Article Text

Abstract
The purpose of the present study was to compare the effects of cold water immersion (CWI) and active recovery (ACT) on resting limb blood flow, rectal temperature and repeated cycling performance in the heat. Ten subjects completed two testing sessions separated by 1 week; each trial consisted of an initial all-out 35-min exercise bout, one of two 15-min recovery interventions (randomised: CWI or ACT), followed by a 40-min passive recovery period before repeating the 35-min exercise bout. Performance was measured as the change in total work completed during the exercise bouts. Resting limb blood flow, heart rate, rectal temperature and blood lactate were recorded throughout the testing sessions. There was a significant decline in performance after ACT (mean (SD) −1.81% (1.05%)) compared with CWI where performance remained unchanged (0.10% (0.71%)). Rectal temperature was reduced after CWI (36.8°C (1.0°C)) compared with ACT (38.3°C (0.4°C)), as was blood flow to the arms (CWI 3.64 (1.47) ml/100 ml/min; ACT 16.85 (3.57) ml/100 ml/min) and legs (CW 4.83 (2.49) ml/100 ml/min; ACT 4.83 (2.49) ml/100 ml/min). Leg blood flow at the end of the second exercise bout was not different between the active (15.25 (4.33) ml/100 ml/min) and cold trials (14.99 (4.96) ml/100 ml/min), whereas rectal temperature (CWI 38.1°C (0.3°C); ACT 38.8°C (0.2°C)) and arm blood flow (CWI 20.55 (3.78) ml/100 ml/min; ACT 23.83 (5.32) ml/100 ml/min) remained depressed until the end of the cold trial. These findings indicate that CWI is an effective intervention for maintaining repeat cycling performance in the heat and this performance benefit is associated with alterations in core temperature and limb blood flow.
Statistics from Altmetric.com
Cold water immersion (CWI) has become a popular postexercise recovery intervention used by athletes in various sports and events, and there is a growing body of evidence to support its use. Compared to control interventions or traditional recovery techniques such as active recovery (ACT), CWI provides significant gains in performance during successive bouts of exercise, particularly in the heat.1,–,6 However, despite these promising findings, others have found negligible changes when investigating the recovery effects of CWI.7,–,9
These inconsistent findings are difficult to explain as the specific mechanisms associated with the performance effects of CWI recovery remain to be elucidated. An increase in hydrostatic pressure and/or a reduction in temperature may contribute the beneficial effect of CWI.10 However, it has been demonstrated that the performance recovery associated with CWI is significantly greater than that achieved with warm (38°C) water immersion.5 This indicates that the performance benefit of CWI is more likely to be the result of a cold effect than a water immersion effect per se. Reductions in core and tissue temperatures,11,–,14 acute inflammation15 and perceived pain1 16 are well-established effects of cold therapy. Although these local effects of cold exposure may contribute to the performance recovery effect, it is unlikely given that muscle strength and power output are impaired immediately after muscle cooling.17,–,19
Cardiovascular responses to body cooling include increases in peripheral vascular resistance, blood pressure and stroke volume, and reductions in heart rate, cardiac output and peripheral blood flow.10 20 21 It has been suggested that the apparent redistribution of blood from the periphery to the core leads to an increase in central blood volume and venous return and thereby improves cardiac efficiency, blood delivery to the working muscles and performance during subsequent exercise.22 In a previous study, heart rate was lower after CWI compared to ACT throughout a 40-min period of rest.4 However, whether CWI recovery has an influence on postexercise limb blood flow is not known.
Therefore, the purpose of the present study was to compare the effects of CWI recovery and ACT on repeated cycling performance, blood flow to the arms and legs and core body temperature, in hot laboratory conditions.
Methods
Subjects
Ten endurance-trained male cyclists (mean (SD); age 33.7 (4.7) years; body mass 78.6 (7.3) kg; height 180.1 (5.2) cm and VO2peak 66.7 (6.1) ml/kg/min) volunteered to participate in the present study. Before participation, all subjects were informed of the potential risks and requirements of the study and provided informed written consent. Subjects were required to refrain from alcohol (48 h), caffeine (24 h) and strenuous exercise (24 h) before testing. The study was approved by the human research ethics committees of the Australian Institute of Sport and the University of the Sunshine Coast.
Experimental design
Before participation, all subjects completed a maximal cycling test on a Lode ergometer (Lode, Groningen, The Netherlands), which commenced at 125 W and increased by 25 W every 3 min until exhaustion. From this, each individual's peak power output (PPO; W) and VO2peak were determined. In addition, two familiarisation sessions replicating the testing protocols and procedures were completed to minimise any potential learning effect throughout the study.
Two experimental testing sessions were completed, separated by 7 days. Each testing session commenced with the subject lying supine for 10 min, during which baseline measures of heart rate, limb blood flow, blood lactate and core temperature were obtained. Subjects then completed two 35-min exercise bouts (Ex1 and Ex2) that were separated by a 60-min recovery period. The two exercise bouts included a 5-min warm-up (1 min at 125 W, 150 W, 175 W, 200 W and 75% individual PPO), followed by a 30-min exercise bout consisting of 15 min at a fixed workload (75% individual PPO) and a 15-min performance trial. During the performance-trial component, subjects were required to complete as much work as possible in the 15-min period. Subjects had access to the test time; however, no other feedback or encouragement was provided throughout the testing session. In a randomised crossover design, subjects performed one of two recovery interventions between the two 35-min exercise bouts: ACT or CWI recovery. All testing and recovery sessions were completed in a temperature-controlled laboratory (temperature 32.8°C (1.1°C); relative humidity 43.6% (1.8%)). Subjects were required to complete a food diary for 24 h before testing to ensure food intake was consistent. In addition, a standardised meal (2 g/kgbw carbohydrate) was provided and consumed 2 h before testing. A standardised fluid carbohydrate beverage (Gatorade, 6% carbohydrate content) was consumed throughout the testing session (4 ml/kgbw during the first 15 min of the two 35-min exercise bouts and 10 ml/kgbw between exercise bouts).
Recovery interventions
Five minutes after the completion of the first exercise bout (Ex1), subjects performed either a standardised ACT protocol (cycling at 40% individual PPO) for 15 min or a full body (excluding head and neck) CWI recovery whereby subjects were vertically immersed in 15°C water for 15 min. Immediately after the recovery intervention, subjects rested in a supine position for a further 40-min period of passive recovery.
Outcome measures
Performance
The effectiveness of each recovery intervention was determined by comparing total work (kJ) performed during the 15-min performance-trial component of each exercise bout.
Rectal temperature
Core temperature, measured as rectal temperature, was monitored through the use of a disposable rectal probe (Mon-a-therm; Mallinckrodt Medical, St. Louis, Missouri, USA) inserted 12 cm beyond the anal sphincter before testing. Rectal temperature was recorded (Zentemp 5000; Zencor, Victoria, Australia) at baseline and every 5 min throughout the testing sessions.
Limb blood flow
Blood flow to the right leg and right forearm was measured using venous occlusion plethysmography. Subjects lay in a supine position with their arms and legs raised on foam blocks, to be above the level of the heart. Rapid inflation pressure cuffs were placed around the thigh and upper arm. To detect the changes in limb volume, mercury-in-silastic strain gauges were placed around the maximal girth of the calf and forearm, and connected to a plethysmograph (EC-6; Hokansen, Bellevue, Washington, USA). Plethysmograph signals, as well as single-lead electrocardiograph signals, were continually captured and stored digitally at 1 KHz (Powerlab; ADInstruments, New South Wales, Australia). Blood flow was assessed by inflating the thigh or arm pressure cuff to a venous occluding pressure of 65 mm Hg for a 10-s period and measuring the rate of rise in limb volume over the period of two cardiac cycles. On each occasion, blood flow was measured in triplicate at the leg and then in triplicate at the arm, with 10-s separating each measurement. The within-subject coefficient of variation of all triplicate measures was 9.5% (7.2%). Triplicate measures were then averaged to provide a single measure of leg blood flow and arm blood flow at each time point. Limb blood flows were measured at baseline, 3 min after each of the exercise bouts and at regular intervals throughout the 40-min passive recovery period (ie, minutes 3, 7, 11, 15, 19, 23 and 27). The leg-to-arm blood flow ratio ((leg blood flow/arm blood flow) × 100) was calculated to differentiate the local effects of exercise from the effects of temperature on leg blood flow.
Lactate
Blood lactate concentration was measured using an earlobe sample and analysed using a portable analyser (Lactate-Pro, KDK Corporation, Shiga, Japan). Blood lactate concentration was recorded at baseline, throughout the exercise bouts (end warm-up, end fixed-intensity component, end performance-trial component) and after the 15-min recovery period (ACT or CWI).
Heart rate
Heart rate was monitored using a Polar heart rate monitor (Polar Electro Oy, Kempele, Finland) fitted to the subject before testing. Heart rate was recorded at baseline and every 5 min throughout the testing sessions.
Statistical analysis
The effect of recovery intervention on the recovery of cycling performance was assessed using a paired t test. Two-way repeated measures analysis of variance was performed on all other data to test for the effects of recovery intervention (ACT, CWI), time throughout the test and interactions between these factors. Where there was a significant main effect or interaction, differences were located using Tukey's test or, for data that were not normally distributed, a Wilcoxon's signed rank test. The strength of association between variables was assessed using Pearson's correlation coefficient. Significance was set at p<0.05 and data are expressed as mean (SD).
Results
Performance
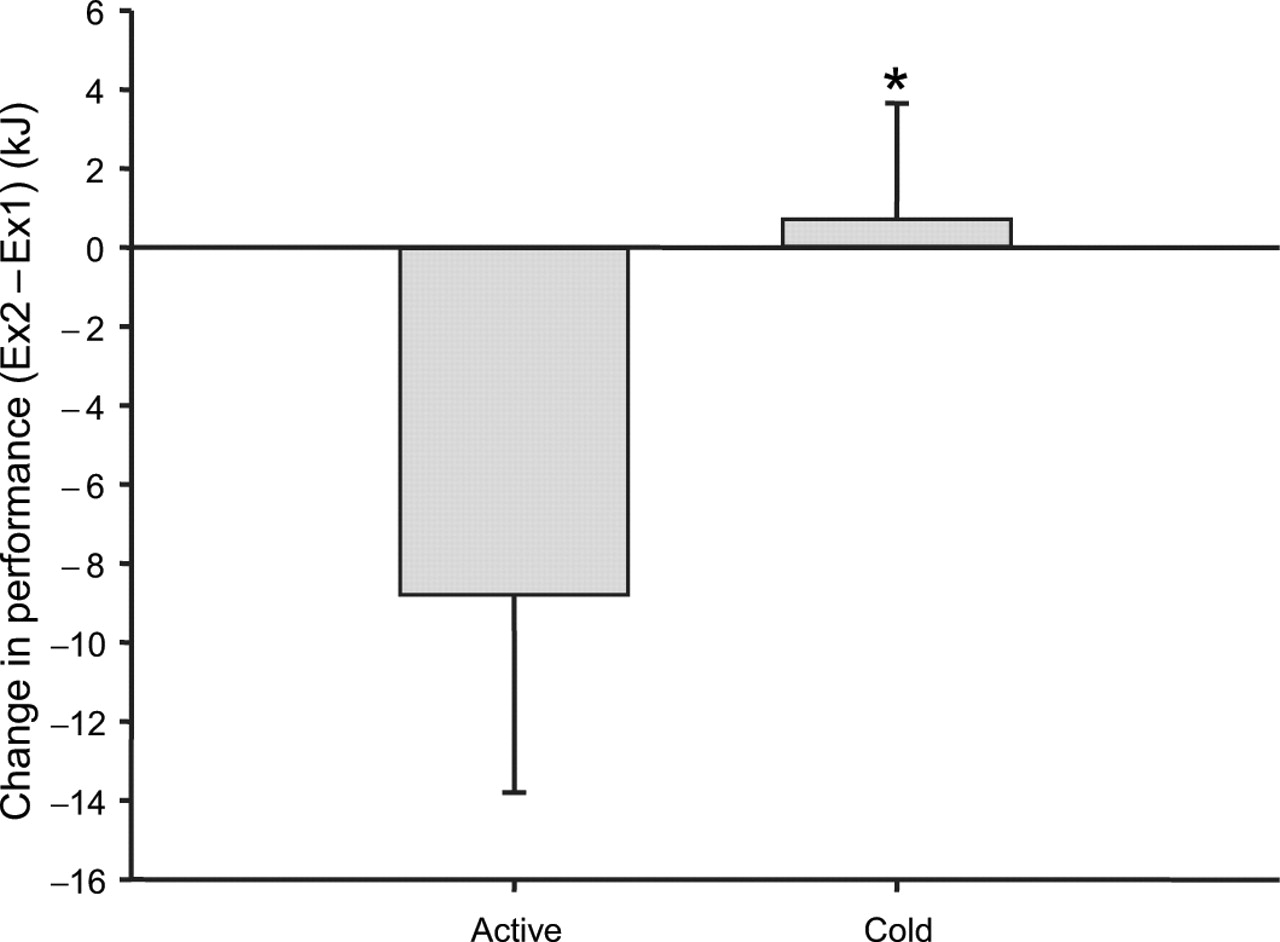
There was a significant decline in performance-trial performance from Ex1 to Ex2 using ACT recovery (−1.8% (1.1%)) compared to the change seen with CWI recovery (+0.10% (0.7%)) (fig 1).
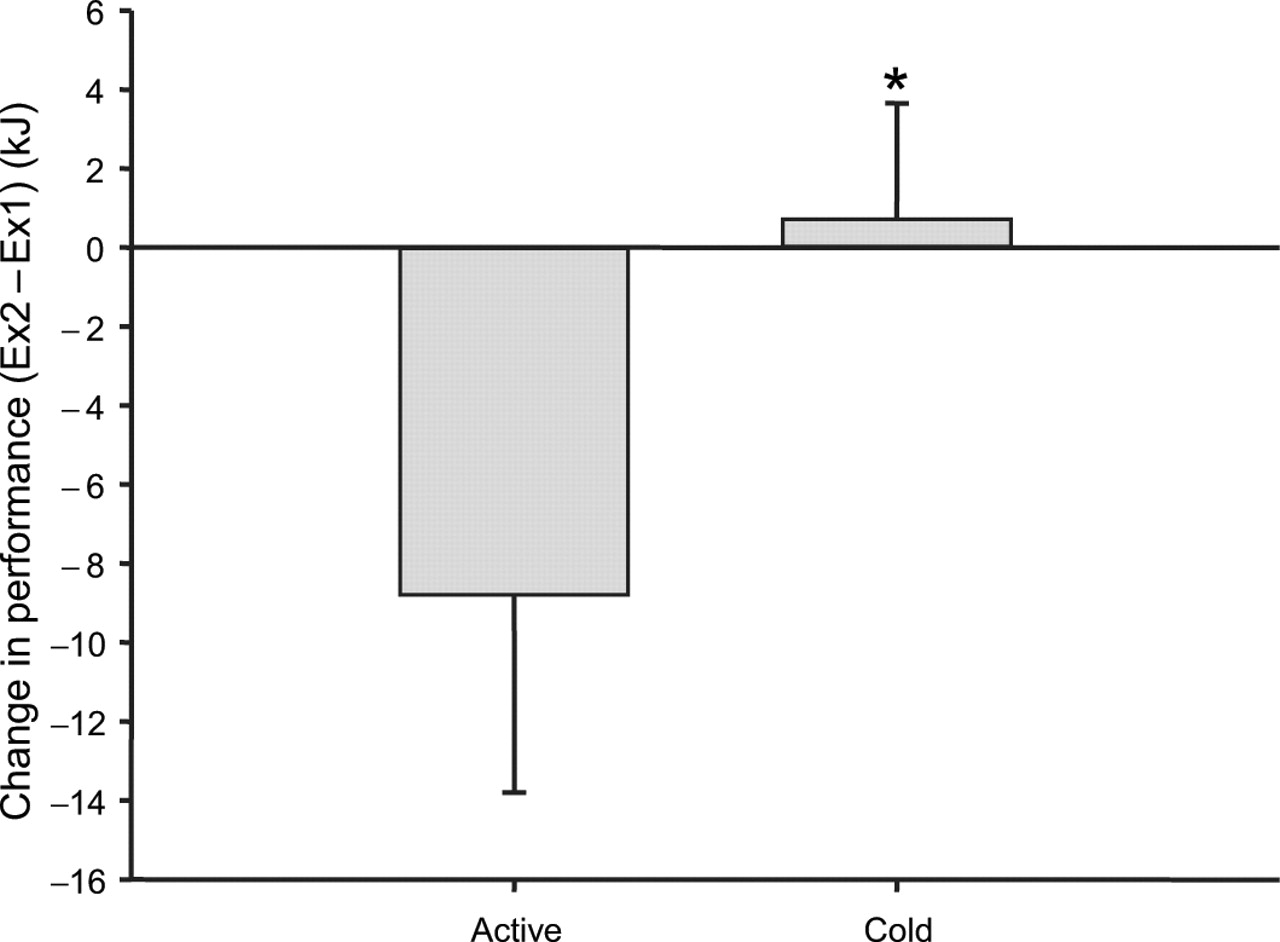
Difference in work done between first (Ex1) and second (Ex2) cycle performance trials. Each trial was separated by a period of either active recovery or cold water immersion recovery. Values are means (SD). *Significant difference between recovery interventions (p<0.05).
Rectal temperature
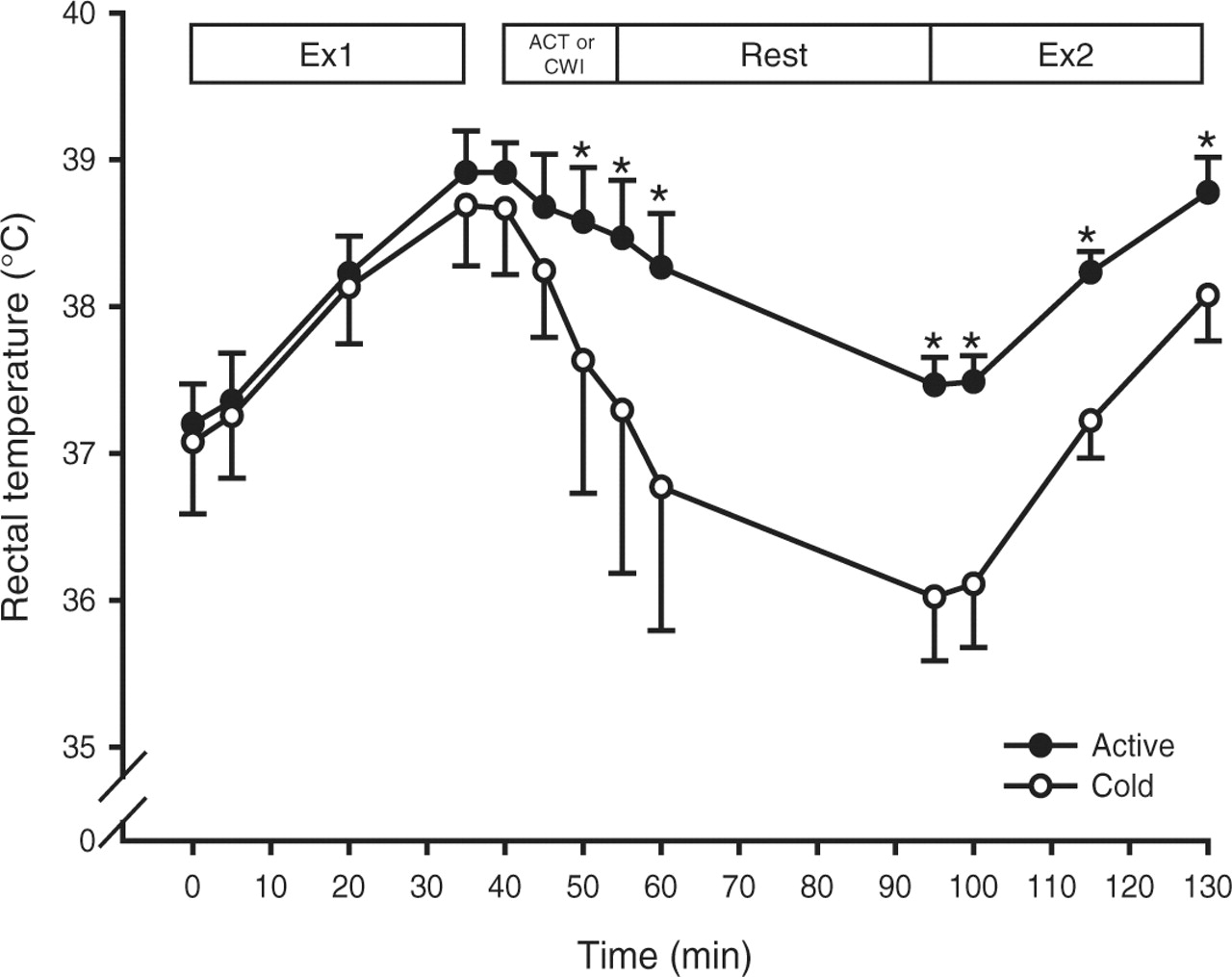
There were no differences in rectal temperature between interventions at baseline or at the end of Ex1 (fig 2). However, rectal temperature was significantly reduced immediately after CWI, at the end of the 40-min passive recovery period and upon completion of Ex2.

Rectal temperature during the first cycling performance trial (Ex1), a 15-min period of either active recovery (ACT) or cold water immersion recovery (CWI) followed by a 40-min rest period, and the second cycle performance trial (Ex2). Values are mean (SD). *Significant difference between recovery interventions (p<0.05).
Limb blood flow
As shown in fig 3, there were no differences in leg or arm blood flows between interventions at baseline or at the end of Ex1. After CWI, there was a dramatic reduction in limb blood flow to sub-baseline levels. Limb blood flow also decreased with ACT, although it did not return to baseline levels. Blood flow to the arms and legs was significantly lower in CWI compared with ACT throughout the passive recovery phase until the onset of Ex2. After Ex2, leg blood flow was not different between CWI and ACT, whereas arm blood flow remained significantly lower in CWI until the end of the testing session.

{kind=link}
{kind=link}
{kind=link}
(A) Leg blood flow, (B) arm blood flow and (C) the leg-to-arm blood flow ratio during the first cycling performance-trial (Ex1), a 15-min period of either active recovery (ACT) or cold water immersion recovery (CWI) followed by a 40-min rest period, and the second cycle performance trial (Ex2). Values are mean (SD). *Significant difference between recovery interventions (p<0.05).
The leg-to-arm blood flow ratio was not different between interventions at baseline or immediately after Ex1, and it remained unchanged throughout the ACT trial (fig 3C). After the CWI intervention, the ratio increased and was significantly higher than that for ACT throughout the passive recovery period. By the end of Ex2, the blood flow ratio in the CWI trial had returned to baseline levels and was not different to the blood flow ratio in the ACT trial.
The difference in the leg-to-arm-blood flow ratio between the passive phases of the ACT and CWI trials was significantly correlated with the difference in core temperature between the trials (r=0.58, p<0.05). Furthermore, there was a significant negative correlation between the gain in performance from the ACT to the CWI trial, and the corresponding reduction in both core temperature (r=−0.70, p<0.05) and the leg-to-arm-blood flow ratio (r=−0.73, p<0.05).
Heart rate
No significant differences were observed in heart rate between trials until the onset of the recovery period after Ex1. Heart rate fell during CWI and remained significantly lower compared with ACT throughout the entire 40-min recovery period. Immediately before Ex2, heart rate was lower in the CWI trial (ACT 90 (11) bpm; CWI 78 (15) bpm, p<0.05). Heart rate tended to remain lower after CWI until the performance-trial phase of Ex2, although this difference between trials was only significant during the first 5 min of the exercise bout.
Blood lactate
Lactate concentrations were very similar between trials, with the only significant difference (p<0.05) observed immediately after the recovery interventions where blood lactate in the CWI trial was 4.5 (1.2) mM compared to 2.3 (0.8) mM in the ACT trial.
Discussion
This study aimed to compare the effects of ACT with CWI recovery on rectal temperature, limb blood flow and repeated cycling performance in hot laboratory conditions. CWI recovery has been shown to benefit repeated cycling and running performance in normal and hot environmental conditions.3 6 Repeated cycle performance across consecutive days in normal laboratory conditions is better maintained when CWI recovery is used compared with warm water recovery and passive recovery.5 In the present study, CWI lead to significant reductions in rectal temperature, leg blood flow, arm blood flow and heart rate compared with ACT. Using CWI recovery, there was no change in cycling performance from the first to second exercise bout, whereas there was a significant reduction (−1.8%) in cycle performance when ACT recovery was completed. This reaffirms the performance benefit of CWI recovery, which has become a popular recovery intervention for many elite athletes.
Little or no performance benefit is gained when CWI is used as a recovery intervention between bouts of local muscle exercise. After bouts of eccentric leg extension exercise8 and eccentric elbow flexion,7 CWI of the exercising limbs offered no benefit in the recovery of muscle performance or the level of muscular pain compared with control. Moreover, CWI of the lower limbs was shown to have a negative effect on repeated 30-s sprint performance compared with passive recovery.23 24 Collectively, these findings suggest that the performance benefit of CWI relies on a full-body cooling protocol, and the benefit is generally limited to high-intensity large-muscle-mass exercise, such as cycling or running, that is maintained for a duration of 15 min or longer.
Whole-body precooling before exercise is associated with improved performance.25 26 It is suggested that precooling before exercise improves performance by extending the time taken (or work done) before a critical limiting temperature is reached.27 A large reduction (0.5–3.5°C) in rectal temperature occurred after CWI that remained throughout the trial. The reduction in temperature in the CWI trial persisted until the end of Ex2, which lends some support to the notion that CWI increases the heat storage capacity of the body and thereby allows for greater work to be performed during repeated exercise bouts in hot conditions.28 An unexpected finding was the negative correlation between the change in rectal temperature and the change in performance between trials, whereby the greatest reduction in rectal temperature was associated with the smallest change in performance. This raises the possibility that there is an optimal cooling threshold, below which there is no further performance benefit, or even a performance decrement. Future research should test the effect of the magnitude of temperature changes on performance recovery with a view to establishing individualised cooling strategies that might take into account the subject's mass, body composition and body surface area.
A key aim of the present study was to examine the effect of CWI and ACT recovery on limb blood flow. Arm and leg blood flows were measured in an attempt to differentiate the local effects of exercise, which would be greatest in the legs, from the effects of temperature, which would have a similar influence on blood flow in the arms and legs.29 30 Indeed, resting blood flow was initially elevated in both the arms and legs above normal resting levels (fig 3). This reflects the influence of the hot ambient conditions on skin temperature, which leads to increased cutaneous blood flow and therefore increased limb blood flow.
Peiffer et al31 recently reported that CWI recovery after a cycling time trial in hot laboratory conditions lead to a reduction in femoral venous diameter, which was interpreted as a vasoconstrictive response. In the present study, limb blood flow during the passive recovery phase was lower after CWI than ACT. The magnitude of the flow reduction during CWI was greater in the arms than in the legs, as reflected by the increase in the leg-to-arm blood flow ratio during the passive recovery period. This increase in the leg-to-arm blood flow ratio during CWI compared with ACT was correlated with the difference in rectal temperature between the two trials, where a large increase in the blood flow ratio was associated with a large reduction in rectal temperature from the ACT to CWI trial. Furthermore, the larger the change in the leg-to-arm blood flow ratio from the ACT to CWI trial, the smaller the performance gain. Venous occlusion plethysmography allows for total blood flow into a limb to be measured. Therefore, although it is not possible to differentiate between skin and muscle blood flow in the present study, the elevated leg-to-arm blood flow ratio during CWI is likely to reflect an altered distribution of blood flow. Hence, while absolute leg blood flow was reduced during CWI, it is likely that there was a relative reduction in skin blood flow, and this redistribution of blood flow was related to rectal temperature and performance. Future studies should aim to differentiate muscle and skin blood flow, and the associated muscle and skin temperatures, after CWI to verify these findings.
The reduced arm blood flow in the CWI trial (fig 3) persisted until the end of the second performance trial (Ex2) in a fashion similar to rectal temperature (fig 2). This suggests there may have been a reduction in skin blood flow that persisted until the end of Ex2, supporting the notion that there is reduced competition between cutaneous and muscle perfusion, allowing for increased venous return and cardiac efficiency.20 22 Indeed, heart rate was lower during the initial stages of Ex2 after CWI compared with ACT, which is similar to previous findings.32 33 Any differences in venous return may also be the result of plasma volume shifts associated with a difference in sweat rates between the CWI and ACT recovery interventions. Although we matched the fluid intakes of the two trials, we did not measure or control for differences in sweat rates. However, the difference in sweat rates between the trials, particularly over such a short duration (35 min), is likely to be negligible.26 The reduction in HR after CWI may also be the consequence of a more rapid rise in parasympathetic activity that may or may not be independent of blood redistribution.34 During the final stages of Ex2, during the all-out performance-trial phase, there was no difference in heart rate, although significantly more work was completed during the performance-trial after CWI compared with ACT.
Peripheral vasoconstriction and the associated reduction in blood flow has been reported as a negative consequence of CWI because of the influence this is likely to have on the clearance of exercise-induced metabolites such as lactate.31 In the present study, the reduction in blood lactate concentration was slower after CWI than after ACT, which may indeed be due to the lower blood flow. However, as in previous studies,5 blood lactate concentration was not different between CWI and ACT after the 40-min passive recovery period before the second performance trial.
The present study has demonstrated that CWI recovery leads to better maintenance of performance during high-intensity cycling in hot conditions than ACT. The reduction in rectal temperature during CWI was negatively correlated with the performance benefit, indicating that there may be a need to individualise cooling protocols to maximise the performance benefits for individual athletes. The reduction in limb blood flow during CWI was greater in the non-active limbs (arms) compared with the active limbs (legs), suggesting that CWI also leads to a redistribution of blood flow. This adds support to the hypothesis that CWI leads to a redirection of blood flow from the periphery to the core, thereby improving venous return, cardiac efficiency and exercise performance.
Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
What is already known about this topic
Cold water immersion (CWI) recovery leads to a reduction in core temperature and better repeated cycling performance in hot conditions than active recovery (ACT).
What this study adds
▶ Compared with ACT, CWI recovery leads to a redistribution of blood flow, as evidenced by a reduction in blood flow to the legs and an even greater reduction in blood flow to the arms.
▶ The greater the reduction in core temperature with CWI recovery, the smaller the performance benefit compared with ACT.
Acknowledgments
This study was supported by Seed Research Grant through the University of the Sunshine Coast.
References
Footnotes
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the University of the Sunshine Coast and the Australian Institute of Sport, Australia.
-
Provenance and peer review Not commissioned; externally peer reviewed.