Article Text

Abstract
Objective To study the relationship between potentially game-disrupting incidents (PGDIs; red and yellow cards, goals and injuries) and the injury incidence in football.
Design Prospective injury surveillance during three FIFA World Cups in 2002, 2006 and 2010. Official match statistics were obtained for all the matches played in the three tournaments.
Setting 2002, 2006 and 2010 FIFA World Cups.
Participants Team physicians at the 2002, 2006 and 2010 FIFA World Cups.
Main outcome measures Injury incidences and incidence rate ratios (IRRs).
Results The injury incidence was significantly higher during match periods within the minute of, or during a five-minute period following a yellow card, red card, another injury or a goal (PGDIs) than during other match periods (76.7/1000 match hours; 95% CI (66.6 to 87.9) vs 54.0/1000 match hours (46.9 to 61.9), p<0.001). There were significant differences in injury incidence between different match periods, with the highest injury incidence seen in the last 15 min of the first half (p<0.001). The PGDIs (other than injury) had a tendency to increase towards the end of the game and the most frequent PGDI was a yellow card. There was a risk ratio of 1.17 (95% CI 1.08 to 1.26) for injury, per PGDI (other injuries excluded) (p<0.001), and 1.15 (95% CI 1.06 to 1.24) after adjusted match time (p<0.001).
Conclusions The injury incidence is high within the five minutes following a PGDI. For both team management and players, being aware of the increased risk of injury directly after a PGDI may be of clinical relevance, as it may enable them to take precautions in order to prevent injuries. There are significant differences in injury incidence between different match periods and game-related factors, such as PGDIs, appear partly to contribute to this variation.
- Soccer
- Sporting injuries
- Epidemiology
Statistics from Altmetric.com
Introduction
Owing to the huge popularity of the game of football, which unfortunately is not free of injury, research into the epidemiology of football injuries, their treatment and the potential for prevention is important. FIFA Medical Assessment and Research Centre (F-MARC) has therefore developed an injury surveillance system that has been successfully implemented at all FIFA tournaments since 1998.1 ,2
One important part of this epidemiological research has been directed at identifying risk factors for injuries in football. The risk factors are often divided into two subgroups, that is, intrinsic and extrinsic factors, related to the individual characteristics of a player and to environmental variables, respectively.3 The most important extrinsic factor in professional and international football appears to be foul play, which is involved in 12–61% of all injuries.2–10 Other extrinsic factors that have been studied include player exposure, match period, type of competition, match venue, current score and final result, among others.2 ,4 ,7 ,10–15 Psychological factors may also play a role and have probably long been underestimated.16
A study of the psychological and sport-specific characteristics of football players found that 90% of footballers are ready to commit a professional foul if required, depending on the score and importance of the match.17 Athletes concentration has been shown to be negatively affected by aroused, angry behaviour and by a social environmental setting of considerable complexity and stress.18 Moreover, watching pictures of players being hurt or severely injured has been shown to evoke emotional and physiological responses in players from the same sport.19 This suggests that game events could change the players’ mentality within a game, possibly increasing the risk of injury. In the past, the changes in injury occurrence within a match have mainly focused on differences in individual time periods of the match or comparing the injury frequencies between the two halves.1 ,6–8 ,11 ,12 ,20 Studies of player performance and the physiology of football players, however, show that there are periods and situations of high-intensity activity, followed by periods with a lower intensity, within a football match.21 ,22 It has been estimated that high-intensity activities in football account for 10–20% of match time.23
To the best of our knowledge, no previous studies have taken account of the possible effect of game events that form an essential and inevitable part of the game (goals, injuries, as well as red and yellow cards) on the injuries in football. The hypothesis in the present study was that these specific game events that affect the course of the game could be seen as potentially game-disrupting incidents (PGDIs), subsequently affecting the players’ attitudes, concentration and team strategies within a game and, accordingly, the occurrence of injuries.
The aim of the present study was to investigate the possible relationship between PGDIs and injuries in international top-level male football.
Materials and methods
The study material consisted of all injury reports with information about match play injuries in the men's FIFA World Cup in 2002 (Korea–Japan), 2006 (Germany) and 2010 (South Africa), as well as match statistics for all the games in these tournaments provided by FIFA's official internet website.24 The material included information on 441 match-play injuries reported on FIFA injury report forms,7 ,9 ,20 as well as match statistics relating to all 192 games played during these three tournaments. Table 1 shows the baseline data.
Characteristics of FIFA World Cups 2002–2010
The match statistics were assessed, using FIFA's official website,24 and they included the time and total number of goals and the time and total number of red and yellow cards. Combining the data from match statistics and injury report forms enabled additional factors to be included in order to analyse all injury circumstances. The injury report forms and the data collection methods are described in previous publications1 ,7 ,9 ,20 and followed the consensus statement on injury definitions and data collection procedures in studies of football injuries.25 The injury reports contain details of the type and location of the injury, the time when the injury occurred, the circumstances (non-contact, contact, foul play) and consequences (referees’ sanction, treatment) of injury, as well as an estimate of the absence from training and/or playing football, resulting from the injury. An injury was defined as any physical symptom that occurred during the match that received medical attention from the team physician, regardless of the consequences with respect to absence from the match or subsequent training.1 ,7 ,9 ,20 ,25
PGDIs were defined as yellow or red cards, injuries and goals. The factors included in the definition of PGDIs were chosen according to two main criteria: (1) the total numbers and minutes when they occurred had to be documented and (2) they had to have a potential impact on the following course of the match that could potentially affect several players simultaneously.
Injury incidence following a PGDI
The timing (minutes) of yellow cards, red cards and goals, as well as injuries from all games, was obtained from the official match statistics and the injury reports, respectively. The match was divided into two periods: (1) minutes played during the minutes of PGDIs or within the following 5 min and (2) other match periods. If there were two or more PGDIs within the same 5 min game period, only the minutes before the subsequent PGDI were calculated for the prior PGDI. The 5 min period was chosen, based on the finding that a football match is characterised by 5 min periods of high-intensity running, followed by 5 min periods with lower intensity running, compared with the average level during matches.22 According to the minutes of injury, obtained from the injury reports, the injuries were grouped into the corresponding match periods (1–5 min following PGDIs vs other match periods). The incidence of injury was then calculated for both match periods. Minutes of additional time were not taken into account.
Time of PGDIs in relation to the time of injuries during different match periods
The match was divided into six 15 min periods and extra time (when played). The PGDIs (injuries excluded) were grouped according to the minute they occurred, based on the match periods. The same was performed separately for all injuries based on the team physicians’ reports. The injury incidence and the mean numbers of other PGDIs were calculated for the different game periods separately. The relationship between PGDIs and injury incidence was assessed.
Statistical analysis
The incidence of injury was calculated using the formula: (number of injuries × 1000 match hours)/((minutes of exposure/60) × N players exposed) and expressed as the number of injuries per 1000 match hours.25
Injury incidence rates (per 1000 match-hours) with 95% CI were calculated assuming a Poisson distribution. Incidence rate ratios (IRR) and the test for a significant trend in injury incidence rates across the different groups were calculated using Poisson regression models. The 95% CIs for numbers of PGDIs per match period were obtained by bias-corrected bootstrapping (5000 replications). The level of significance was set at p values of <0.05. The STATA 12.1, StataCorp LP (College Station, Texas, USA) statistical package was used for the analyses.
Results
Injury incidence following a PGDI compared with the rest of the match
The total injury incidence was 67.8/1000 match-hours (95% CI 61.7 to 74.5). For 412 injuries (93.4%) the time (minute) of injury was reported on the injury report forms and only these were included in the study.
On average, there were 9.5 PGDIs (SD 3.8) per match. The most frequent PGDI was a yellow card, with an average of 4.6 yellow cards a match (SD 2.6), followed by goals (2.5; SD 1.6), injuries (2.3; SD 1.7) and red cards (0.3 SD 0.6). The total match exposure was 2686 player hours for match periods from the minutes of PGDIs to the following 5 min, and 3815 player hours for other match periods. Two hundred and six injuries (50%) occurred during match periods at the minutes of PGDIs or within the following 5 min, giving an injury incidence of 76.7/1000 match-hours (95% CI 66.6 to 87.9), which was significantly higher compared with other match periods (54.0/1000 match-hours; 95% CI 46.9 to 61.9) (IRR 1.42; (1.17 to 1.72), p<0.001).
Time of PGDIs in relation to the time of injuries during different match periods
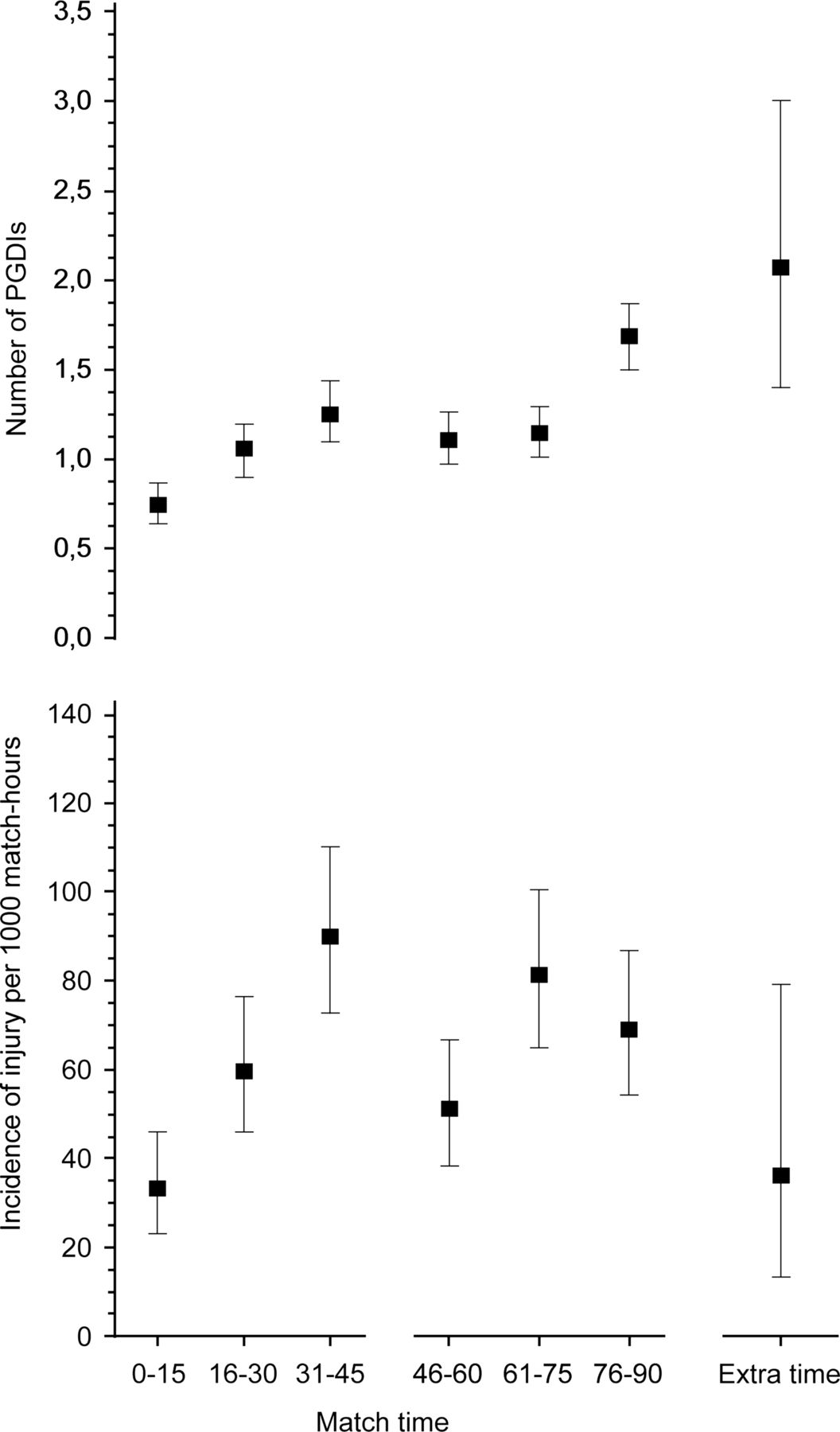
The lower part of figure 1 shows the variation in injury incidence across different match periods. The differences in the injury incidence between the match periods were statistically significant (p<0.001), with the highest injury incidence calculated for the last 15 min of the first half (90/1000 match-hours; 95% CI 72.8 to 110) and the lowest for the initial 15 min period of the match (33.1/1000 match-hours; 95% CI 23.1 to 46.1). The upper part of figure 1 shows the means of PGDIs (injuries not included) during the different match periods. There was a risk ratio of 1.17 (95% CI 1.08 to 1.26) for an injury per PGDI (other than injury) (p<0.001) and 1.15 (95% CI 1.06 to 1.24) after adjusted match time (p<0.001).
{kind=link}
Average incidence of injury and number of other potentially game-disruptive incidents during the course of the match.
Discussion
The most important finding in the present study was that the injury incidence is high during a 5 min period following a PDGI (ie, goal, injury to another player, as well as red or yellow cards).
The hypothesis in the present study was that red and yellow cards, injuries and goals could disrupt the normal course of the game, evoke responses from both players and teams, at both a strategic and a psychological level, leading to an increased injury risk. With the exception of foul play, essential and inevitable game events within a game have not been studied as possible extrinsic risk factors for injuries. Contact between players accounts for between 63% and 86% of the injuries in international football tournaments.1 ,7 ,9 ,10 ,20 Foul play and the possible subsequent yellow and/or red cards may provoke aggression and, in the worst cases, even action involving elements of revenge among the players of the team against which the foul was committed. Moreover, injuries resulting from contact, even when they do not involve foul play, may provoke aggression among the injured player's team-mates. Players’ concentration on the game and awareness may be affected by PGDIs and fouls in a disadvantageous way, leading to an increased risk of injury. The results of a study assessing the effect of behavioural and situational factors on concentration and skill performance in sports suggest that concentration is negatively affected by aroused, angry behaviour and by a social environmental setting of considerable complexity and stress.19 Psychological stressors and situation-dependent emotional states seem to have an effect on athletes’ risk of injury.16 Stanger et al18 found greater physiological responses (blink responses, heart-rate deceleration, P300 and slow-wave potentials) when athletes were looking at unpleasant sport-specific pictures (players being hurt by another player or players being badly injured) compared with neutral or pleasant pictures. The participants in the study by Stanger et al were both male and female football, rugby and field hockey players. These findings present possible underlying factors for altered emotional states and subsequent physiological responses resulting from some of the PGDIs, perhaps affecting the injury risk. However, we found no studies showing a relationship between these physiological responses and sports injuries in the literature.
Changes in the score (goals) can also affect player attitudes, awareness and team strategies. Junge et al17 found that 90% of football players were ready to commit an intentional (‘professional’) foul if required, depending on the score and importance of the match. The FIFA World Cup is one of the most followed and valued sports tournaments and the relatively small number of matches per team during the tournament highlights the importance of each match. Significant variation in the injury incidence depending on the current score has been shown in FIFA World Cup matches.13
It has been shown that the total incidence of injury (without taking into account injury or player specific factors) increases towards the ends of each half and this has generally been attributed to increasing fatigue of the players, which does indeed appear to play an essential role.4 ,11 ,26 However, previous research also shows that the amounts of high-intensity running and distance covered by sprinting are similar in the last 15 min of the first half and the first 15 min of the second half22 and this is somewhat contradictory in relation to the fatigue hypothesis. The present study found the highest injury incidence in the matches during the last 15 min of the first half, and a tendency for the incidence to decrease during the last 15 min of the game (figure 1), when fatigue supposedly accumulates.22 A comparison of the variation in injury incidence and the mean numbers of PGDIs (injuries not included) in figure 1 reveals a similarity in the increased injury incidence of injury, towards the end of each half and the increasing numbers of other PGDIs, with the exception of the last 15 min of the match and extra time. It could be claimed that the accumulating fatigue towards the end of the game, resulting in lower levels of high-intensity running and sprinting,22 with a subsequent reduction in potential trauma energy, might reduce the incidence of injury.
Video analysis could possibly have reduced the bias of possible incorrectly reported injury minutes. However, previous research demonstrates that it incorporates other sources of bias. First and foremost, not all injuries are identified on video recordings.27–30 Second, a larger percentage of contact injuries compared to non-contact injuries are identified on video material.28–30 Fuller et al31 avoided this bias by analysing the injuries resulting from tackles only. Tscholl et al27 analysed the injuries in six women’s top-level tournaments from video recordings, and discussed wrong selections of video recordings as a possible reason for a lack of concordance between injury report data and the data obtained by video analysis.
Study limitations
One possible limitation could be inaccurate minutes of injuries in the injury reports. As the team doctors filled in the injury reports after the matches, it is possible that some reported injury times are merely approximations rather than exact minutes. The half-time break was not taken into account. A half-time break may, however, have a transitory calming effect on the game and, if a PGDI had occurred in the last minutes of the first half, the following half-time break might reduce the intensity following one of these incidents. It has been shown for both halves of the match that fewer injuries tend to occur during the first parts of the half compared with the last minutes,6 ,7 ,9 ,26 ,32 and the findings in the present study are in line with this. The exclusion of minutes of additional time from the analysis may also have been a source of bias. Further limitations were the exclusion of other interruptions (goal kicks, substitutions, free kicks and so on) from the analysis; they too, may have a calming effect on the game, as they may allow the players to take a short break. Differences between injury types, locations or the severity of injuries were not taken into account and individual player exposures were not recorded. Differences between the effects of the different factors included in the definition of PGDI on injury incidence were not taken into account.
The definition of PGDIs applied in the present study may be regarded as strength and a limitation. The match events defined as PDGIs were chosen because of their potentially major effect on players’ attitudes and concentration, teams’ strategies and, accordingly, the subsequent course of the match. There might be numerous other factors, such as aggressive or insulting comments by players or fans, personal frustrations, referees’ mistakes and rejected goals, among perhaps countless others, that affect the players’ concentration that have similar effects. However, data on all of these may be impossible to obtain, and therefore their significance difficult to assess. Whether or not all reported injuries should have been included in the definition of PGDIs is controversial. It might be argued that only acute injuries that result in a clear interruption of the game should be included, as some other injuries (or their symptoms) may occur by gradual onset (ie, some overuse injuries) and not reach the consciousness of many players simultaneously and have a more moderate impact on the match. However, there is to our knowledge no reliable tool available for assessing which particular injuries the players, team management and referees become aware of at the specific moment of injury, and furthermore, whether some injuries affect the subsequent course of the match more than others. Therefore, all reported injuries were included in the present study.
Clinical implications
Recognising the significance of the proximity of PGDIs and injuries, opportunities for sanctions, including temporary expulsion from a game for players committing violent fouls, could be considered. A few minutes’ absence for the player violating the rules could theoretically help to re-establish the players’ concentration on the game more rapidly. For both team management and players, being aware of the increased risk of injury directly after a PGDI may be of clinical relevance. It may be useful for coaches to take this into account when discussing team tactics in order to prevent injuries.
What are the new findings?
-
The incidence of injury within a 5 min period following potentially game-disruptive incidents (PGDIs) was significantly higher than during other match periods.
-
There were on average 9.5 PGDIs per match, and the most frequent PGDI was a yellow card.
-
The frequency of PGDIs increased towards the end of each half.
How might it impact on clinical practice in the near future?
-
The findings may help to improve the planning of medical services and injury prevention during major football tournaments.
-
The teams may be able to reduce the risk of injuries through interaction between players, team medical staff and team management.
-
The findings may be of use to referees in order to protect the players by sanctioning foul play, especially during game periods with a high risk of injury.
Acknowledgments
The authors gratefully acknowledge FIFA (Fédération Internationale de Football Association) for funding this study. We also greatly appreciate the cooperation of all the team physicians who provided the injury data. We express our gratitude to Professor Ilkka Kiviranta (University of Helsinki) whose initiative was essential for this project to be realised.
References
Footnotes
-
Contributors JR coordinated the study, collected part of the data, conducted the statistical analysis, together with HK and wrote the major part of the final manuscript. All authors participated in the study design through revision and by partly writing the research plan, as well as all versions of the manuscript. AJ, JD and LP played a key role in the collection of injury data. AJ prepared the anonymous injury data files. JK supervised and took part in all the phases of the study since its conception, as well as revision and writing of all versions of the manuscript. MB participated in revision and writing of the research plan, the first draft as well as the final manuscript.
-
Funding FIFA (Fédération Internationale de Football Association).
-
Competing interests None.
-
Ethics approval The ethics approval for injury surveillance has been obtained before by F-MARC. This approval covers the data of the present study and articles based on these data have been published before (i.e. Br J Sports Med 2007;41:578-581 doi:10.1136/bjsm.2006.034579).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com