MU, p<0.05).
The postrace orthostatic challenge resulted in a decrease in SBP (supine: 117 (31) vs standing: 132 (23) mm Hg, p = 0.06), in part due to reductions in SV (81 (16) vs 55 (17) ml, p<0.05) and CO (6.55 (1.16) vs 5.53 (1.66) litres/min, p<0.05) and despite a significant increase in HR (82 (9) vs 101 (8) beats/min, p<0.05) and unchanged TPR (supine: 0.794 (0.274) vs standing: 1.160 (0.686) MU, p = 0.10). DBP was unaltered (supine: 71 (12) vs standing: 73 (16) mm Hg, p = 0.34); however, the participants demonstrated relative postural orthostatic hypotension (Δ SBP<20 mm Hg) in response to the 3 minute postrace orthostatic challenge.
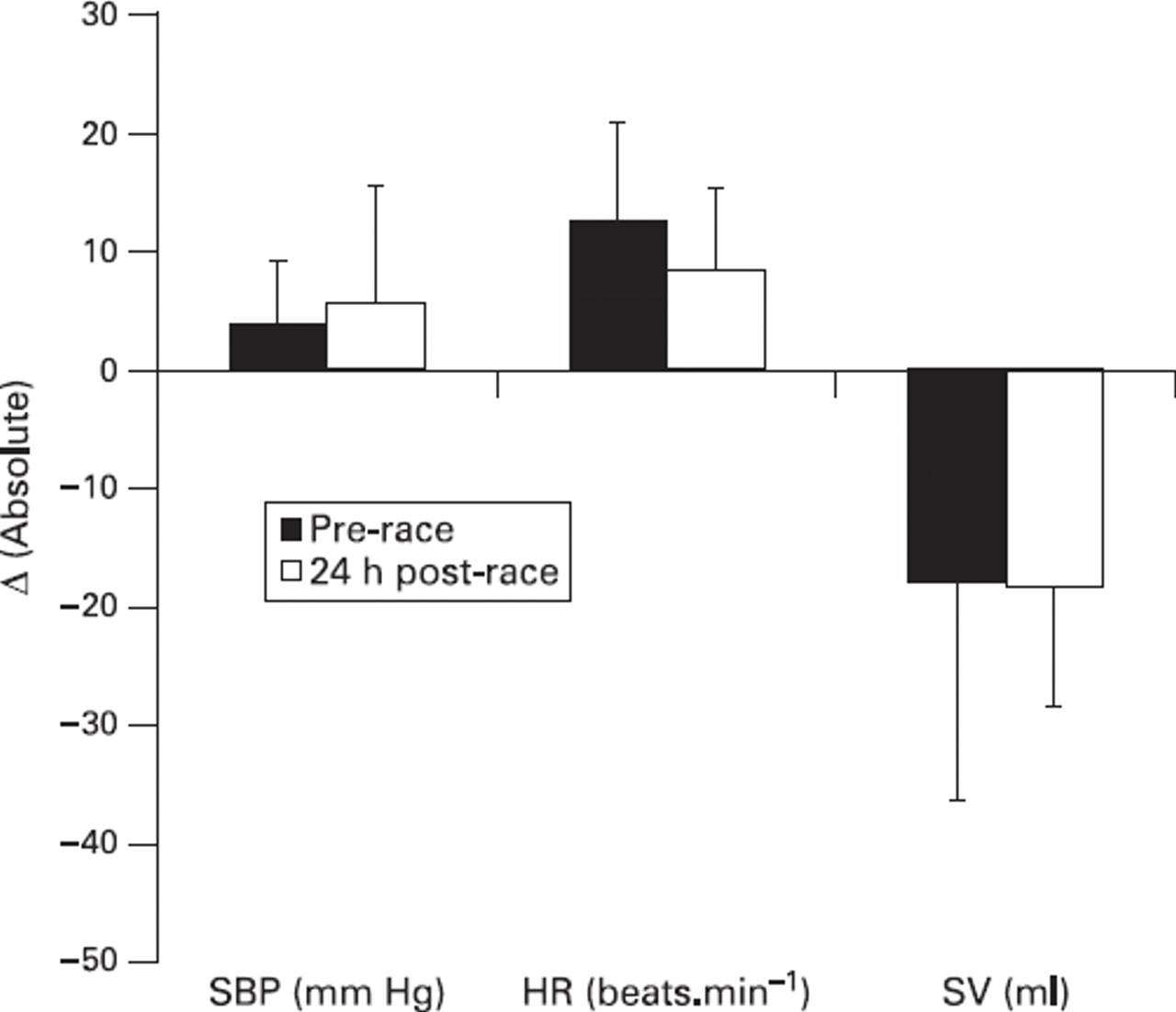
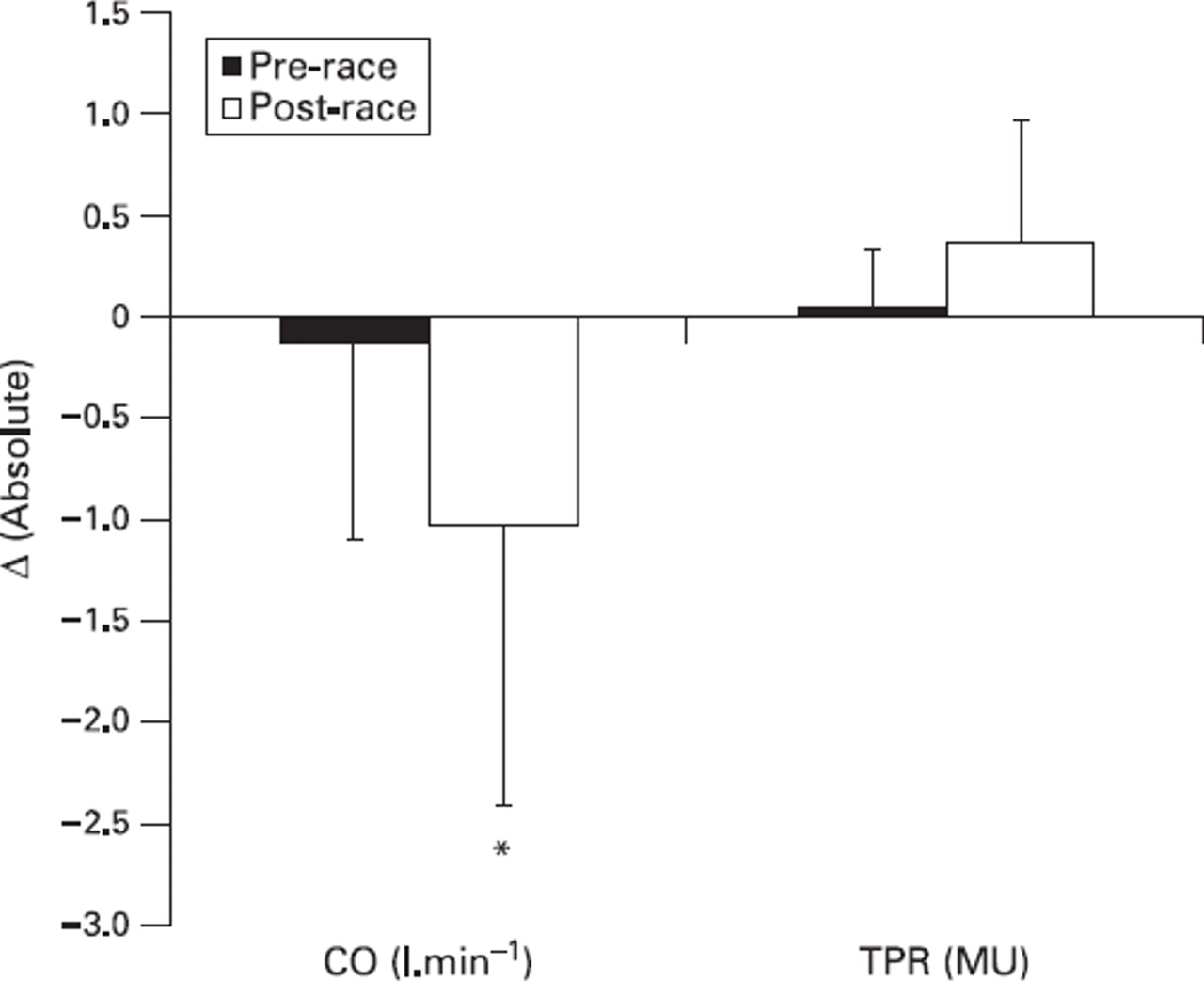
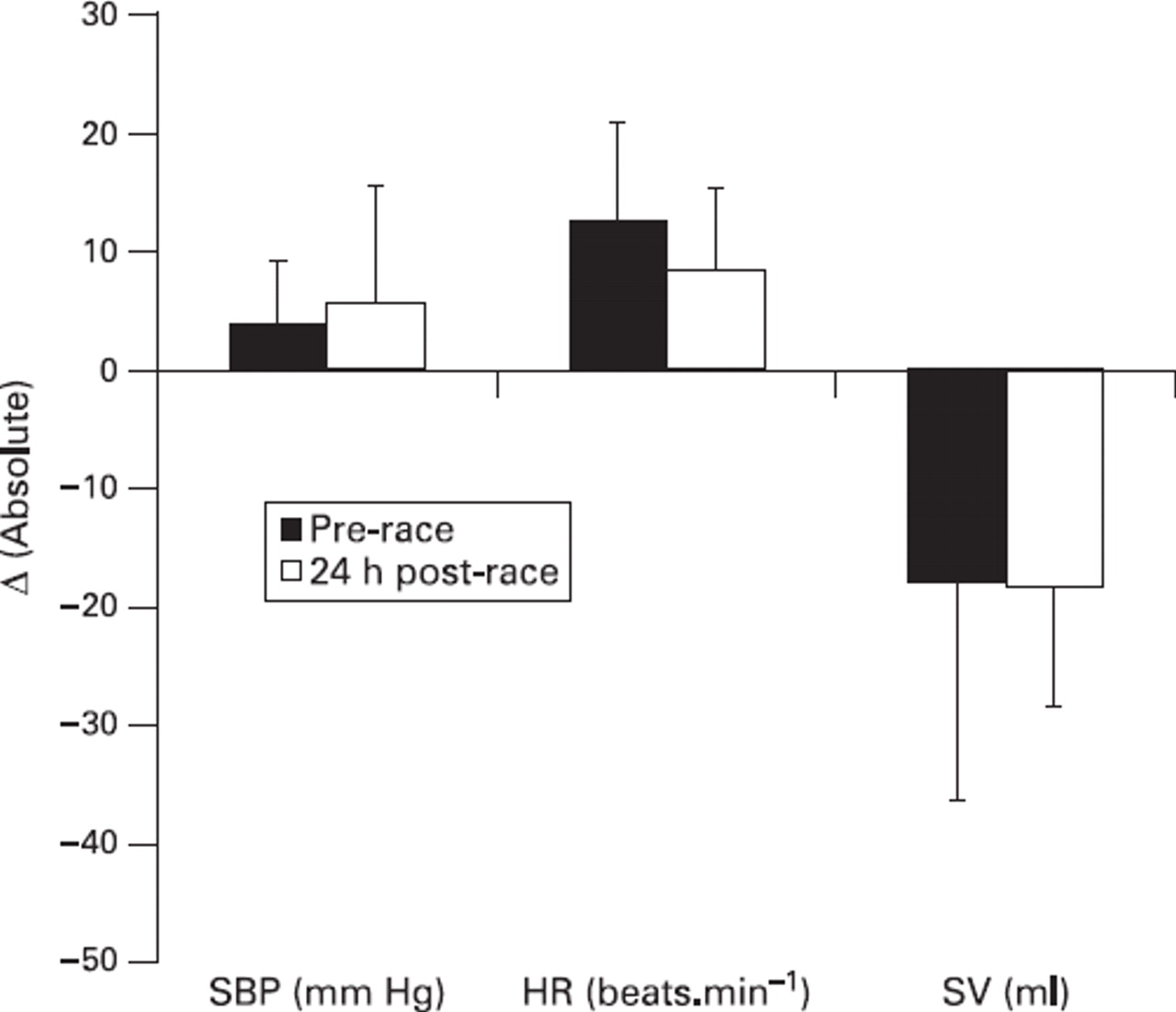
The delta scores (Δ) for SBP were significantly different between prerace and postrace (prerace: Δ1 (9) mm Hg vs post-race: Δ−15 (20) mm Hg, p<0.05; see fig 3). This was a likely result of a larger decrease in SV (prerace: Δ−16 (9) vs postrace: Δ−26 (14) ml, p = 0.09) and CO (prerace: Δ−0.13 (0.97) vs postrace: Δ−1.02 (1.39) litres/min, p<0.05; see fig 4) that was not completely offset by changes in TPR (prerace: Δ0.047 (0.280) vs postrace: Δ0.366 (0.607) MU, p = 0.16) or DBP (prerace: Δ3 (7) mm Hg vs postrace: Δ3 (7) mm Hg; p = 0.79). Changes in HR in response to standing were greater postrace (prerace: Δ13 (7) vs postrace: Δ19 (6) beats/min (p<0.05), and helped all 10 individuals to complete the postrace orthostatic challenge with only one subject demonstrating presyncopal symptoms (nausea) towards the end of the 3 min period.

Alterations in cardiovascular variables (stand – supine) during prerace and postrace orthostatic challenges. * p<0.05 postrace (white box) change significantly greater than prerace (black box) change.
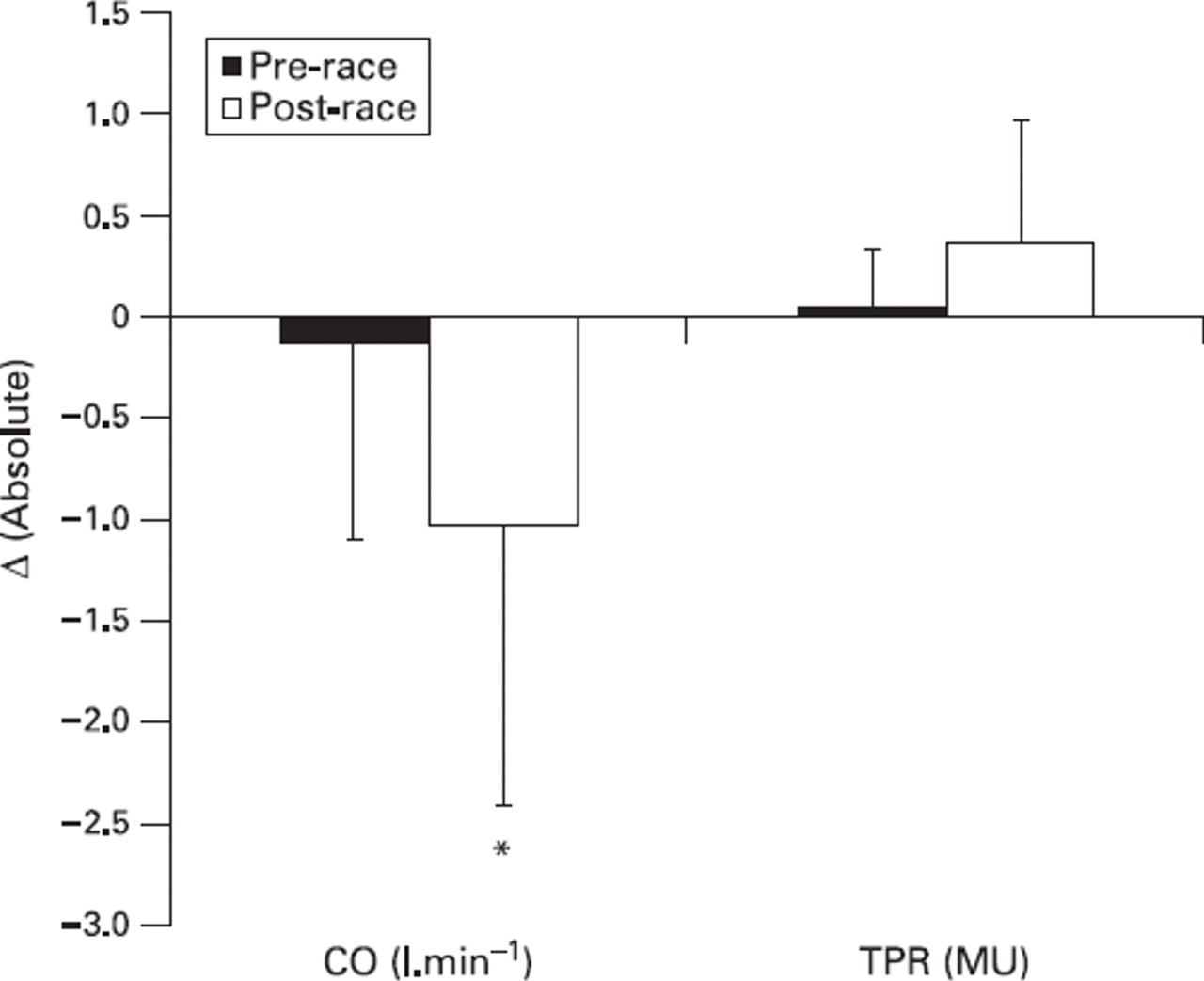
Alterations in cardiac output and total peripheral resistance (stand – supine) during prerace and postrace orthostatic challenges. * p<0.05 postrace (white box) change significantly different from prerace (black box) change.
24 h postrace
Six of the 10 participants returned for the third orthostatic challenge 24 h postrace. The average body mass recorded for this group is 75.6 (6.6) kg, which represented a return to baseline. Supine data, as well as responses of BP, HR, SV, CO and TPR to the orthostatic challenge, had returned to prerace values (figs 5 and 6). All participants were capable of completing the 24 h postrace 3 minute challenge without experiencing presyncopal symptoms.
Cardiovascular responses of orthostatically tolerant participants (n = 6) during prerace and 24 h postrace orthostatic challenges. There were no significant differences between periods.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cardiac output and total peripheral resistance responses of orthostatically tolerant participants (n = 6) during prerace and 24 h postrace orthostatic challenges.
Discussion
The main findings of this study indicate that both prerace and postrace orthostatic challenges induced a gravitational decrease in SV, leading to a marked reduction in blood pressure, which was corrected by a significant increase in HR in the prerace condition only. In the postrace period blood pressure remained below baseline despite a significantly greater increase in HR.
Immediately postrace, the participants were not hypotensive in the supine position despite a significant reduction in body mass (2.1 (2.7) kg), presumably due to fluid loss. This apparent dehydration was not associated with hypotension or a decline in CO, since HR was elevated. Indeed, in the supine position postrace CO was elevated. This data suggests that, in the supine posture postmarathon, there is no evidence to indicate heightened cardiovascular strain despite an almost 3% loss in body mass. The lack of postexercise hypotension is contrary to previous studies that have documented a fall in blood pressure in normotensive individuals in the supine posture that may last for up to 60 minutes4; however, these studies were concerned with the effect of shorter (<60 minutes) and much higher exercise intensities on recovery blood pressure.3,–,5 Given that the degree of postexercise hypotension is intensity and duration-dependent,14 this may explain this contrasting finding.
Postrace standing responses demonstrated a trend towards an orthostatic reduction in SBP, resulting in operative values significantly lower than prerace stand values. Nonetheless, defence of BP regulation was adequate, enabling each subject to complete the entire standing challenge. Throughout the 3 minutes of standing postrace, heart rate was elevated further (101 (8) beats/min, p<0.05) to compensate for the displacement of blood to the periphery and active muscles causing a reduction in central blood volume and therefore filling of the heart. Postrace, significant elevations in resting HR, in combination with larger relative (prerace: 20 vs postrace: 23%) and absolute (prerace: Δ13 (7) vs postrace: Δ19 (6) beats/min) increases in heart rate during the stand, may contribute to the maintenance of systolic blood pressure at a level sufficient to prevent OI subsequent to completion of the challenges.
Stroke volume postrace did not distinctly differ from prerace supine values (prerace: 92 (20) vs postrace: 81 (16) ml, p = 0.08). Postrace, however, there was a decrease in TPR and a trend displaying a reduction in stroke volume in the supine position in comparison to baseline values. At such a time, peripheral capacitance may be amplified, increasing circulatory stress postexercise, despite retaining a recumbent position. Upon completion of the postrace challenge, SV had significantly reduced to 55 (7) ml (p<0.05). This alteration in SV was greater than that observed during prerace orthostasis in absolute (prerace: Δ−16 (9) vs postrace: Δ−26 (14) ml) and relative (prerace: −17% vs postrace: −32%) terms, and relates to a redistribution of blood to the lower limbs causing greater reduction in central blood volume following the race. Due to gravitational stress during the standing phase, the volume of blood in the lower limbs is increased, causing blood flow “transit time” to be increased. Increases in transit time may be more evident during the orthostatic challenge due to decreased TPR relative to baseline prior to the postrace challenge. The reduction in central blood volume will ultimately lead to a reduced venous return and a consequent reduction in SV.
The reported reductions in SV were lower than those seen amongst asymptomatic high-fit, mid-fit and low-fit groups respectively, in response to −40 mm Hg LBNP (−39.6 (5.7)%, −23.1 (5.6)%, −34.7 (2.7)%).15 These values are in excess of the reduction noted here and likely reflect the more aggressive stimulus of LBNP. In the present study the reductions in SV did not reduce blood pressure to levels leading to presyncope.
Arterial hypotension is recognised as an imbalance in CO and TPR. In the current study, CO was significantly increased during the postrace challenge; however, TPR remained unchanged, inferring that, in the presence of a falling SV, HR is solely responsible for the maintenance of blood pressure. Subjects did not display alterations in CO or TPR as a result of the prerace challenge, suggesting that the current group of subjects regulate BP via an increased cardiac sympathetic drive. The finding that TPR does not increase in response to orthostasis postrace is consistent with the observation of decreased vascular responsiveness to sympathetic stimulation in recovery from exercise.16 Indeed, at this time, as well as the lack of responsiveness to sympathetic vasoconstriction, it is likely that there is increased vasodilator activity due to the accumulation of metabolites from the preceding exercise. If the orthostatic challenge were of longer duration, it is likely that the lack of vasoconstrictor responsiveness and background dilator activity would reduce TPR further, leading to a greater fall in pressure and causing the onset of syncope. Translocation of the blood from the periphery via circulatory reflexes including recovery of vasoconstrictor tone at onset of orthostasis would be reflected by increased calculated TPR. It is apparent that the current study demonstrates a suppression of vascular resistance, vasodepressor reflex, during increased gravitational stress. Nevertheless, alternative central sympathetic reflexes are adequate for the maintenance of BP and orthostatic tolerance throughout the study.
The clinical implications for exercise-induced orthostatic intolerance may include accurate diagnosis, notably to differentiate from syncope which occurs during exercise. Analysis of physiological responses of individuals who experience presyncope and/or syncope despite presenting without a history of syncope can determine those susceptible to instances in situational circumstances (prolonged standing in queues). All 10 athletes remained orthostatically tolerant to the standing challenge postrace despite trends suggesting greater reductions in SBP (p = 0.06). The Δ−15 (20) mm Hg reduction in SBP as a result of the 3 minute stand would appear to be inadequate to facilitate the development of presyncope amongst the athletes, with the exception of one athlete who reported blurred vision and nausea (SBP Δ−30 mm Hg, HR Δ18 beats/min, SV Δ−41 ml (−53%)). Individuals who develop such symptoms, but do not progress to syncope, can be classified to have an “orthostatic weakness”.17 Susceptibility to the onset of presyncope and syncope has previously been proposed to be related to the development of postural hypotension18; however, asymptomatic postural hypotension postexercise has previously been reported.19
What is already known about this topic
▶. Circulatory responses (HR and/or TPR) to orthostasis are responsible for the defence of sufficient blood pressure, and therefore orthostatic tolerance.
▶. The literature suggests that postexercise (intermittent and high-intensity) hypotension can occur amongst normotensive individuals; however, its effect in combination with gravitational stress following a bout of prolonged exercise is unknown.
What this study adds
▶. Increased HR allows for the maintenance of supine SBP postexercise in the face of decreased TPR.
▶. Alterations in SBP, HR and CO were significantly greater postexercise, although all individuals remained orthostatically tolerant. A longer standing period might have induced postural orthostatic hypotension (Δ SBP<20 mm Hg) and the potential onset of postexercise orthostatic intolerance.
One limitation to the generalisation of the current results was that the study recruited runners with no history of exercise-associated presyncope or syncope. Evaluation of this population would have important clinical implications and should be the focus of future research. The period of the standing challenge (3 min) may not have been sufficient to induce reductions in SV. This response is thought to be associated with pre-exercise and/or postexercise orthostatic alterations in individuals with recurrent presyncope and a history of syncope postexercise, although this is not seen in the current study. If the orthostatic period is prolonged, the potentially continuous reduction in SV, in combination with reduced vasoconstrictor responsiveness, may exacerbate the pooling effect, which may in principle lead to presyncopal symptoms. However, for the purpose of the present study a 3 min period was selected to ensure that each athlete was assessed without delay upon presentation to the testing area.
Furthermore, the indirect measurement of BP at a peripheral assessment location, and the estimation of consequential haemodynamic variables, may not be as accurate as invasive measurement, but these measures have been shown to provide a reliable index of change during interventions.10,–,13 Methods such as echocardiography are preferable to ensure more accurate measurement of SV and subsequent CO. However, in this field situation, the PortAPres was more appropriate for the assessment of athletes and recorded stable BP responses during the supine and orthostatic periods.
Conclusions
In the current cohort, following prolonged exercise, the imposition of an orthostatic challenge results in a reduction in SV, CO and SBP despite a rise in HR. Despite a reduction in SBP, presyncopal symptoms were only experienced by one runner, and thus the orthostatic challenge was relatively well tolerated.
References
Footnotes
-
Funding Olympic Medical Institute, Northwick Park Hospital, Watford, Road Harrow, HA1 3UJ; Centre for Sports Cardiology, Northwick Park Hospital, Watford Road, Harrow, HA1 3UJ.
-
Competing interests None.