Article Text

Abstract
Objective To summarise the best available evidence to determine the impact of helmet use on head injuries, neck injuries and cervical spine injuries in skiers and snowboarders.
Data sources Relevant publications were identified through electronic searches of MEDLINE, PubMed, EMBASE, CINAHL and the Cochrane Library databases (1966–2009) in addition to manual reference checks of all included articles.
Review methods 45 articles were identified through our systematic literature search. Of these, 10 studies met the inclusion criteria after two levels of screening. Two independent reviewers critically appraised the studies. Data were extracted on the primary outcomes of interest: head injury, neck injury and cervical spine injury. Studies were assessed for quality by the criteria of Downs and Black.
Results Studies reviewed indicate that helmet wear reduces the risk of head injuries in skiing and snowboarding. Four case-control studies reported a reduction in the risk of head injury with helmet use ranging from 15% to 60%. Another cohort study found a significantly lower incidence of head injuries involving loss of consciousness in helmet users (p<0.05). The five remaining studies suggested a major protective effect of helmets by indicating that none or few of the head-injured and deceased participants wore a helmet.
Conclusions There is strong evidence to support the protective value of helmets in reducing the risk of head injuries in skiing and snowboarding. There is no good evidence to support the claim that the use of helmets leads to an increase risk of cervical spine injuries or neck injuries.
Statistics from Altmetric.com
Introduction
Alpine skiing and snowboarding are among two of the most popular winter sports in the world. Of the 600 000 ski and snowboarding-related injuries each year in North America, an estimated 15–20% are head injuries.1 Head injury is indicated as the most frequent reason for admission and constitutes 20–54% of hospital admissions for injury from skiing and snowboarding.2 Levy et al3 reported that among skiers and snowboarders of all ages admitted to hospital for head injuries, skier–tree collision was the most common mechanism for head injuries. The prevalence of these head injuries is especially worrisome for children younger than 18 years of age. Downhill skiing injury fatalities in children comprised 14% of all skiing fatalities from ski resorts in Colorado, and traumatic brain injuries were the primary cause of 67% of total fatalities.4 In another study, children were found to have twice the incidence of injury to the head, face and neck as other age groups, and 22% of head injuries were serious enough to cause loss of consciousness or clinical signs of concussion.5 Helmets have been proposed as an injury-prevention strategy, yet their protective value remains the subject of intense debate.
Following the well-publicised death of actor, Natasha Richardson, who died from an epidural haematoma at the Mont Tremblant ski resort in Quebec in March 2009,6 the debate over the use of helmets to prevent fatalities related to ski and snowboarding head injuries has been revitalised. Though multiple media reports claim that Ms Richardson might have survived had she received immediate treatment instead of allowing 4 h to be elapsed between her injurious fall and hospital admission,7 just as many British and international media stories have addressed the possibility that helmet use could have reduced the blunt impact.6,–,8
The US Consumer Product Safety Commission projected that 44% of head injuries could be prevented by the use of helmets in skiing and snowboarding, and that the use of helmets for children aged 15 and under could reduce head injuries in this group by 53%.9 Despite the burden of these injuries and the potential for the prevention of such injuries with the use of helmets,10 helmet wear remains particularly low. In a study conducted at multiple US ski resorts, helmets were worn by only 12.1% of the skiing population.11 Since Ms Richardson's death, Intrawest, the company that operates the facility, has announced that it will strongly recommend helmet wear at all its nine North American resorts.12 Furthermore, helmets will be mandatory for children and teens enrolled in ski and snowboard programmes and for any student, regardless of age, participating in freestyle terrain park programmes.12 These new and unprecedented helmet guidelines are expected to have a ripple effect at resorts around the world.
We are aware of only one other literature review that has been carried out in this area. Benson et al13 conducted a systematic review of the literature to address whether protective equipment is useful in preventing concussion. They aimed to evaluate the efficacy of protective equipment such as mouthguards, face shields and helmets/headgear in reducing concussion risk across a variety of sports including football, rugby, hockey, bicycling, soccer, skiing and snowboarding. The breadth of this review did not allow for a detailed review of studies reporting on the specific protective value of helmets in skiing and snowboarding activities. Furthermore, their review was restricted to examining just one outcome, concussions, thereby neglecting the spectrum of other potential head injuries that may be sustained from skiing and snowboarding as well as additional adverse events such as cervical spine injuries and neck injuries.
The main objectives of this study were to systematically review the effectiveness of helmet wear in reducing the risk of head injuries for skiers and snowboarders, and to summarise the potential adverse events, namely cervical spine injury and neck injury, which are associated with helmet wear. Due to the heterogeneity in the design of the included studies, they have been reviewed systematically using a narrative approach.
Materials and methods
A comprehensive search of the English-language literature was performed incorporating both electronic and manual components. The electronic search was performed using MEDLINE (1966 to November 2009); PubMed (1948 to November 2009); EMBASE (1980 to November 2009); CINAHL (1982 to November 2009) and the Cochrane library databases. Keywords searched were ‘head injury,’ ‘brain injury,’ ‘concussion,’ ‘traumatic brain injury,’ ‘head trauma,’ ‘neck injury,’ ‘cervical spine injury,’ ‘helmets,’ ‘helmet wear,’ ‘skiing,’ ‘skiers,’ ‘snowboarding,’ ‘snowboarders,’ ‘winter sports.’
Study selection was accomplished through two levels of study screening. At level 1 screening, abstracts were reviewed for the following exclusion criteria: publication of abstracts only, case reports, letters, comments and reviews; languages other than English; and no reporting of the helmet intervention for skiers and/or snowboarders. Full articles were then obtained for all studies accepted at level 1 and for any citations for which a determination could not be made from the abstract. For level 2 screening, inclusion required that the studies dealt with at least one of the outcomes: head injury, neck injury or cervical spine injury.
Studies that were admissible to the systematic review were ones that passed both levels of screening. Data were extracted by two reviewers, and all disagreements were resolved by consensus. Table 1 presents the definitions of key terms used in this review.
Definitions
Quality assessment
Methodological quality was assessed using the Downs and Black checklist.14 The five main areas assessed were: reporting, external validity, bias (internal quality), confounding (internal validity) and power. The performance of the included studies in each of these areas is summarised in online supplemental table 1 and discussed below.
Reporting
Reporting was adequate for all the included studies. This included reporting of the study hypothesis, the main outcomes and interventions, participant characteristics, estimates of random variability and main findings. Five studies reported on potential adverse events that may be associated with helmet wear (cervical spine injury and neck injury). None of the studies reported on characteristics of study participants lost to follow-up or the cost-effectiveness of the interventions. Apart from these concerns, the studies were carried out with otherwise appropriate reporting.
External validity
For all 10 included studies, participants were representative of the entire population from which they were recruited. Additionally, the staff, places and facilities where the patients were treated were representative of the treatment that the majority of patients received in all studies.
Internal validity
As the study population and the study investigators could not be blinded with respect to the intervention, concern for internal validity bias is present. However, the absence of concealment was due to the nature of the intervention itself, and the studies were carried out with otherwise sound methods (appropriate statistical tests, reliable compliance with intervention measures, valid outcome measures).
Results
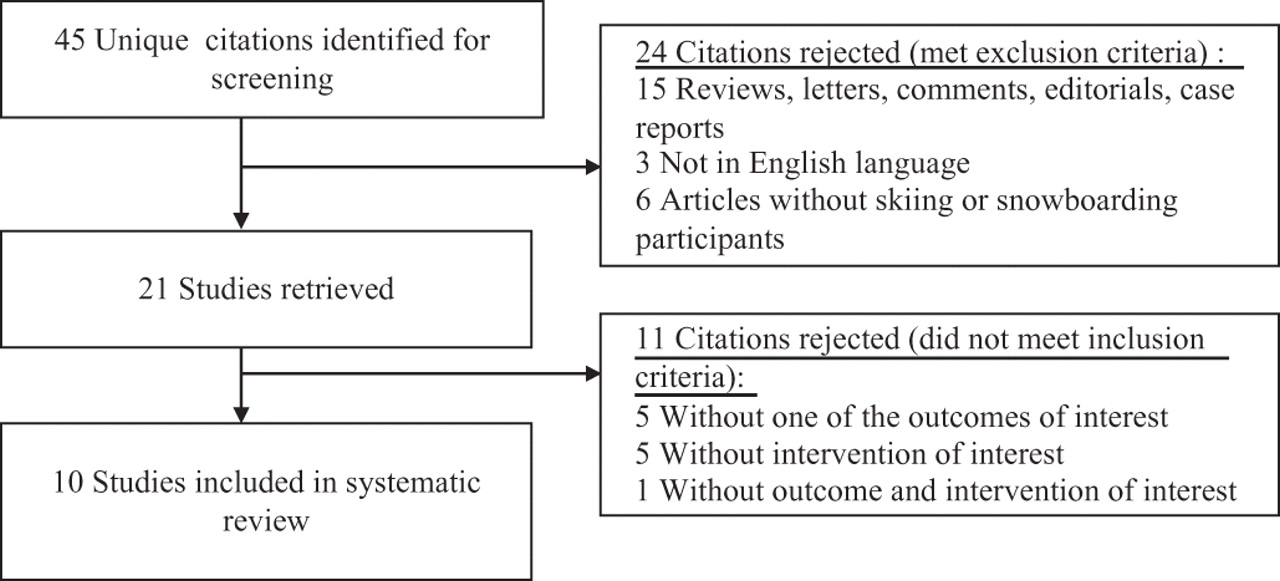
A flow diagram outlining the systematic review process is provided (figure 1). The initial literature review identified 45 citations for screening. Of these, 24 were rejected after reviewing their abstracts. Of the remaining 21 articles, 11 did not meet the inclusion criteria. Therefore, 10 fully extracted studies were available for the systematic analysis.

{kind=link}
Study attrition diagram.
The characteristics of the included studies are presented in table 2. Six of the studies were based in North America, three in Europe and one in Japan. Included were four case–control studies, two retrospective cohort studies and three uncontrolled case series investigations, and one other study was cross-sectional in design. One study examined all three primary outcomes of interest.2 Four studies reported on both head injuries and neck injuries.1 2 15 16 Table 2 provides a summary of the following demographic and methodological components in each of the included studies: sport, study design, duration (seasons), eligibility/study population, exposure measures, outcome measures and the main results.
Characteristics of included studies
Head injury
All four case–control studies reported a reduction in the risk of head injury with helmet use ranging from 15% to 60%.1 2 15 16 The case–control studies incorporated a concurrent comparison group and all performed appropriate statistical analyses. Cases were recruited from the same populations as the intervention groups and over the same period of time. Data were available as measures of comparison between cases and controls in the risk of sustaining head injuries from helmet use and non-use respectively.
Mueller et al1, Hagel et al15 and Sulheim et al16 used individuals with other injury types as controls. These three studies also used matching techniques and controlled for potential confounders and effect modifiers. Macnab et al2 compared a simple count of the proportion of helmet users in this group with random skiers and snowboarders at the same resort. Of note is the study done by Sulheim et al,16 which examined the relationship using a second set of a non-injured, representative control group to correct for potential confounders. In doing so, the study investigators addressed the more general question as to whether helmets were protective for all skiers and snowboarders, irrespective of whether they experienced other injuries.
In a retrospective cohort study, Greve et al17 reported that helmets were especially protective in collisions with fixed objects. Fukuda et al18 conducted a case series which did not find any significant association between helmet wearing and the occurrence of head injuries requiring medical attention. Machold et al19 suggested a major protective effect of helmets by indicating that none of the helmeted participants sustained a head injury. Similarly, Sacco et al20 and Ekeland and Rødven21 suggested a protective effect of helmets by indicating that none or few of the head-injured and deceased patients wore a helmet.
Cervical spine injury and neck injury
Macnab et al2 reported no increased risk of cervical spine injury with helmet wear in children under the age of 13. With respect to neck injury, Hagel et al,15 using a population of skiers and snowboarders with other injuries as their control group, could not rule out the possibility of an increased risk of neck injury with helmet use, but the estimates on which this assumption is based are imprecise. Bridges et al22 studied a young group of children in their Mt Tremblant study and found that when adjusted for age (<6, 6–12, >12), there was no increase in neck injury due to helmet use. Additionally, Sulheim et al16 found that helmet use did not increase the risk of neck injury in alpine skiing and snowboarding populations. Similarly, Mueller et al1 found no evidence that helmet use increases the occurrence of neck injuries.
Discussion
Our systematic review found that helmet wear is associated with a significant decrease in the risk of head injuries for skiers and snowboarders. It is thought that helmets may increase the risk of spinal injury owing to the biomechanics of the association between the helmet and the head and neck,13 a particular concern for children, who have a greater head-to-body ratio. However, our systematic review found no conclusive evidence to support the claim that helmet use is associated with a heightened risk of neck or cervical spine injury.
The Ohio Commission on the Prevention of Injury and the Ohio Post-Critical Trauma Care Commission have released findings reporting that for every dollar spent on a bicycle helmet, $30 is saved in direct medical care costs and other costs to society.23 Although cost-effectiveness needs to be further explored in skiing helmets, given the current evidence, we recommend the use of helmets by all skiing and snowboarding participants along with the promotion and enforcement of appropriate standards for ski and snowboarding helmets.
Also relevant to this discussion is the theory of compensating behaviour or risk compensation that has been advanced by some researchers to suggest that if a person perceives an intervention (eg, ski helmet use) to have lowered their level of risk, they will change their behaviour back to their desired risk level (eg, ski faster or more aggressively).18 However, in a recent matched case–control study by Hagel et al,24 the authors found that there is no evidence to support the contention that helmet use increases the risk of severe injury or high-energy crash circumstances. The results show that helmet use in skiing and snowboarding is not associated with riskier activities that lead to injuries to other regions of the body.
Limitations
Some limitations of our review also merit discussion. The most important is that we were unable to identify any randomised controlled trials (RCTs). It is unlikely that RCTs will ever be undertaken to study this question; thus the strongest feasible design for addressing our question is case–control. A report of the evidence supporting educational and other interventions to prevent injury in skiing and snowboarding was beyond the scope of this review.
Future directions
Although we have presented the strongest data to date on this issue, there is still room for better research. Skiing and snowboarding are universal sports, but the included studies arose from a limited number of high-income nations in the Northern Hemisphere. If any global impact is to be made on this pressing problem, further research and action are required from an international community. There is also a need for analysing the risk of sustaining a head injury in each snowboarder and skier according to other potential risk factors such as the actual time spent on the skis or snowboard, the type of equipment used, the individual experience and the slope conditions presenting at the time. Future research should also address the reasons for helmet use or non-use (such as personality or parental influence in the case of adolescent participants). Role modelling can have powerful effects. Research in helmet use in cyclists shows that one of the major predictors of reliable and sustained helmet use in children is whether the parents of these children wear helmets themselves.25
Additionally, helmets are only one aspect of a multifaceted approach to preventing head injuries. Future research needs to explore the value of other approaches such as educational and policy interventions to prevent such injuries. More high-quality studies that report on all three outcome measures, particularly for adolescent populations where the prevalence of head injuries attributable to these winter sports is known to be higher, are required.
Conclusions
Our systematic review confirms that helmets are protective and do not lead to a heightened risk of neck or cervical spine injury. The international debate on helmet use in winter sports is at a crucial juncture, with many individuals suggesting that participants would benefit from a reduced risk of head injuries with more stringent recommendation guidelines on helmet wear. Head injuries can have fatal or devastating long-term sequelae.
Policy-makers, the stakeholders who seek to influence them and the public whose health will be affected by their decisions should take this research evidence into account.
What is already known on this topic
Skiing and snowboarding are fast, high-impact sports with a high propensity for head injuries.
What this study adds
▶. Helmet wear reduces the number and risk of overall head injuries in skiing and snowboarding.
▶. Helmet use does not appear to be associated with an increased risk of neck injuries and cervical spine injuries for skiers and snowboarders.
References
Footnotes
-
Competing interests The authors have no financial conflict of interests. MDC holds a volunteer position without remuneration as Vice President of ThinkFirst Canada.
-
Provenance and peer review Not commissioned; externally peer reviewed.