Article Text

Abstract
Background There is a risk of concussion when playing rugby union. Appropriate management of concussion includes compliance with the return-to-play regulations of the sports body for reducing the likelihood of premature return-to-play by injured players.
Purpose To describe the proportion of rugby union players who comply with the sports body's regulations on returning to play postconcussion.
Study design Prospective cohort study.
Methods 1958 community rugby union players (aged 15–48 years) in Sydney (Australia) were recruited from schoolboy, grade and suburban competitions and followed over ≥1 playing seasons. Club doctors/physiotherapists/coaches or trained injury recorders who attended the game reported players who sustained a concussion. Concussed players were followed up over a 3-month period and the dates when they returned to play (including either a game or training session) were recorded, as well as any return-to-play advice they received.
Results 187 players sustained ≥1 concussion throughout the follow-up. The median number of days before players returned to play (competition game play or training) following concussion was 3 (range 1–84). Most players (78%) did not receive return-to-play advice postconcussion, and of those who received correct advice, all failed to comply with the 3-week stand-down regulation.
Conclusions The paucity of return-to-play advice received by community rugby union players postconcussion and the high level of non-compliance with return-to-play regulations highlight the need for better dissemination and implementation of the return-to-play regulations and improved understanding of the underlying causes of why players do not adhere to return-to-play practices.
Statistics from Altmetric.com
Introduction
A high incidence of concussion in contact sports, such as rugby union, is reported, with Australian community rugby union players1 experiencing almost eight concussions per 1000 player game hours. Given the sizeable incidence of concussion and the potential for prolonged adverse effects or delayed long-term consequences (ie, chronic traumatic encephalopathy) associated with premature return-to-play,2 ,3 greater focus on the management and prevention of concussion is needed.
For the management of concussion, the Australian Rugby Union4 recommends that community players and coaches follow the regulations endorsed by the International Rugby Board (IRB), namely that all players who suffer concussion take a 3-week break from both training and games. This regulation is mandatory for players in age-graded competitions (ie, junior players younger than 19 years); however, other players may return to play within the 3-week period only if they are found to be symptom-free and declared fit to play by a recognised neurological specialist after assessment.4 ,5 The extent of compliance with these regulations is unknown, including the extent of its implementation in Australian community rugby union.
Finch6 ,7 has highlighted the need for a much greater focus on translation and implementation research. For example, there is a paucity of research pertaining to the compliance, knowledge and awareness of the regulations or guidelines for returning to play postconcussion. In a recent Canadian study,8 33% of ice hockey players who were advised by a physician not to return to play postconcussion were non-compliant. Furthermore, 80% of the non-compliant players continued to suffer postconcussion symptoms 2 or more years later.8 In another Canadian study,9 almost 25% of ice hockey players did not know whether a player who was experiencing symptoms of concussion should continue playing. Similarly, an American study found that almost half of all high school athletes failed to comply with the American Academy of Neurology10 return-to-play guidelines and 40% returned to play prematurely.11 In New Zealand, high school rugby union players also had limited knowledge of the concussion guidelines12 and of players who subsequently sustained a concussion, over half reported returning to play without medical clearance, and 22% against physicians' orders.
In community sport, the responsibility for implementation and adoption of sports safety measures, including regulations and guidelines for concussion management, involves different levels of sports delivery.7 Even though the goal is to improve player safety and injury outcomes, it is most commonly the role of clubs, coaches or other support staff (rather than the players themselves) to ensure that injury prevention measures are in place. In a study of certified athletic trainers of American football, soccer, basketball and baseball, only 3% were found to fully comply with the concussion management guidelines.13 In New Zealand, 48% of rugby union club teams irregularly used standardised procedures regarding return-to-play after musculoskeletal injury, with only 12% of club personnel (and 16% of players) believing that full recovery was essential before a player returned to competition.14 Team medical staff or coaches are often called upon to make a return-to-play decision based on limited observation of the player and a brief sideline evaluation. Return-to-play decisions are often therefore, made against the backdrop of a noisy sports ground where there may be pressure from coaches and players to return the injured player to the field as quickly as possible15 or for them to not leave the field at all.
Among school and club-based community rugby union players in Australia, only 8% of players who had sustained a concussion injury missed more than two games due to the injury.16 Returning to play prematurely postconcussion has been shown to slow reaction times in athletes,17 leading to an increased risk of re-injury.18 Premature return-to-play postconcussion can also increase an athlete's risk of suffering more severe postconcussive symptoms,19 and in cases of multiple concussions has been shown to be a risk factor for the lowering of cognitive ability20 or later in life, cognitive impairment.21
To date, there have been few studies that have examined a player's compliance with return-to-play regulations, postconcussion in any sport. This article represents a snapshot of practice derived from a cohort study and identifies a gap between regulation and practice, namely a failure in translation and implementation.6 This study reports the proportion of community rugby union players complying with postconcussion return-to-play regulations and the self-reported level of return-to-play advice provided to them.
Methods
A cohort of 1958 male community rugby union players aged 15–48 years from the Sydney metropolitan area was recruited preseason from suburban, grade and schoolboy competition levels. At baseline, each player completed a self-administered questionnaire on age, competition level and a 19-item sensation-seeking scale assessing impulsive behaviour, player characteristics (ie, rugby experience, playing position, training volume and protective equipment use), and the number of concussions in the previous 12 months etc. Study participation ranged from one to three playing seasons (2005–2007), with most players (85%) followed for one season.
The injury event of interest was concussion and this was reported either by a trained injury recorder (n=12) who attended school games, or by a nominated suburban or grade club coach (n=7), a physiotherapist (n=13) or doctor (n=2). Players were recorded as sustaining a concussion during the game if they received a knock to the head that resulted in (1) stoppage of play, (2) the player receiving medical attention and/or (3) the player leaving the field. Concussed players were further followed up at five intervals over a period of 3 months by researchers to monitor the injury treatment, management and return-to-play advice they received, as well as their actual return-to-play behaviour regarding both training sessions or games.
Injury report forms relating to each player's concussion were completed and forwarded to the researchers after the game by the assigned team doctor, physiotherapist or coach. The injury report included details such as whether the injured player left the field or returned to play during the same game. Player game exposure was collected from team lists, and return-to-play times were both self-reported by the player as well as extracted from records of the weekly player team lists. The main outcome of measure was the number of days accrued (postconcussion) until the player returned to play (either competition game play or a regular team training session), and this estimate was calculated from the date the concussion was sustained until the first regular team training session or competition game the player was next actively involved in. Concussed players were identified as being ‘compliant’ with the return-to-play regulations if they did not return to play (either competition game play or a regular team training session) for 3 or more weeks postconcussion. Players were identified as ‘non-compliant’ if they were actively involved in either competition game play or a regular team training session (or both) before the end of the 3-week stand-down period. Comparisons were made with player return-to-play times and compliance with return-to-play regulations in relation to returning to competition game play, regular team training, or both.
Statistical analysis
Data analysis was performed using SPSS version 17.0.22 Descriptive statistics were calculated and a Kaplan–Meier survival curve was plotted to illustrate the time taken to return to play for players who sustained at least one concussion, including the proportion of players who returned to play prior to completion of the regulation 3-week stand-down period.
Bivariate analyses were undertaken to identify associations between compliant and non-compliant players returning to play. Associations between compliant/non-compliant player return-to-play behaviour across player subgroups were analysed by χ2 tests. Statistical significance was accepted at p<0.05. The frequency of injured players receiving return-to-play advice was calculated, as well as the type of advice received and from whom it was received.
Only a small number of players sustained >1 concussion throughout the study and therefore, the χ2 analyses were restricted to the first or only concussion sustained by players (n=187) although descriptive statistics are presented for players with ≥1 concussion. Twenty injured players (11%) sustained their concussion during the last game of the season and therefore did not provide return-to-play data; and 17 players (9%) were missing return-to-play or injury data and therefore not included in the analyses.
Results
Ten percent (n=187) of the cohort sustained one or more concussions (range 1–4) during the observational period of the study, with a total of 215 concussions sustained overall. Of the 187 concussed players, 163 players sustained one concussion, 24 players sustained two, 3 players sustained three and 1 player sustained four concussions. The median number of days until players returned to either competition game play or a regular team training session following their first concussion was 3 (range 1–84); 87% of concussed players returned to either competition game play or a regular team training session within 1 week, 91% by the second week and 95% by the third week. The Kaplan–Meier survival curve (see figure 1A) illustrates the time taken for players after the first concussion to return to either competition game play or a regular team training session. The median time to return to either competition game play or a regular team training session after the second concussion was 7 days (range 0–120), with 95% of players returning to play within 3 weeks. The high proportion of players returning to either competition game play or a regular team training session prior to completion of the 3-week stand-down period was the same whether it was the player's first or second concussion. Of the three players who sustained a third or fourth subsequent concussion, 67% returned to either competition game play or team training within the 3-week stand-down period.
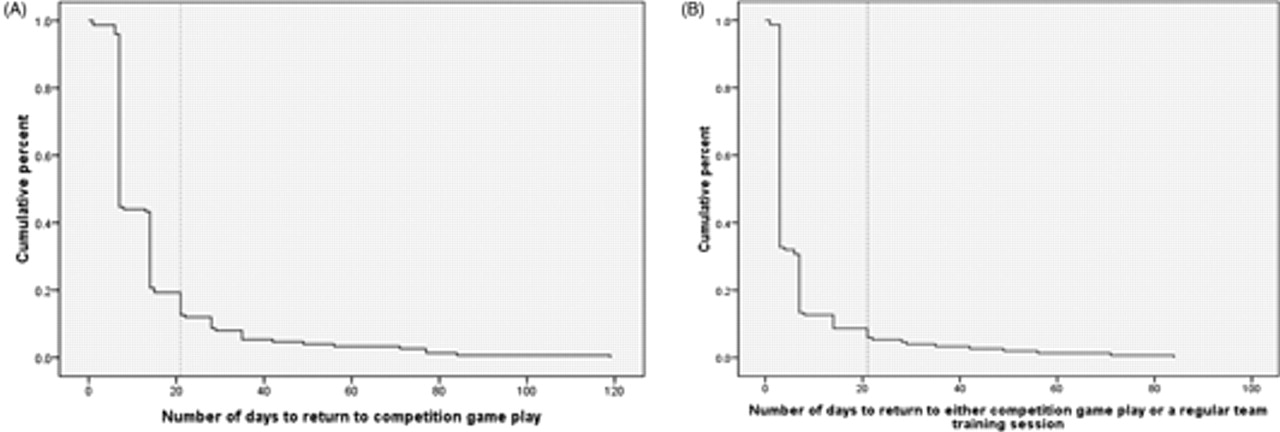
{kind=link}
(A) Time taken for players (n=150) to return to competition game play after their first concussion sustained throughout the study. (B) Time taken for players (n=150) to return to either competition game play or a regular team training session after their first concussion sustained throughout the study. End of regulation 3-week stand-down period is marked by a dotted line.
The median number of days until players returned to competition game play following their first concussion was longer at 7 days (range 1–119), indicating that many players returned to training before they returned to competition games. Of players who sustained a concussion, 56% returned to competition game play within 1 week, 81% by the second week and 88% by the third week. The Kaplan–Meier survival curve (see figure 1B) illustrates the time taken for players after the first concussion to return to competition game play. The median time to return to competition game play after the second concussion was 7 days (range 0–161), with 94% of players returning to play within 3 weeks. A slightly higher proportion of players returned to competition game play prior to completion of the 3-week stand-down period for their second concussion (94%) compared with their first concussion (88%). After their first concussion, the proportion of players returning to play within the 3-week stand-down period was slightly lower for those returning to competition game play only (88%) compared with those who returned to either competition game play or a regular team training session (95%). Of the three players who sustained a third or fourth subsequent concussion, the proportion returning to play within the 3-week stand-down period was the same regardless of whether they were returning to either competition game play or team training, or just competition game play only.
There was no significant association (p<0.05) between the concussed players' compliance with the 3-week stand-down regulation and the characteristics likely to be associated with the player's knowledge or behaviour regarding the regulation, namely, age, competition level, impulsive behaviour, years of rugby playing experience, player position, amount of training hours, wearing of headgear, history of recent (previous 12 months) concussion, timing of the most recent concussion and the number of recent concussions (see table 1). A significant association (χ12 p = 0.008) was observed between the number of concussions sustained by players throughout the study and player compliance with the 3-week stand-down regulation.
Player characteristics and compliance with the return-to-play regulation postconcussion
Only 22% (n=23) of players reported being given return-to-play advice postconcussion and of these players, none complied with the return-to-play regulation for returning to either competition game play or a regular team training session (100% player non-compliance) (table 2). Only 2 of the 23 players who received advice complied with the return-to-play regulation if ‘return-to-play’ was defined as returning to competition game play only (91% player non-compliance). Players aged 21–26 years were more likely to receive return-to-play advice postconcussion compared with the 15–20 years or 27+ year age groups. Players who trained for approximately 3+ hours per week were more likely to receive return-to-play advice compared with those who trained <3 h per week. According to the players who received advice (n=23), over three quarters received advice that did not comply with the regulation 3-week stand-down period, and of the remaining 22% (n=5) who received advice compliant with the regulation, all went against what was advised and were non-compliant in returning to play prematurely. The majority of players who received return-to-play advice (n=19) obtained it from medically trained personnel, with the remaining four players receiving advice from their coach (or a family member). Two players reported seeking further treatment after the game from a surgeon or an unspecified specialist.
Return-to-play advice and player behaviour in comparison with return-to-play regulation
Player behaviour on the field after sustaining a concussion, as reported by the coach, sports doctor or physiotherapist, showed that 48% of the players returned to play in the same game that the injury was sustained and 34% of the players did not leave the field at all (table 2).
Discussion
The current study is one of few to investigate the compliance of players with regulations for return-to-play postconcussion in sport. The main finding that 100% of players who received correct return-to-play advice failed to comply with the 3-week stand-down regulation for returning to either competition game play or a regular team training session is of concern. Among high school rugby union players,10,–,12 non-compliance with concussion return-to-play guidelines after being given correct advice has been reportedly much lower (40–50% of players). In contrast, in the current study, the schoolboy competition had the highest rate of player non-compliance (100%) compared with grade (97%) and suburban (91%) adult levels suggesting that there are differences in how return-to-play regulations are implemented across the different delivery settings.
The definition used in this study for players returning to play was taken from the IRB medical regulation stating that all players who suffer concussion should take a 3-week break from both training and games postconcussion. Having the definition inclusive of both training and games for defining return-to-play implicitly implies that all team training sessions include a contact component like that found in returning to competition game play. Issues may arise in attempting to quantify player non-compliance using this definition. With best practice for return-to-play postconcussion involving graded return to non-contact training, players may be classified as non-compliant when in fact they may be following neurological specialist return-to-play instructions. However, only two concussed players in the current study reported seeking further assistance from a specialist, albeit possibly not a neurological specialist as required by the code medical regulations.
When a player sustains a concussion during a rugby game, a decision is made at the time as to whether the player must leave the field or remain and continue playing. Coaches and support staff assess injured players and make return-to-play decisions from the sideline or on the field after stoppage of play. Almost half of the players in the current study who sustained a concussion returned to play during the same game with over one third of players not leaving the field, twice the proportion found in professional rugby union players (17%) in UK.23
In a Canadian study, 33% of ice hockey players who were advised by the team physician never to return to play postconcussion were non-compliant.8 Although this is a considerably lower proportion of non-compliance compared with the current study, it reflects intentional non-compliance as all players received return-to-play advice. In contrast, only 22% of players in the current study received return-to-play advice, yet like the Canadian study, these players were non-compliant. Although non-compliance with advice is a significant concern, it is important to be aware that the responsibility for sports safety is shared across different parts of the sports delivery system, with the players being only one component of this.7
Given the largely volunteer nature of community rugby union in Australia, the majority of players have limited medical support on the sideline and therefore, the type of advice provided by coaches and support staff varies considerably across the rugby union clubs. It is likely that people called upon to give return-to-play advice are not fully aware of the scientific evidence behind such advice, as has been shown to be the case in relation to coaches and lower limb injury prevention strategies.24 The regulation 3-week stand-down period postconcussion makes it easy for consistent implementation by sporting bodies; however, as highlighted in this study, it is not being fully implemented in community rugby. Greater efforts need to be devoted to developing advice and implementing that advice to teams, players and families involved.
A limitation of this study and other sports injury studies surrounds defining and identifying injury, in this case concussion. In attempting to capture concussion (which often goes unnoticed), our concussion definition was very inclusive and therefore may have possibly included players who had not, in fact, sustained a true concussion. Despite this, we validated the reporting of concussion using random DVD recordings for 10% of the 2007 study games (n=35). The assigning of a concussion from these recordings was compared against the assignment of concussion as allocated by the team injury reporters for the same game. Importantly, 70% of concussions reported were confirmed by DVD observation. In accounting for the remaining 30% of concussions, players may have sustained a concussion throughout the game (without stoppage of play) and received medical attention after the game where the concussion would have been unable to be validated by DVD observation. It is also possible that some injury reporters may have recorded a concussion as occurring when it was another type of head or facial injury, which could have contributed to the number of players not leaving the field. In relation to the latter, this bias, although small, is likely to have overestimated the poor adherence to the regulations.
It was not possible to obtain the return-to-play time for 20 players who sustained a concussion during the last game of the season. Although this was a small proportion of the overall injured group (11%), the absence of follow-up of these players poses a bias to the findings albeit unlikely to have changed the overall study findings. Of the injured players, 60% consented to follow-up 72 h postconcussion and importantly, these players did not differ significantly to those who did not consent, or were non-contactable, across all characteristics.
What is already known on this topic
Most sporting codes, like the rugby union, have medical regulations that are recommended for the safety of players. However, little is known about the transfer of this information through to the player via coaches and medical personnel, particularly regarding player compliance with concussion regulations or return-to-play advice, if provided.
What this study adds
This study has identified the gap between regulation and practice in community rugby, where the translation and implementation of concussion return-to-play regulations has clearly failed. The potential to reduce re-injury through improved provision of return-to-play advice, and subsequent regulation compliance, highlights the importance for further research into the underlying causes of non-compliance.
Finally, the study relied on player self-report in relation to the return-to-play advice they received postconcussion. The accuracy of these data is unknown as we did not collect information from the team staff on what advice was actually provided to each specific player. Bias from self-report is well known, including the time period between injury event and its recall. With the first training session usually within 3–4 days postconcussion, players at the 72 h follow-up would currently be (or have been) considering any return-to-play advice they received at the game for deciding whether to attend the training session.
Conclusion
Return-to-play decisions and the management of sport-related concussion is an important challenge faced by sports physicians, coaches and other support staff in community rugby union. Within this population, there is a gap between regulation and practice, with most players not receiving return-to-play advice following concussion, and all players who did receive the correct advice being non-compliant with the return-to-play regulation of the sports body. There is clearly a failure in the translation and implementation of concussion return-to-play regulations within community rugby. It is imperative that players and all those involved in the delivery of safe sport are made aware of the current medical and safety regulations.
Acknowledgments
The authors thank the New South Wales Sporting Injuries Committee (NSW SIC) for their continued support of new researchers in sports medicine research in Australia and the Australian Centre for Research into Injury in Sport and its Prevention (ACRISP) as one of the International Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee (IOC).
References
Footnotes
-
Funding The main funding for the study was provided by the NIH Centres for Disease Prevention and Control, The University of Pittsburgh, Pennsylvania, USA. The primary author received a National Health and Medical Research Council (NHMRC) postgraduate research scholarship during 2 years of PhD candidature, a scholarship from the New South Wales Sporting Injuries Committee and additional financial support from The George Institute for Global Health and the School of Public Health, The University of Sydney, Australia.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the University of Sydney Human Research Ethics Committee (HREC) and the US Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.