Article Text

Abstract
Background and objectives Treatment of chronic running-related overuse injuries by orthopaedic shoe orthoses is very common but not evidence-based to date.
Hypothesis Polyurethane foam orthoses adapted to a participant's barefoot plantar pressure distribution are an effective treatment option for chronic overuse injuries in runners.
Design Prospective, randomised, controlled clinical trial.
Intervention 51 patients with running injuries were treated with custom-made, semirigid running shoe orthoses for 8 weeks. 48 served as a randomised control group that continued regular training activity without any treatment.
Main outcome measures Evaluation was made by the validated pain questionnaire Subjective Pain Experience Scale, the pain disability index and a comfort index in the orthoses group (ICI).
Results There were statistically significant differences between the orthoses and control groups at 8 weeks for the pain disability index (mean difference 3.2; 95% CI 0.9 to 5.5) and the Subjective Pain Experience Scale (6.6; 2.6 to 10.6). The patients with orthoses reported a rising wearing comfort (pre-treatment ICI 69/100; post-treatment ICI 83/100) that was most pronounced in the first 4 weeks (ICI 80.4/100).
Conclusion Customised polyurethane running shoe orthoses are an effective conservative therapy strategy for chronic running injuries with high comfort and acceptance of injured runners.
Statistics from Altmetric.com
Running injuries, particularly located in the lower limb, are among the most commonly treated sports-related injuries.1 Of the latter, overuse injuries are the main pathologic conditions to prevent competitive runners from training or competition.2,–,5 In the past three decades, the incidence of running-related overuse injuries has continuously increased because of a rising number of recreational athletes and higher training intensity in competitive athletes.6,–,8 Several risk factors seem to be associated with those injuries such as weekly distance, history of previous running injuries, number of years running, training characteristics, surface and footwear.1,–,3
The most common diagnoses in running injuries are patellofemoral pain syndrome, iliotibial band syndrome, tibial stress syndrome (often referred to as shin splints), low back pain, chronic exertional compartment syndrome, plantar fasciitis and tendinopathies (particularly of the Achilles tendon, the patellar tendon, the posterior tibial tendon, the adductor tendons and the upper hamstring tendons).9,–,11
Treatment consists most commonly of a multi-oriented approach. Conservative treatment is usually based on a combination of training modifications, anti-inflammatories, infiltrations and physiotherapy including soft tissue mobilisation, deep frictions, stretching and strengthening of involved muscles and physical measures (eg, ultrasound, interferential, cryotherapy and heat).12 Insoles are thought to be an efficient tool in the treatment of running-related overuse injuries through correction of biomechanics, modification of afferent input on the foot sole and minimising muscle work.13,–,19 Patient satisfaction after orthotic therapy has severally been reported, but clear evidence-based data from randomised controlled trials is still rare.20,–,26 In addition, comparison of studies on foot orthoses and transfer to clinical applications is difficult because outcome measures and insole constructions are diverse and often not well detailed in the studies. Two recent systematic reviews on foot orthoses in lower limb overuse conditions showed that there is insufficient evidence to support or refute the use of foot orthoses in the treatment of lower limb overuse injuries to date because methodological quality of the available controlled clinical trials is mostly weak and data are too heterogeneous to pool it.21 23 One high-quality randomised controlled study on 179 patients that found foot orthoses to produce earlier and larger improvements than flat inserts in patients with patellofemoral pain syndrome has additionally been published lately.27
The aim of the present study was to evaluate the influence of standardised individually customised foot orthoses on pain and impairment of daily life in runners with unilateral running-related overuse injuries by a randomised controlled trial.
Methods
This study was conducted at the University Hospital of Freiburg, Germany, in compliance with the European Community Good Clinical Practice (EC-GCP) Note for Guidance and the Consolidated Standards of Reporting Trials (CONSORT) guidelines for randomised controlled trials.28 The study was reviewed and approved by the local university's ethics committee.
Orthoses construction
The sports orthoses used in this study are made out of polyurethane foam material (ethylene vinyl acetate, compression moulded, and semirigid) with a bowl-shaped heel, a medial longitudinal arch support and a detorsion wedge (fig 1; IETEC GmbH, Fulda, Germany, type “Move Control”). They are individually customised based on the participant's dynamic barefoot plantar pressure distribution. In the study, this was conducted by the same orthopaedic technician (HT) using an Emed SF pressure platform (Novel, Munich, Germany).

Running shoe orthosis (polyurethane material with bowl-shaped heel, medial longitudinal arch support and detorsion wedge individually customised by dynamic barefoot plantar pressure distribution measurements).
The particularity of those orthoses is the adaptation of the stiffness of the polyurethane material, depending on the runner's body weight and running velocity comparable with the midsole material of standard running shoes. It is thought that the resulting combination of orthosis and shoe leads to a proper fit and a synergism of their effects. Furthermore, the relatively stiff material is thought to provide a direct feedback from the running surface and thus enhances proprioception of the foot sole. Evidently, proper shoe selection and fit of the orthoses are essential. For this type of orthosis, runners are advised to choose a neutral running shoe without additional stabilising elements. The orthoses showed promising results in daily clinical routine and biomechanical testing in healthy runners.29
Recruitment, participants and group assignment
All runners with unilateral, chronic overuse injuries presenting to the University Outpatient Clinic between July 2002 and July 2005 were eligible for inclusion. Furthermore, runners from the community with unilateral running-related overuse symptoms responded to publicity measures in local newspapers and at local running events. Male and female participants were recruited for the study. Inclusion was based on unilateral running-related overuse injuries, including patellofemoral pain syndrome, iliotibial band syndrome, shin splints, plantar fasciitis and tendinopathies with a duration of >3 months, clinically diagnosed by an independent sports medicine physician (orthopaedic surgeon FM). Additional inclusion criteria were age range between 18 and 60 years, a running distance of >20 miles per week (32 km/wk)10 and the absence of other illnesses and complaints. The exclusion criteria were history of surgery to lower extremities and lumbar spine, signs or symptoms suggestive of an acute injury, any parallel therapies including physiotherapy, insoles, non-steroidal anti-inflammatory drugs or corticosteroid injections during the previous 6 months.
Study procedure
Potential participants were instructed to contact the study coordinator to review the inclusion criteria of the study. If these were met, the sports medicine physician evaluated them to determine if the physical examination criteria were compliant. If the patient met the inclusion criteria and agreed to participate in the study, written informed consent in accordance to the local university's ethics committee was obtained. The study coordinator then obtained background demographic data (age, weekly distance, training characteristics and surface, number of years running, shoes worn, amount and distance of competitions per year and aerobic capacity by individual anaerobic threshold determined by an incremental treadmill test30) and measured the participant's height and weight. All the data were documented in prepared case report forms. A baseline assessment of the study's outcome measurements was then performed.
The outcome measurements were as follows:
(1) Pain disability index (PDI):31,–,35 Assessment of functional disabilities in activities of daily living resulting from running-related injury symptoms. PDI is a seven-item inventory designed to measure the degree to which pain interferes with functioning across a range of activities. The seven categories include family/home responsibilities, recreation, social activity, occupation, sexual behaviour, self-care and life support activity. Each item can range from 0 (no interference) to 10 (total interference). Thus, total PDI score can range from 0 to 70.31,–,35 For statistical evaluation, sum scores of all categories were calculated. PDI is considered reliable for assessment of functional impairment and chronic diseases.35 The validity in overuse injuries has previously been proven.12
(2) Subjective Pain Experience Scale (SES): Pain quality is described by 24 adjectives including sensory and affective pain qualities using simple descriptive scales.12 36 SES was used to quantify the course of current symptoms on measurement days and during the intervention period. A sum score of sensory and affective qualities and a total sum score were calculated with minimum values of 14 points for affective part A (SES-A) and 10 points for sensory part B (SES-B).12 36
(3) Comfort index of orthoses (ICI): Modelled after that of Mündermann et al, orthosis comfort was rated on five independent visual analogue scales ranging from 0 (=‘not comfortable’) to 10 (‘very comfortable’).37 38 The five items included the quality of heel cup fit, longitudinal arch support, flexibility, combination of orthosis and shoe and running with orthosis compared to running without orthosis (‘much worse’ to ‘much better’). A sum score was calculated analogous to PDI. The total ICI score can range from 0 to 100.
After baseline evaluation of the outcome measurements, the patients were instructed how to use the training diary. Distance, duration and intensity had to be documented for every training session. The SES pain questionnaire and the ICI comfort questionnaire for orthoses had to be filled out at the end of each week.
Then, runners were randomly assigned to the control or orthoses group by permuted block randomisation (blocks of four), separated according to sex. The randomisation scheme was generated by using the website http://www.randomization.com (plan Nos. 19189 and 22219) and kept in a locked cabinet. According to the CONSORT guidelines, a research assistant not involved in outcome assessment revealed group allocation, followed by plantar pressure assessment for patients assigned to the orthoses group.28
The following 2 weeks were considered the habituation and instruction phase for the pain questionnaires and the training diary. Accuracy of training documentation was checked at a second appointment 2 weeks later. At that time, orthoses were handed out to the patients of the orthoses group and correct fit in their personal running shoe was evaluated.
The orthoses had to be worn for all physical activities during the intervention phase. This had to be documented in the diaries, as an orthosis use of >80% of training sessions was required. Patients were advised to contact the study coordinator directly in the case of any fitting problems, blisters, bruises or any other new symptoms.
All the participants were advised to continue their regular training activity without modification of training habits. This was controlled by the documentation of distance and duration in the diaries at the end of the study. The outcome measurements were assessed at the end of every week over a period of 8 weeks. After the intervention period, there was another appointment at the study centre including outcome assessment and clinical re-evaluation. If pain was still present in participants of the control group, orthoses were customised for them as well.
Statistics
Baseline data from the case report forms were manually entered into a prepared database and crosschecked twice. All the evaluated data were first analysed for plausibility. Implausible values were compared with the raw data and recalculated, if necessary. In addition, 10% of all values were recalculated from the original data and compared with the values in the database (>95% of the values had to agree).
Change in SES sum score, PDI and ICI over 8 weeks was analysed using descriptive statistics (mean values and SD). The mean difference between the two treatment groups after the 8-week period was compared by using 95% confidence intervals (CI). The primary outcome measures (PDI and SES sum scores) were statistically analysed by a two-factor repeated measure's analysis of variance (α=0.05). The independent variable was the intervention group (orthoses/control), and the dependent variable was the PDI/SES sum score. All statistical analyses were performed with JMP Statistical Discovery Software package V.5.0.1.a (SAS Institute, Cary, North Carolina, USA).
Results
Before treatment
Participants
A total of 63 male and 62 female runners were initially evaluated for the study. After orthopaedic examination and checking of the inclusion criteria, 50 men and 49 women were included and randomised to the two intervention groups (orthoses n=51; control n=48; fig 2).

Flowchart of patient recruitment, randomisation, treatment and follow-up.
Baseline data
The patients' ages ranged from 19 to 52 years (mean (SD) 37.2 (8.3)) and were running a mean weekly distance of 44 km. Most of the participants were experienced runners (regular running activity >3 years, mean 8.1 years) and high-level athletes (mean training speed 5:40 min/km, individual anaerobic threshold >12 km/h). There was no statistically significant difference in any of the baseline criteria between the groups (p>0.05, table 1).
Participant characteristics at baseline for the orthoses and control groups
The most common diagnosis in the 99 patients was Achilles tendinopathy (26 patients), followed by patellar tendinopathy (18 patients), patellofemoral pain syndrome (14 patients), iliotibial band syndrome (13 patients), plantar fasciitis and periostitis tibiae (each in seven patients). Table 2 shows the distribution of the diagnoses in the groups.
Distribution of diagnoses in the orthoses and control groups
Disability and pain
The mean PDI sum score and the mean SES sum score at baseline were similar in the two intervention groups. As presented in table 3, baseline values of the PDI were 4.1 (5.6) in the control group and 4.0 (5.5) in the orthoses group; the baseline values of SES were 31.6 (9.6) in the control group and 29.9 (8.2) in the orthoses group, respectively (p>0.05, table 3).
Group mean values and group mean differences of PDI and SES at baseline and post-treatment
After treatment
During the intervention period of 8 weeks, there were 18 dropouts recorded (fig 1). Six had acute injuries/illnesses, including one forearm fracture, one ankle sprain and one borreliosis infection in the orthoses group and one meniscal injury, one ankle sprain and one acute low back pain in the control group. Four in each group withdrew from the study without specification of causes, and four were excluded because of non-compliance (arbitrary side therapy, inadequate documentation of questionnaires or training habits or reduction of training volume and/or intensity). The dropout rate was equivalent in both intervention groups (17.6% in the orthoses group and 18.6% in the control group); none of the participants changed between groups. Thus, there remained 39 athletes in the orthoses group and 42 athletes in the control group for final evaluation (fig 2).
Disability
There was a statistically significant difference in the group mean values of the orthoses and control groups at the second measurement day for both SES and PDI (p<0.05, table 3). In the orthoses group, the mean PDI sum score decreased from 4.0 to 1.6 after the 8 weeks (p<0.05), whereas it slightly increased from 4.1 to 4.8 in the control group (p>0.05, table 3). When calculated as intra-individual percentages of the baseline values (the PDI sum score at the first measurement day100%), there was a mean reduction of 58% in the orthoses group (95% CI −74% to −43%) and a mean increase of 23% in the control group (95% CI −16% to 62%), respectively (p<0.001, fig 3).

Intra-individual percentage of PDI sum score at M2 (M2/M1×100) for the control and orthoses groups (mean/95% CI).
Pain
The mean SES sum score analogously decreased from 29.9 to 25.9 in the orthoses group (p<0.05) and again slightly increased from 31.6 to 32.5 in the control group (p>0.05, table 3). The statistically significant reduction of SES mean values in the orthoses group were seen in both parts of the questionnaire with affective part values reducing from 17.2 (95% CI 15.6 to 19.0) to 14.9 (95% CI 13.4 to 15.5) and sensory part values reducing from 12.6 (95% CI 11.6 to 13.7) to 10.9 (95% CI 10.5 to 11.6).
In the control group, the increase was only observable in the affective part of the questionnaire: the affective part mean sum score at baseline was 18.3 (95% CI 16.3 to 20.8) versus 19.9 (95% CI 17.2 to 21.0) after the 8 weeks, and the sensory part mean sum scores were 13.3 (95% CI 12.0 to 14.6) at baseline versus 13.3 (95% CI 11.9 to 14.8) after the 8 weeks.
Pain course
Figure 4 shows the course of the mean SES sum scores in the control and orthoses groups during the intervention phase. After a slight increase at the end of the first week in both groups, there was a continuous decrease in the orthoses group the following 7 weeks. The mean values of the control group remained almost constant for 5 weeks and increased again slightly towards the second measuring day. For some individuals in the orthoses group, a longer time passed before they reported a decrease of pain level.
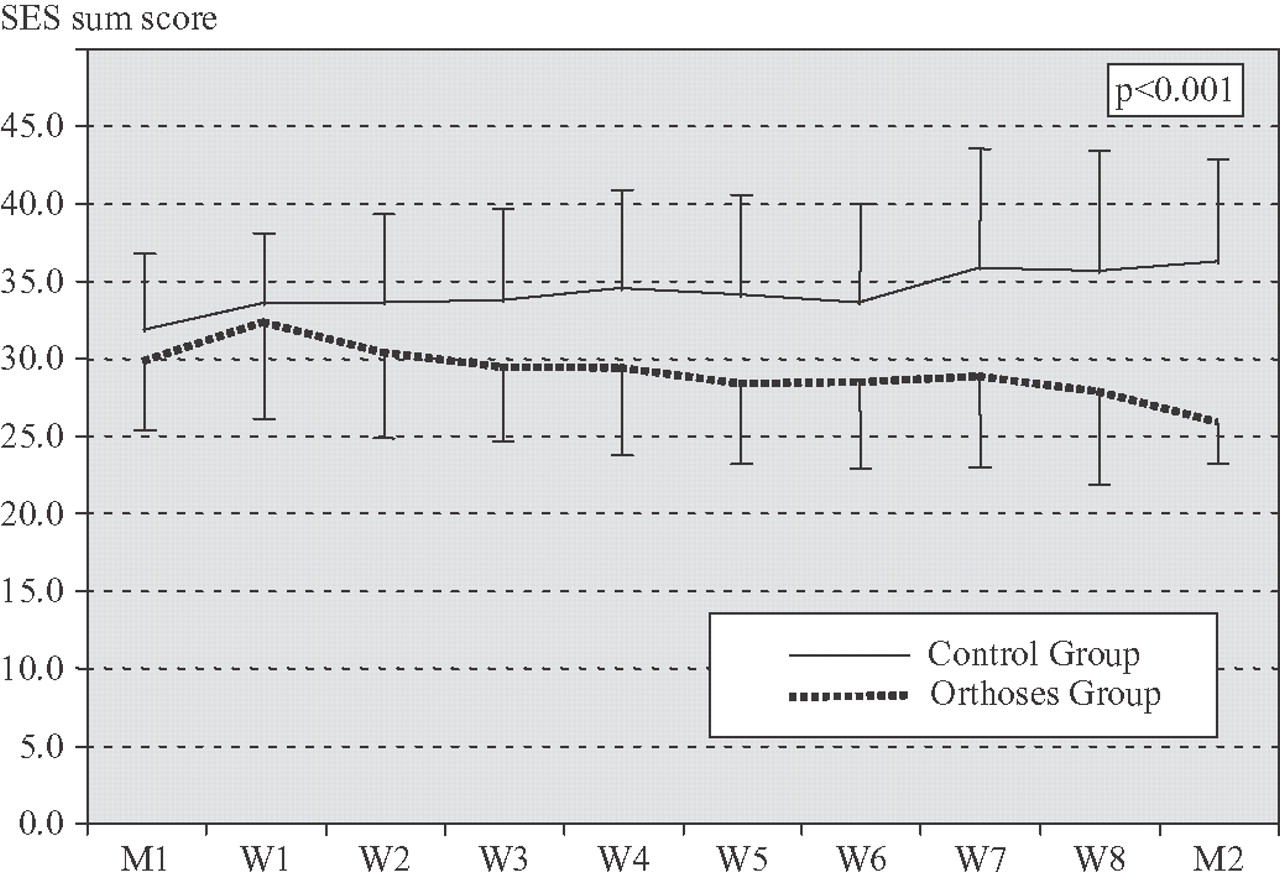
Course of SES sum score during 8 weeks' therapy for the control and orthoses groups (mean/SD).
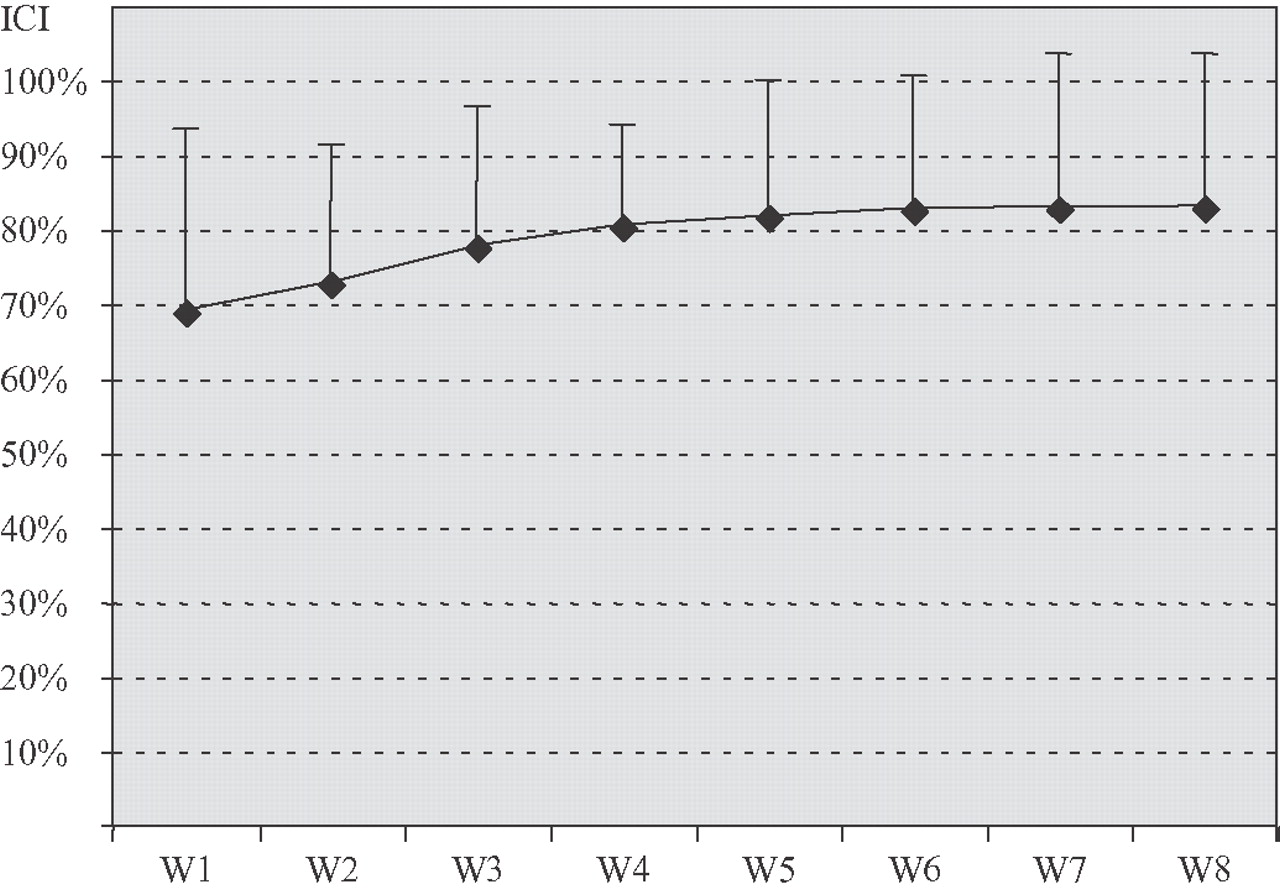
Orthoses comfort
Overall, the patients reported high comfort when wearing the orthoses. All except one of the participants judged the orthoses very comfortable and, after the 8 weeks, preferred running with the orthoses rather than without. Only one runner rejected the orthoses, and one runner used an additional viscoelastic heel cup, so that he had to be excluded from the study. The mean comfort index values of the comfort questionnaire raised by 14% during the intervention phase. There was a 10% increase in the first 4 weeks with mean values rising from 69.0 (95% CI 61.0 to 77.0) to 80.4 (95% CI 75.6 to 85.1), which was most pronounced in the second to third week. No substantial further increase was noted during the second 4-week period (80.4–83.0; 95% CI 75.0 to 91.2; fig 5). When analysing the individual diaries of the patients, in quite a few cases, pain reduction was already apparent in the second week of treatment, whereas satisfaction concerning the comfort of the orthoses took longer.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Course of orthoses comfort index (ICI) during 8 weeks' therapy (mean/SD).
Side effects
There were no adverse effects of the orthoses recorded at all, neither local foot problems nor symptoms in localisations other than the initial ones. One patient rejected the orthoses because he did not like them. All the patients who retired from the study were also asked for adverse effects, and none of them reported any.
Discussion
The present study is one of the first randomised controlled studies on foot orthoses in lower extremity overuse injuries showing a statistically significant pain reduction in runners after a standardised orthoses therapy of 8 weeks. The results revealed statistically significant differences between the intervention and control groups at the second measurement day for both questionnaires, SES and PDI. The pain reduction after the intervention phase was seen in the sensory and the affective part of the SES, with post-treatment values of 14.9 in the affective part and 11.0 in sensory part. As minimum scores (14 points for the affective part and 10 points for the sensory part) were almost reached; this result can be considered not only statistically significant but also highly clinically relevant.
The pain decrease proved in the SES questionnaire was accompanied by a significant reduction of the impairment in activities of daily living, expressed by a 58% decrease in PDI sum score, which must be considered a relevant reduction.
Nevertheless, compared with the maximum value of 96 for SES and 70 for PDI, the mean values of the injured runners at baseline and the absolute improvement during the intervention phase were rather low. As floor effects are very likely when investigating sport-specific injuries that do not highly affect everyday living, the use of more specific pain questionnaires and functional disability measures—for example, the VISA questionnaire in Achilles and patellar tendinopathy, should be implemented in further therapy studies.
Regarding the course of the pain level during the 8 weeks, it was interesting to see that the SES sum score initially slightly increased. Transferring these results to clinical practice, it seems important to prepare patients for a possible pain increase at the beginning of an orthoses therapy so that they do not immediately stop using the orthoses.
Concerning possible mechanisms for the effect achieved by the orthoses, it is currently speculated that neuromuscular adaptations and reduction of muscle fatigue play the most important role.15 21 29 39 40 Mündermann et al showed changes in electromyographic pattern as an expression of neuromuscular changes related to different insoles.15 40 To support the hypothesis of sensorimotor effects of the orthoses used in this study, a pilot study including electromyography and plantar pressure measurements was conducted before. Using the same type of orthoses, Baur et al showed an increasing electromyographic activity of the peroneus longus muscle accompanied by higher peak pressure values under the midfoot when wearing orthoses with a longitudinal arch support.29 39 As higher electromyogram activity of the peroneal muscle might imply enhanced joint stability in the stance phase of running, this leads to the conclusion that modification of the sensory input to the sole can considerably influence neuromuscular response patterns and that neuromuscular adaptations may be more important than mechanical corrections.29 39 41 The fact that the adaptation to the orthoses seems to be almost completed after 4 weeks of therapy supports this hypothesis of a mainly sensorimotor effect as it is well known that the results of sensorimotor training show within 4 weeks.42
In addition to the improvement in pain and functional disabilities, the participants showed very good compliance in wearing the orthoses. All except one runner reported a high satisfaction concerning wearing comfort. This is probably due to a good fit of the customised orthoses, as it is postulated that orthoses fit when running is essential to provide comfort and to not hamper the natural rollover process of the foot. 43 44 In this study, this was allowed by customising the orthoses to the runner's individual dynamic barefoot plantar pressure distribution and by using polyurethane material similar to the midsole of running shoes. The polyurethane does not provide additional cushioning so that proprioception is not altered. Robbins and Gouw showed a reduction of afferent input from the foot sole when wearing soft shoes or walking on soft ground and concluded that soft materials negatively influence feedback.45
An additional important reason for the high satisfaction and compliance to the orthoses therapy certainly is that runners usually prefer therapies that do not imply a reduction of running distance and do not require any additional training time. As orthoses generate their effect when running, it is even important for their effectiveness that patients continue their running activity.
Some limitations of the study have to be considered when interpreting the results. A lack of the study certainly is that therapy was not blinded and that only one orthoses type was tested. As there was no comparative sham orthosis, it cannot be proven that the sports-specific model used in the study is more effective than standard models or prefabricated ones. Because of the fact that all patients included in this study were still able to continue their regular training activity with a weekly distance of at least 32 km, transfer of the study results to other populations with more severe symptoms is limited. As repetitive loading of the orthoses seems to be the most important factor for their effectiveness, this type of therapy can only work as long as the runner is able to run. Additionally, all types of overuse running injuries were included in the study. Thus, the results are not diagnoses-specific and may not apply to all diagnoses to the same degree.
Conclusions
The results of this study indicate that individually customised foot orthoses are an important effective treatment strategy for running-related overuse injuries. In contrast to the widespread opinion that “orthoses are only one facet of treatment and should be combined with rest, training modification, a change in the running surface or shoe and a proper conditioning and stretching programme”, the results of our study justify the prescription of orthoses as a single-measure approach for runners that are still able to continue their training activity while the majority of participants responded well without any side treatments and reported high comfort wearing the orthoses.24
What is already known on this topic
▶ Running-related overuse injuries are among the most frequent reasons for consulting a sports medicine practitioner.
▶ Foot orthoses are often prescribed for those injuries despite a lack of high-quality evidence from randomised controlled trials as highlighted by two recent systematic reviews.
What this study adds
The results of this randomised controlled study show that foot orthoses are an effective treatment strategy for overuse injuries with a high acceptance by injured runners.
Acknowledgments
The authors acknowledge study coordinator Mrs Katrin Renner and the doctoral thesis students involved in data collection, as well as Dr Manfred Baumstark for his help in the statistical evaluation.Our appreciation is also extended to the IETEC GmbH, Fulda, Germany, and Herbert Türk (HT), Fuß-Vital-Center Türk, Freudenstadt, Germany, for the support of the orthoses and their customisation.
References
Footnotes
-
Funding This research was supported by a grant from the National Institute of Sports Science (BISP), Bonn, Germany.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the University of Freiburg's ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.