Article Text

Abstract
Background Growth factor technologies are increasingly used to enhance healing in musculoskeletal injuries, particularly in sports medicine. Two such products; platelet-rich plasma (PRP) and autologous blood, have a growing body of supporting evidence. No previous trial has directly compared the efficacy of these two methods.
Hypothesis Growth factor administration improves tissue regeneration in patients who have failed to respond to conservative therapy.
Study design A prospective, double-blind, randomised trial.
Methods Elbow tendinopathy patients who had failed conservative physical therapy were divided into two patient groups: PRP injection (N=80) and autologous blood injection (ABI) (N=70). Each patient received two injections at 0 and 1 month. Patient-related tennis elbow evaluation (PRTEE) was recorded by a blinded investigator at 0, 1, 3 and 6 months. The main outcome measure was PRTEE, a validated composite outcome for pain, activities of daily living and physical function, utilising a 0–100 scale.
Results At 6 months the authors observed a 66% success rate in the PRP group versus 72% in the ABI group, p=NS. There was a higher rate of conversion to surgery in the ABI group (20%) versus the PRP group (10%).
Conclusion In patients who are resistant to first-line physical therapy such as eccentric loading, ABI or PRP injections are useful second-line therapies to improve clinical outcomes. In this study, up to seven out of 10 additional patients in this difficult to treat cohort benefit from a surgery-sparing intervention.
Statistics from Altmetric.com
The ability to augment the healing of musculoskeletal injuries remains an elusive goal in modern medical practice. In elite and professional sport, intense pressure exists to accelerate an athlete's ‘return to play’, because injury can rapidly prove costly both in terms of performance and finance. In non-elite and recreational exercise, injury can cause rapid demotivation, with a slide towards sedentary behaviour, or prolonged work absence. Eccentric loading remains the accepted first-line therapy for tendinopathy, but is not always successful, and requires high levels of patient motivation.1
Complex growth factor preparations, derived from the patients' own (autologous) blood, are used to drive the body's own tissue healing mechanisms in the hope of stimulating rapid healing. Such preparations are used increasingly in sports medicine to accelerate healing from injury, although evidence of efficacy is based only on cohort studies, animal studies or small randomised controlled trials.2,–,8 35 However, there is no standard technique for harvesting growth factors for administration,9 and several different preparations are described in the literature, namely autologous blood injection (ABI),2 leucocyte-depleted, moderate-yield platelet-rich plasma (PRP),10 11 essentially plasma with erythrocytes and leucocytes removed and leucocyte-rich, high-yield PRP—‘buffy coat’.4 12 These preparations can only be classified on an individual basis according to erythrocyte, leucocyte, platelet and growth factor (insulin-like growth factor 1, epidermal growth factor, hepatocyte growth factor, vascular endothelial growth factor, fibroblast growth factor, platelet-derived growth factor, transforming growth factor beta 1) content.9 13 14 Such blood-derived preparations also contain several thousand other platelet-derived and plasma-derived biologically active substances that have received scant attention in the PRP literature so far.15
No trial has directly compared the efficacy of these two techniques head to head or against a placebo. We present a trial comparing ABI—‘whole blood’ with moderate-yield PRP—‘plasma’ in the management of resistant elbow tendinopathy.
Methods
Main outcome measure
A single outcome measure, the patient-related tennis elbow evaluation (PRTEE) score was used. The PRTEE is a well validated 0–100 composite scale measuring pain and physical function.16 Patients completed the PRTEE at baseline (PRTEE1), second injection at 1 month (PRTEE2), 3 months (PRTEE3) and 6 months (PRTEE4). We defined a clinically significant improvement in PRTEE as 25 points on the scale, which is comparable to other studies.17 In a therapy-naive group of patients this may seem like a small gain; however, this cohort of patients had already received extensive previous therapy, meaning any additional improvement is difficult. As the mean PRTEE score at the outset in our cohort of patients was 49, a 25-point improvement represents an approximately 50% reduction in scores in our cohort. This represents a considerable effect size in previously ‘resistant’ patients. The questionnaire was administered by the research assistant specifically recruited for this task.
Power calculation
Based on the pilot study we estimated a SD of 20 (σ=20) for mean improvement in PRTEE scores from 0 to 3 months in both groups, with a minimum clinically significant improvement within groups of 25 (δ=25). We defined the minimum clinically significant between-group difference as 10 (δ=10). We set the significance level, α, at 0.05 (α=0.05) and power at 90% (1-β=0.9).
For within-group analysis of improvement this yielded a necessary enrolment of 11 patients per group to detect a change of 25 points in PRTEE. However, our null hypothesis was that both groups (plasma or blood) would improve by the same amount. To detect a difference of 10 points on the PRTEE scale in mean improvement between the plasma and blood groups required 44 patients in each arm. Allowing for up to 20% loss to follow-up we aimed to enrol at least 52 patients in each group.
Technique
All patients included in the trial had previously failed therapy using conservative measures including physical therapy exercises (stretches and eccentric loading). Patients who had previously had a corticosteroid injection, dry-needling or blood injection were also excluded. Patients had to have had symptoms for a minimum of 6 months to be included in the study.
All patients signed informed consent documentation.
Blood was collected using a 21 gauge needle from the antecubital fossa into an 8.5 ml vacutainer tube with citrate anticoagulant. For patients randomly assigned to plasma injection, the blood was spun in a centrifuge at 2000g for 15 min (LC6; Sarstedt, Numbrecht, Germany) and 1.5 ml was siphoned from the buffy coat layer.
Tendons were first surface bathed with 2 ml bupivacaine, followed by a 2 min wait before proceeding to blood or plasma injections. Patients were advised to continue normal activities, but to avoid any physical activity or heavy carrying for the next 48 h. They were allowed to ice the elbow and take paracetemol as necessary, but to avoid anti-inflammatory drugs.
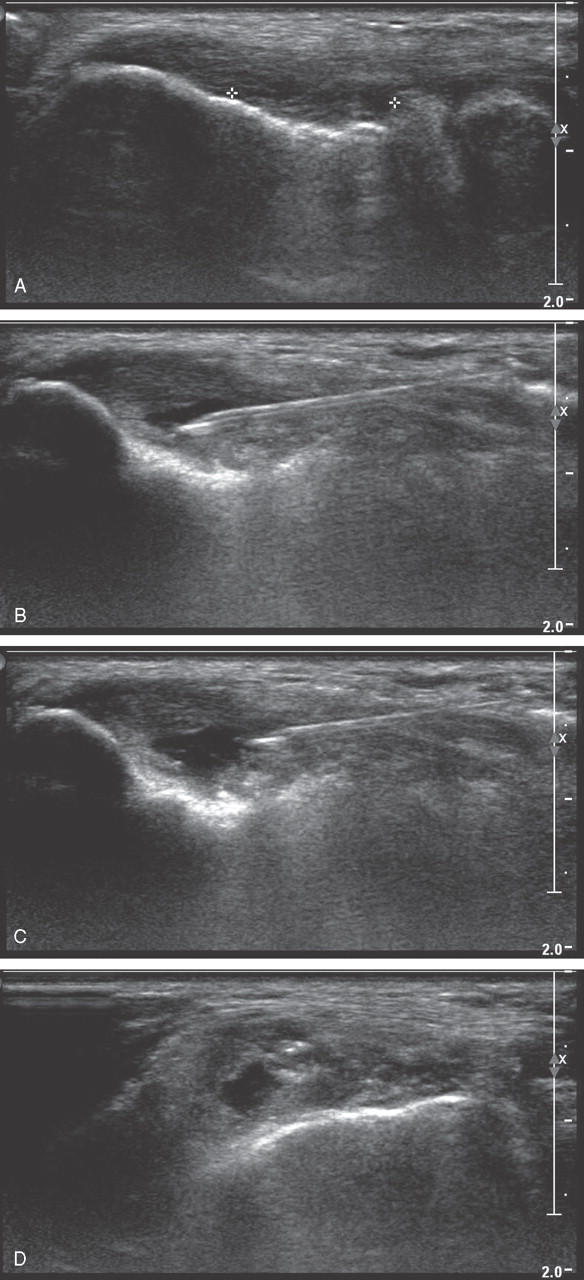
All injections were performed by the same operator, a musculoskeletal radiologist with 15 years experience and 20 000 ultrasound scan-guided injections performed, including 3000 ABI. Preparation was injected into clefts of hypoechoicity using a 23G needle within the tendon using minimal pressure. To minimise trauma, no dry needling was performed (figure 1).
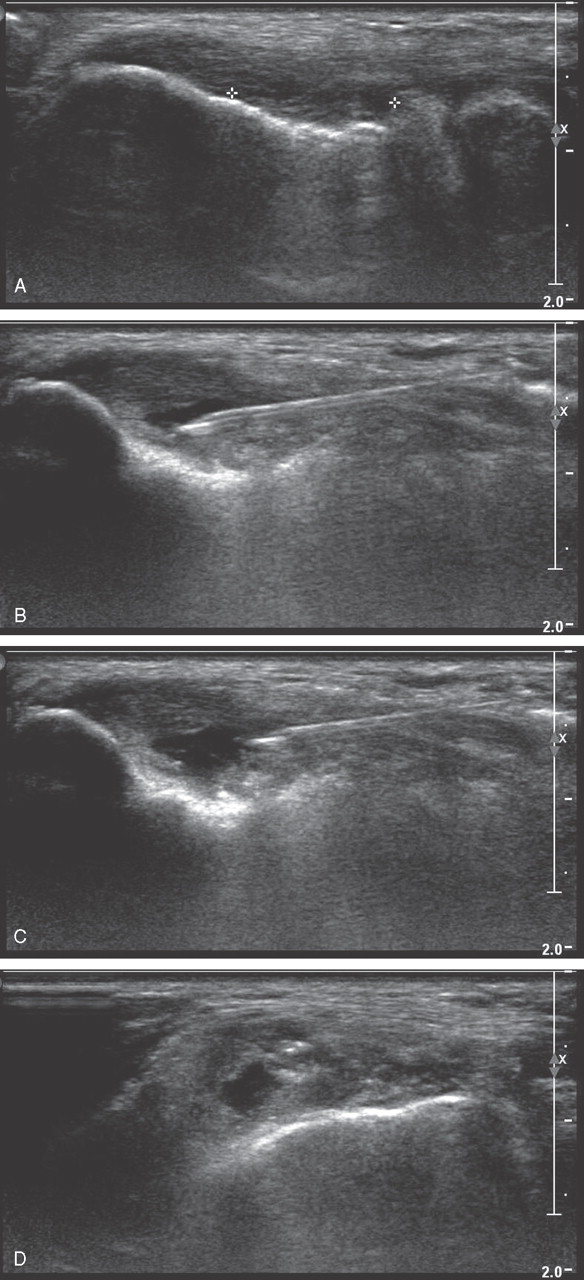
Injection of platelet-rich plasma (PRP) within an intratendinous tear. (A) Intratendinous cleft (tear) identified between markers. (B) Cleft is seen to open into a cavity using minimal pressure. (C) PRP is injected into the cavity. (D) Transverse section demonstrating fluid (PRP) filled cavity.
Patients had a course of two injections at time point 0 (PRTEE1) and 1 month (PRTEE2).
Statistical analysis of the results was performed using Excel 2003 and SPSS version 18. The intention-to-treat analysis utilises a crude success/failure outcome measure for each group, yielding a 2×2 contingency table tested with the χ2 test. The efficacy subset analysis utilises the actual mean improvement in PRTEE, a continuous variable on a 0–100 scale, for which we have used a two-tailed Student's t test.
Results
Demographics
Table 1 displays the basic demographics of the study population.
Demographics
Randomisation
One hundred and fifty consecutive patients were randomly assigned by means of sealed envelopes to receive a course of two ultrasound-guided blood or plasma injections (plasma, n=80; blood, n=70). As a result of loss to follow-up, complete datasets at analysis included 130 patients who were included in the final analysis (plasma, n=70; blood, n=60), an attrition of 20 patients or 13% (plasma, n=10; blood, n=10). Statistics are calculated with both intention-to-treat and efficacy subset analysis for comparison.
Platelet count of plasma and whole blood samples
Ten random samples from each group were sent for platelet counts to verify the elevation in platelet counts from baseline in the plasma (PRP) group compared with whole blood samples. Individual platelet counts are presented below, with means and 95% CI in table 2:
Platelet concentrations of plasma and blood samples used for injection therapy
Whole blood (platelets×109): 212, 232, 189, 310, 259, 179, 202, 200, 252, 304
Plasma (platelets×109): 601, 659, 459, 702, 849, 776, 567, 689, 672, 542
Homogeneity of groups
For all 150 patients randomly assigned the mean PRTEE1 was 48.8 (46.1–51.5). At baseline PRTEE1 was 45.8 (41.9–49.6) in the plasma group and 52.5 (48.5–56.5) in the blood group, a difference of 6.7, with overlapping 95% CI. Therefore, we concluded that the groups were comparable at baseline.
Intention-to-treat analysis
At final evaluation complete data was not available for 20 cases (13%) due to loss to follow-up, meaning genuine intention-to-treat analysis was not possible. Next best analysis included an evaluation of all remaining patients with complete datasets who persisted with injection therapy or elected to have surgery.
We defined success as an improvement in the PRTEE score of 25 points at final analysis, and outright failure as an improvement of less than 25 points or progression to surgery. The composite failure rate is defined as the sum of outright failures and surgery.
This yielded a success rate of 66% (95% CI 55% to 77%) in the plasma group versus 72% (95% CI 61% to 83%) in the blood group, p=0.59 (NS) (figure 2).

Intention-to-treat flowchart.
There is extensive crossover between the ‘failure’ and ‘surgery’ outcome groups, because patients failing injection therapy opted, in the vast majority of cases, to have surgery. Furthermore, a higher proportion of the blood group failures elected to proceed to surgery (12/17) than in the plasma group (7/24). It is not clear why this is the case, and may represent statistical chance.
Efficacy subset analysis (figure 3)
Excluding patients who opted for surgery meant that quantitative statistical comparison was possible for 63 (46+17) patients in the plasma injection group versus 48 (43+5) in the blood injection group.

Improvement in patient-related tennis elbow evaluation (PRTEE) scores from beginning to end of trial (efficacy subset analysis).
At time point PRTEE3, the mean improvement in the PRTEE score from PRTEE1 to PRTEE3 in the plasma group was 33 (95% CI 28.2 to 37.8) versus 37.7 (95% CI 32.2 to 43.3) in the blood group. These improvements were both greater than the predefined clinically significant improvement of 25. The between-group difference of 4.7 with overlapping CI did not amount to the predefined clinically appreciable between-group difference of 10.
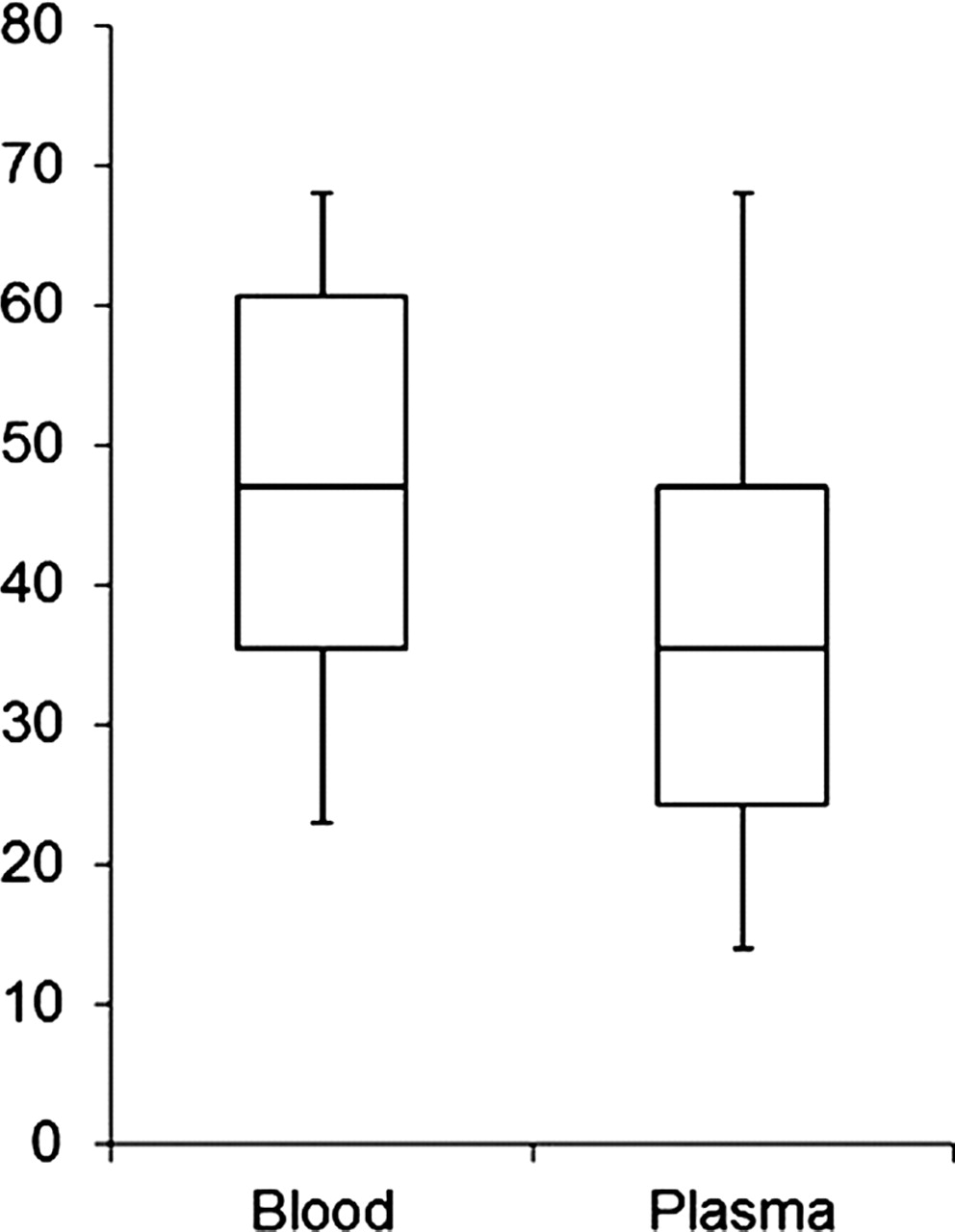
At time point PRTEE4, the mean improvement in the PRTEE score from PRTEE1 to PRTEE4 in the plasma group was 35.8 (95% CI 30.3 to 41.4) versus 46.8 (95% CI 42.1 to 51.5) in the blood group. These improvements were both greater than the predefined clinically significant improvement of 25. The between-group difference of 11 with non-overlapping 95% CI was greater than the predefined clinically significant between-group difference of 10 (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box and whisker plot for improvement in patient-related tennis elbow evaluation from 0 to 6 months. Mean (line), IQR (box), 9th and 91st centiles (whiskers).
Caution is advised against concluding that there is a true difference at time point PRTEE4, because a higher proportion of blood group failures are removed from this groups analysis as a result of opting for surgery. This creates a false elevation in the mean improvement for the remaining patients analysed.
Conclusions
The intention-to-treat analysis reveals that both ABI and plasma injections are effective in producing a clinically significant reduction in PRTEE pain scores at 6 months in a cohort of patients with previously resistant elbow tendinopathy. In up to 70% of cases, injection therapy can succeed when conservative physical therapy has already failed, and both methods appear to be of comparable efficacy. The efficacy subset analysis is suggestive of equal efficacy at 3 months, with a slight superiority of ABI at 6 months. Caution is exercised in drawing this conclusion because a higher proportion of ABI-treated patients elected to have surgery, causing a false elevation in mean PRTEE scores for the remaining patients in the cohort.
We thus recommend PRP/ABI injections as important second-line options in patients for whom conservative physical therapy has failed.
Limitations of the study
As evidence of efficacy exists for both of these methods,2 6 17 it was not considered ethical to include an inactive placebo control group. However, a follow-up study could compare these novel therapies with a well-established and common treatment modality such as a corticosteroid injection. The lack of a placebo group in our trial, or blinding of the investigator, means we cannot with certainty rule out a placebo effect from our injections, or the introduction of bias at the treatment stage. In defence, patients were blinded to treatment modality at the time of injection and follow-up, and a separate investigator evaluated the outcome measures, meaning bias was kept to a minimum.
Our primary outcome measure, the PRTEE, is a clinical tool that measures patient satisfaction with treatment, an appropriate emphasis. However, we were not able to correlate clinical findings routinely with ultrasound appearances or histology without unduly inconveniencing our patients.
We chose a two-injection protocol, which is our established clinical practice. There are also instances in the literature in which a one-injection,4 6 7 18 three-injection5 or four-injection8 protocol have also been used, demonstrating the heterogeneity within therapeutic growth factor research. Furthermore, evidence exists regarding the cell toxicity of local anaesthetics, albeit in myocytes, not tenocytes;19 however, their use is unavoidable considering the pain associated with these injection techniques.
The follow-up period of 6 months may be considered short; however, the data confirm an enduring benefit from the 3 to the 6-month time points.
There are several facets to the injection technique described, including the use of marcaine, and unavoidably, a degree of ‘dry needling’. Both of these elements may in themselves have therapeutic effects that potentially confound our results.
Unfortunately, as a result of the significant amount of pain associated with this technique, marcaine had to be used. A repeat study could include arms that use marcaine alone without any other active treatment, and dry needling alone.
Discussion
We believe our data contribute to the maturing body of evidence that complex growth factor preparations are an effective treatment modality for refractory tendinopathy. De Vos et al6 studied conservative therapy-naive patients, and were unable to demonstrate a statistically significant additional benefit (improvement beyond that gained with eccentric loading) in VISA-A (Victoria Institute of Sport Assessment-Achilles) scores between PRP (21.7) and placebo (20.5) treated patients. We alternatively examined a subgroup of elbow tendinopathy patients who appeared to be resistant to the benefits of eccentric loading, and were able to demonstrate further benefit in up to 70% of these patients. We therefore argue that in a difficult group of patients in whom conservative therapy fails, ABI/PRP can be used as effective second-line therapy, preventing surgery in a majority of patients who would previously have had no other option.
It is difficult to extrapolate these results to other forms of tendinopathy such as that seen in the Achilles or patella; however, the pathological processes are presumably similar. Our findings raise important questions about how much growth factor needs to be delivered to an injury site in order to stimulate healing, because a normal concentration of platelets appeared to be as efficacious as a higher concentration. ‘Less’ may in fact be ‘more’.5 9 11 20
What is already known on this topic
There is limited animal, cohort and small randomised controlled trial evidence that growth factor delivery methods such as autologous blood and PRP can accelerate and enhance healing in soft-tissue or bony injury.
What this study adds
▶ There is a group of patients with elbow tendinopathy who fail traditional conservative physical therapy.
▶ These difficult-to-treat patients often need surgery.
▶ This study supports the notion that up to 70% of these patients may be spared surgical intervention following growth factor administration.
▶ The procedure can be performed by surgeons, physicians or radiologists in the office setting.
Tendinopathy is an ‘avascular’ injury. Tendons have a poor blood supply, which is implicated in their poor capacity to regenerate.21 Furthermore, the neovessels22 seen in some tendinopathies are proposed to represent a failed attempt to bring nutrients to areas of microtears within a tendon.23 Operative findings in tendinopathy are usually a relatively bloodless field with areas of mucoid degeneration.24 Given this situation, it is presumably of benefit to a tendon for any exogenous growth factors to de delivered to the site of injury, as this will provide some stimulation rather than none at all. Increased stimulation with a higher concentration of growth factors (as in PRP) may not be possible because physiological mechanisms may already be driven to work at maximum capacity. Analogous situations exist elsewhere within human physiology. Many enzymes are easily saturated, displaying ‘zero-order’ kinetics, for example, alcohol dehydrogenase.25 There is certainly cell culture evidence to suggest that once stimulated to a certain point, cells of fibroblast-tenocyte lineage cannot produce collagen at a higher rate.11 20 26 It is possible that this level of stimulation may be reached using a baseline concentration of platelets seen in whole blood. Furthermore, there are many other factors within blood with the potential to influence healing.15
In our study the benefit of two injections continued long after the platelets would have been expected to have secreted all stored growth factors and perished. It has been postulated that the delivery of vascular endothelial growth factor (which is expressed in fetal tendons, but not mature tendons), which is responsible for angiogenesis, may explain the enduring benefit.27
Although this argument is feasible, it is entirely hypothesis, and may not apply to other types of ‘bloody’ injuries such as muscle tears. In muscle injury, a haematoma forms at the site of injury, so it is inconceivable that further benefit could be achieved by injecting more of the same. With muscle injuries, strategies have concentrated more on limiting the initial secondary extension of damage by activated neutrophils with traumeel28 29 in Europe, or corticosteroids30 in the USA. Furthermore, preventing fibrosis by blocking the expression or action of transforming growth factor beta 131–33 has been trialled in animals.
Scientific study of these techniques has received attention from the World Anti-Doping Agency,34 which has now relaxed its embargo on using these preparations to treat most injuries in elite athletes. Sports persons may now be treated with PRP provided a declaration of use is provided. The exception is muscle injuries for which PRP injection requires a therapeutic use exemption. The use of these techniques is increasing, and will filter down to non-elite and recreational exercisers also. As such it is imperative to produce robust trials of efficacy.
Areas for further research
Further prospective research is needed in other tendon conditions to confirm the healing properties of complex growth factor preparations, together with elucidation of the optimum methods of preparation and dosing regimen. It is also important to know what elevation of growth factor, platelet, white cell concentration or other factors is required to boost physiological healing mechanisms.
References
Footnotes
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Royal National Orthopaedic Hospital Ethics Committee.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.