Article Text

Abstract
Background Previous reviews have highlighted the benefit of loaded therapeutic exercise in the treatment of tendinopathy. Changes in observable structural outcomes have been suggested as a possible explanation for this response to therapeutic exercise. However, the mechanism for the efficacy of therapeutic exercise remains unclear.
Objective To systematically review the relationship between the observable structural change and clinical outcomes following therapeutic exercise.
Data sources An electronic search of AMED, CiNAHL, Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, PEDro and SPORTDiscus was undertaken from their inception to June 2012.
Study eligibility criteria Any study design that incorporated observable structural outcomes and clinical outcomes when assessing the effect of therapeutic exercise on participants with tendinopathy.
Study appraisal and synthesis methods Included studies were appraised for risk of bias using the tool developed by the Cochrane Back Review Group. Due to heterogeneity of studies, a qualitative synthesis was undertaken.
Results Twenty articles describing 625 patients were included. Overall, there is a strong evidence to refute any observable structural change as an explanation for the response to therapeutic exercise when treated by eccentric exercise training. Moderate evidence does exist to support the response of heavy-slow resistance training (HSR).
Conclusions and implications of key findings The available literature does not support observable structural change as an explanation for the response of therapeutic exercise except for some support from HSR. Future research should focus on indentifying other explanations including neural, biochemical and myogenic changes.
Registration Number Registered with PROSPERO, registration number CRD42011001638.
- Tendons
- Exercise rehabilitation
- Ultrasound
- Eccentric exercise
Statistics from Altmetric.com
Introduction
Tendinopathy is a widely accepted, generic term that encompasses any abnormal condition of a tendon.1 Clinical symptoms include activity-related pain associated with tenderness, localised swelling and disability.2 Tendinopathy is reported to be the cause of 30–50% of all sports-related injuries.3 Furthermore, within top level runners, there is a 52% lifetime risk of developing Achilles tendinopathy.4 Patellar tendinopathy is reported to be responsible for 20% of all knee injuries attending a sports medicine clinic.5 Tendinopathy is also prevalent within the lateral and medial epicondyle of the elbow and the rotator cuff of the shoulder.6
Previous reviews have highlighted the benefit of loaded therapeutic exercise in the treatment of tendinopathy.7–10 Such approaches include a variety of exercise regimes (table 1). Tendinopathy is a characteristic of structural changes that alter the loading capacity of a specific tendon.11 Changes to structural outcomes such as neovascularisation and tendon diameter have been reported as a response to therapeutic exercise.12 ,13 Generally it is thought that the loading forces applied to the affected tendon help stimulate the remodelling of the abnormal tendon structure by alterations to blood and fluid flow.14 ,15
Overview of the therapeutic tendon loading exercise regimes used
Despite widespread theorises being proposed to explain the response to therapeutic exercise, the histological adaptations and the explanations of improved clinical outcomes have yet to be established.16 Hence, the mechanism for the efficacy of the therapeutic exercise remains unclear.17 No previous reviews have been indentified that investigate observable structural change as an explanation for improved clinical outcomes following therapeutic exercise. Therefore, the purpose of this paper was to determine whether there was a correlation between the structural change and clinical outcome, based on the current evidence base.
Methods
Protocol and registration
A systematic review was performed using a predetermined protocol in accordance with the PRISMA statement.18 The study protocol was registered with PROSPERO, registration number CRD42011001638.
Data sources and search strategy
An electronic search of AMED, CiNAHL, Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, PEDro and SPORTDiscus was undertaken from their inception to June 2012. The search terms used for the MEDLINE search are displayed in table 2. This strategy was adapted for the other database searches.
Search terms used in the study selection process
The electronic search was complemented by hand searching the reference lists of pertinent papers identified and previous systematic reviews on related topics. In addition, a recognised expert in this field was consulted in an attempt to identify any further published or unpublished studies. The search was conducted by two reviewers (CL and BS).
Inclusion criteria
Population
Human adult participants diagnosed with tendon-related disorders including but not restricted to tendinosis, tendinopathy, tendinitis, partial or full thickness tears. Animal-based studies were excluded.
Intervention
Exercises were considered relevant if they were specified as designed to place therapeutic load on the tendon. Exercise regimes might be described as eccentric, concentric, isometric, isotonic and isokinetic. Non-exercise interventions, for example, electrotherapy, manual therapy and injections were excluded.
Outcome
Structural changes of the tendon observable via imaging techniques including diagnostic ultrasound, MRI or CT. Any clinical outcomes including, but not restricted to, measures of pain and disability were included.
Study design
Any study design that incorporated measurement of observable structural changes and clinical measures of pain and/or disability including case study, case series, cohort study, uncontrolled clinical trials, quasi-experimental studies and randomised controlled trials (RCTs). Preclinical or biological studies and narrative reviews, editorials or opinion-based publications were excluded.
Language
English languages papers were included. Studies were excluded if they are only published in languages other than English.
Critical appraisal
The risk of bias of the included studies was undertaken independently by two reviewers (BD and BS) using the Cochrane Back Review Group (CBRG) risk-of-bias tool.19 The CRBG tool was used because currently there is no ‘gold standard’ for any study design, nor is there any widely accepted generic tool for critical appraisal that can be applied equally across all study types.20 It was theorised that the most appropriate design to answer our question was the RCT. The RCT design minimises potential sources of bias relating to selection of participants and assessment of outcome. Hence, all studies should be assessed against this standard. The CBRG tool has an empirical evidence to support it use,21 and is now widely used in systematic reviews. Each item was rated as yes (1), no (0), unclear (?) or not applicable (N/A). If the information was unclear, attempts were made to contact the specific authors to clarify these queries. A study with a low risk of bias was defined as one fulfilling six or more criteria.
Data extraction
Two independent reviewers (BD/BS) used a standardised form to extract data regarding study characteristics, participant characteristics, interventions, settings and outcome data/results.18 The data extraction process was initially piloted by the two reviewers before the study was undertaken. Only data from the therapeutic exercise intervention were analysed.
Results were analysed to determine the association of pain, function and treatment satisfaction on tendon diameter, neovascularisation, structural abnormalities, tendon volume and tendon cross-sectional area.
For the purpose of this study, the clinical outcome Victorian Institute of Sport Assessment-Achilles questionnaire (VISA-A) and Victorian Institute of Sport Assessment-Patella questionnaire (VISA-P) were included under ‘pain’ due to the questionnaires being constructed to cover the three domains of pain.22 The term ‘structural abnormalities’ was used to encompass: echoic aspects, longitudinal splitting and intratendinous calcification as used commonly in the current literature.23 ,24 Upon completion, the reviewers met to agree upon the data to be extracted. A third reviewer (TS) was available in the event of disagreement.
Data synthesis
There was considerable clinical heterogeneity within the included studies with regard to the exercise interventions.25 Therefore a qualitative review was deemed the most appropriate means to analyse the data. The qualitative synthesis of data was informed and interpreted using the levels of evidence (table 3) determined by the results of the risk-of-bias assessment and the methodological quality of the included studies.21 A subgroup analysis was conducted using the three types of therapeutic exercise regime: eccentric exercise training (EcEx), heavy slow resistance training (HSR) and medical exercise therapy (MedRx).
Levels of evidence21
Results
Study selection
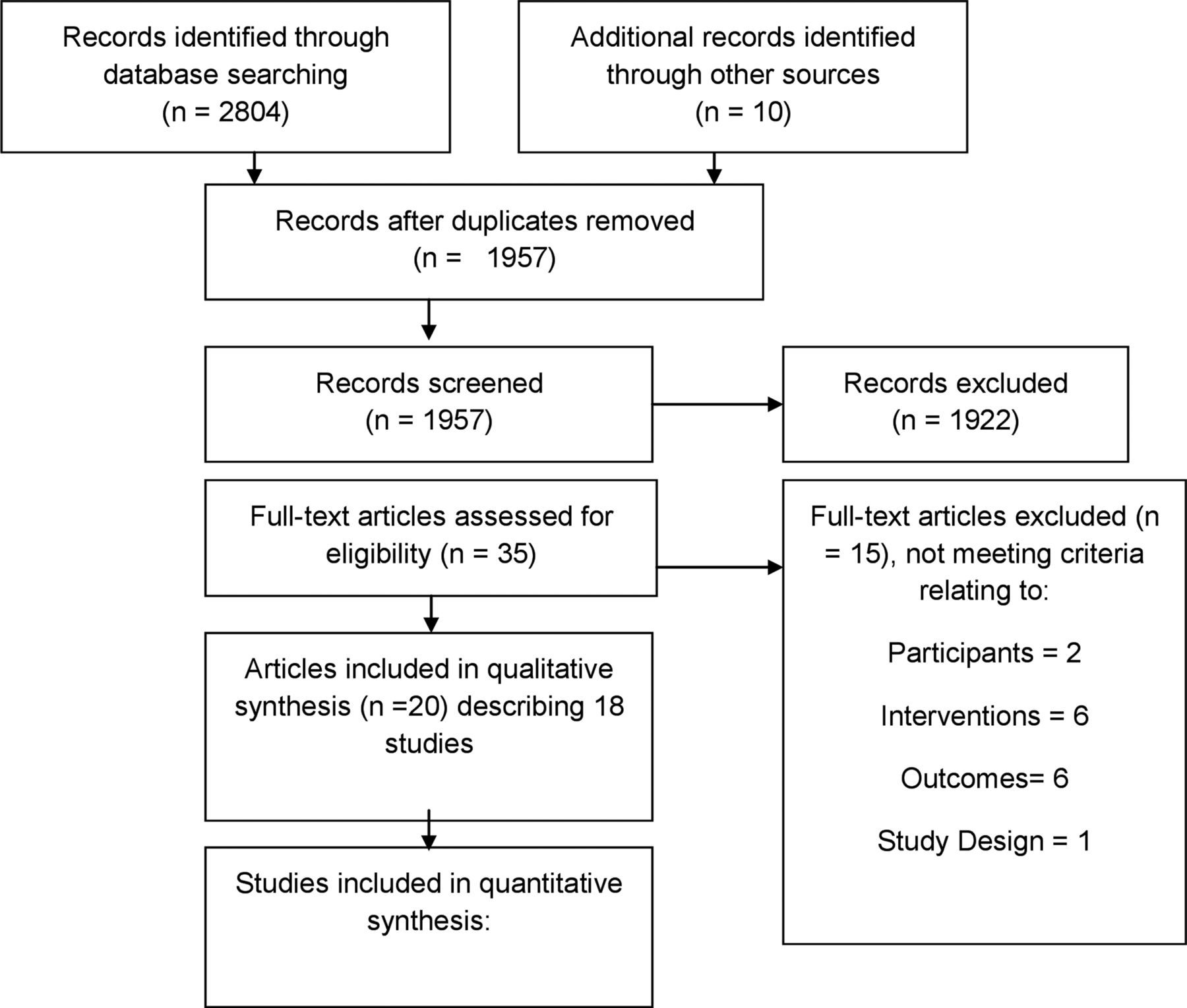
Figure 1 represents the results of the study identification process. Initially, 1957 citations were indentified once duplications were removed. After screening, 35 studies were considered for full review. Applying the eligibility criteria, 20 papers describing 18 studies were included in qualitative synthesis. There were two incidences where one study of the same cohort was published across two papers.26–29 However in both instances; the papers presented the results of different outcomes. Therefore both publications were reviewed to extract all pertinent data.

{kind=link}
Study selection flow diagram.18
Risk-of-bias assessment
The results of the risk-of-bias assessment are shown in table 4. Eight studies had a low risk of bias.23 ,24 ,26 ,27 ,30–34 The remaining 10 studies were determined to have high risk of bias. Blinding of the patient to the intervention and blinding carer to the intervention were recurrent weaknesses across the included studies with only one study satisfying both criteria.26 ,27
Risk of bias for the included studies
Study characteristics
A summary of the characteristics of the included studies are shown in online supplementary table S5.43
Study design
The most frequently used study design was the RCT (n=7)24 ,26 ,27 ,30–34 and the prospective cohort (n=7).15 ,28 ,29 ,35–39 The other designs used were controlled trial (n=2),23 ,41 case series (n=1)40 and case study (n=1).42
Participants
The studies included 625 participants, 342 men and 291 women. The mean age of the participants was 44.2 years, ranging from 32.432 to and 73 years.42 The mean duration of symptoms was 21.9 months, although one study40 had a comparatively longer mean duration of symptoms of 57.6 months for their cohort of six participants.
Clinical findings
Pain versus structural change
Overall, there is conflicting evidence relating to the association between pain and structural change following therapeutic exercise.
Pain against tendon diameter
EcEx
There is strong evidence from five RCTs with a low risk of bias24 ,30 ,32–34 and one low-quality study with a low risk of bias23 to suggest that a reduction in pain is not associated with a reduction in tendon diameter. Only one low-quality study with a high risk of bias41 supports the association.
HSR
There is moderate evidence from one RCT with a low risk of bias32 to suggest that a reduction in pain is associated with a reduction in tendon diameter.
Pain against neovascularisation
EcEx
There is strong evidence from four RCTs with a low risk of bias26 ,27 ,30–32 and one low-quality study with a high risk of bias38 to suggest that a reduction in pain is not associated with a reduction in neovascularisation. Only two low-quality studies with high risk of bias35 ,41 support the association.
HSR
There is moderate evidence from one RCT with a low risk of bias32 to suggest that a reduction in pain is associated with a reduction in neovascularisation.
Pain against structural abnormalities
Pain against tendon volume
EcEx
There is a limited evidence from one low-quality study with high risk of bias28 ,29 to suggest that a reduction in pain is associated with a reduction in tendon volume at short-term follow-up. There is a limited evidence to support that a reduction in pain is not associated with a reduction in tendon volume at long-term follow-up.29
Pain against cross-sectional area
HSR
There is limited evidence from one low-quality study with a high risk of bias37 to suggest a reduction in pain is not associated with an increase in cross-sectional area.
Function versus structural change
Overall, there is conflicting evidence relating to the association between function and structural change following therapeutic exercise.
Function against tendon diameter
EcEx
There is strong evidence from two RCTs with a low risk of bias32 ,33 and one low-quality study with a low risk of bias23 to suggest that an improvement in function is not associated with a reduction in tendon diameter.
HSR
There is moderate evidence from one RCT with a low risk of bias32 to suggest that an improvement in function is associated with a reduction in tendon diameter.
Function against neovascularisation
EcEx
There is strong evidence from two RCTs with a low risk of bias26 ,27 ,32 and one low-quality study with a high risk bias38 to suggest that improvement in function is not associated with a reduction in neovascularisation.
HSR
There is moderate evidence from one RCT with low risk of bias32 to suggest that an improvement in function is associated with a reduction in neovascularisation.
Function against structural abnormalities
Function against tendon volume
Pain against cross-sectional area
HSR
There is limited evidence from one low-quality study with a high risk of bias37 to suggest that an improvement in function is not associated with an increase in cross-sectional area.
Treatment satisfaction versus structural change
Overall, there is conflicting evidence to support the association between treatment satisfaction and structural change following therapeutic exercise.
Treatment satisfaction against tendon diameter
EcEx
There is strong evidence from two RCTs with a low risk of bias30 ,32 to suggest that an improvement in treatment satisfaction is not associated with a reduction in tendon diameter. One low-quality study with high risk of bias39 does support the association.
HSR
There is moderate evidence from one RCT with low risk of bias32 to support that an improvement in treatment satisfaction is associated with a reduction in tendon diameter.
Treatment satisfaction against neovascularisation
EcEx
There is strong evidence from three RCTs with a low risk of bias26 ,27 ,30 ,31 and one low-quality study with a high risk of bias35 to suggest that an improvement in treatment satisfaction is not associated with a reduction in neovascularisation. Only one low-quality study found an association.15
HSR
There is moderate evidence from one RCT with low risk of bias32 to suggest that an improvement in treatment satisfaction is associated with a reduction in neovascularisation.
Treatment satisfaction against structural abnormalities
Discussion
This systematic review suggests that when therapeutic exercise is considered as a whole, conflicting evidence exists in relation to structural change. However, analysed by specific regimes, strong evidence exists to refute observable structural change as an explanation for the response to EcEx. Treatment using HSR demonstrated moderate evidence to suggest an association with both tendon diameter and neovascularisation but not cross-sectional area. It must be noted, however, that the support for HSR is based on a single RCT so a degree of caution on this interpretation is advised. Conflicting evidence exists from low-quality studies in relation to the hypothesis that there is an association between structural change and clinical outcome following MedRx.
To the authors’ knowledge this is first systematic review of its kind. Previous systematic reviews have investigated the clinical outcome of therapeutic exercise, in particular EcEx, for the treatment of tendinopathy.7 ,9 None of these studies have specifically focused on the observable structural changes and their response to therapeutic exercise. The current review was undertaken in accordance with published guidelines.18 A minimum of two reviewers were involved at each stage of the review in order to minimise bias. In contrast to the previous reviews in the field, the current review included RCT and non-RCT studies which the authors acknowledge can lead to potential bias.44 It was considered that the inclusion of all study types represents the evidence base as whole; thus allowing the clinician to make their clinical reasoning based on a synthesis of all the available evidence.45 However, to aid this, the data synthesis was constructed to reflect the risk of bias and methodological quality by using a best-evidence synthesis.21 The nature of the research design of the included RCTs meant that often data were analysed from a single arm of the trial. The authors recognise that the optimal research design for the included studies would ideally include a randomised therapeutic exercise group versus a ‘sham’ therapeutic exercise group with a long-term clinical and structural follow-up. This may be an area for future study.
Despite a few exceptions, generally the studies with a low risk of bias demonstrated no association between structural and clinical outcome following therapeutic exercise. The studies with a high risk of bias demonstrate some association. One possibility for this discrepancy could be the presence of both outcome and selection bias. A current theme of the high risk of bias studies was the lack of outcome assessor blinding and random treatment allocation which is known to cause potentially inflated findings.46 Langberg et al47 showed using microdialysis that following eccentric exercise an increase in collagen synthesis occurs after 12 weeks. The authors, however, were only able to speculate to whether this would translate into changes in the structural outcomes used in the present review. The lack of translation into observable structural outcome may be the result of different follow-up durations and procedures. Almost half the included studies followed their participants for longer than 6 months.24 ,29–31 ,33 ,34 ,36 ,38 ,39 However only four studies30 ,33 ,34 ,38 incorporated a structural outcome assessment at follow-up. Furthermore, it must be noted that treatment satisfaction appears to be used by some of the included studies15 ,39 as a proxy for clinical outcomes such as pain and disability which is likely to affect the construct validity of the outcome measures used.
Worthy of discussion is the moderate evidence to support the prescription of HSR. The significant structural change seen in HSR compared with the more commonly prescribed EcEx regimes maybe the result of the HSR only being performed three times per week as opposed to daily. This may allow more time for structural changes such as collagen synthesis.32 Collagen synthesis may also be influenced by the loading magnitude.32 HSR by nature uses a high-loading magnitude which is calculated clearly based on repetition maximum while the EcEx regime also stipulates increased loading but the method of loading progression is less standardised and more reliant on patient compliance. Nevertheless, the RCT in which HSR supports structural change,32 despite having a low risk of bias and demonstrating high-methodological rigour, recruited only a small sample which solely consisted of men, limiting the generalisability of the findings.
The conclusions drawn from the current review are based on predominantly Achilles tendinopathy with the other studies examining the knee,32 ,37 elbow,23 ankle38 and shoulder.40 ,42 The efficacy of tendinopathy treatment will most likely be dependent on the specific tendon's anatomical and biomechanical characteristics.48 For example, with Achilles tendinopathy most commonly manifesting in the mid-portion and patellar tendinopathy occurring as an enthesopathy,49 this variation may potentially affect the outcome of HSR on treating Achilles tendinopathy.
The structural responses demonstrated in the included studies were established by grey-scale ultrasonography, Doppler ultrasonography, MRI and ultrasound tissue characterisation (UTC). Despite being important outcomes within the present review, both grey-scale ultrasonography and MRI have well-documented limitations regarding their reproducibility. Both have reported poor interobserver reliability due to grey-scale ultrasonography being a vastly operator-dependent technique50 and MRI being greatly influenced by the interpreters’ experience.51 UTC appears to have better inter-observer reliability and greater ability to differentiate asymptomatic and symptomatic tendon yet this tool is still arguably in its infancy with regards to human populations.50 As a general rule, the use of imaging within tendinopathy research challenges the external validity of the findings, since because routine imaging is not currently recommended practice36 so researchers need to be aware of the potential for bias with patients feeling more reassured and reporting more positive pain outcomes when regularly investigated.
Neovascularisation, identified by both colour and power Doppler ultrasonography, has previously been thought to adapt to therapeutic exercise regimes.15 One explanation for the refutation in the current review could be the lack of standardisation with examination. First, three studies used power Doppler, the other four used colour Doppler. Previous authors have suggested that power Doppler is more sensitive in quantifying the amount of neovascularisation compared with colour Doppler since power Doppler is capable of identifying all flow, independent of velocity.52 Likewise, the lack of a gold standard scoring system makes comparison between studies challenging. Many of the studies adopt a five-point-graded modified Ohberg score while some use less robust methods. The concern with using a questionnaire with items ‘poor’ to ‘excellent’ is the potential of acquiescent response bias;53 while scales with greater categories have been suggested to make significant correlations with structural outcomes possible.52 Debate also surrounds the significance of pre-examination activity levels on neovascularisation scoring because rest has been associated with a low-blood flow.54 To address this, some researchers have suggested that 24 h abstinence from physical activity before Doppler examination.35 None of the studies reviewed made any clear consideration of this variable.
Finally, an additional factor that may play role in accounting for the disparity between clinical outcome and structural change could be the stage of the pathological tendon. Cook and Purdam11 recently proposed a continuum of pathology for tendinopathy. Within the included studies of our review, diagnostic subgroups may have existed within the cohorts which may have the potential to make a very different type of tendon pathology.55
Future directions
The finding of the current review suggests that studies with low risk of bias show no association between structural outcome and clinical outcome following the more commonly prescribed EcEx. Despite the positive association when treated by HSR, the mechanism for therapeutic exercise remains unclear. Clinically, emphasis should be focused on the clinical outcome and physical examination, with less reliance on the results of structural outcomes. While not directly reviewed here, the findings also question the use of observable structural outcomes as a prognostic tool in tendinopathy. Perhaps other outcomes for example, patient-reported outcome measures should be considered instead. This is an avenue for future research.
While a clear explanation for the response of tendinopathy to therapeutic exercise is lacking then further studies to identify the underlying mechanism are warranted. Theories surrounding the potential influence of neural, biochemical and myogenic factors have been proposed37 ,56 ,57 and merit further review. While still considering the likelihood of a multifactorial explanation.58 The findings of the review also suggest that further research could consider HSR as an alternative to EcEx. As highlighted as a weakness in the current literature, future studies should be conducted using validated measurement tools to standardise findings. Consideration should be made to the tendinopathy continuum, and to the possibility that diagnostic sub-types exist. Selection criteria should be devised to address this developing principle.
Conclusions
There is a strong evidence to refute observable structural change as an explanation for response to EcEx. However, there is a moderate evidence to support the explanation when treated by HSR. The evidence as a whole would indicate that treatment progress should be guided by clinical examination and patient-reported outcome measures, rather than structural imaging. Future study based on adequately powered RCTs should aim to investigate other potential mechanisms for the effect of therapeutic tendon loading exercise such as neural, biochemical or myogenic factors. These studies should address underlying variables such as diagnostic tendon subgroups with consideration of tendinopathy as a pathological continuum.
What this study adds
-
Observable structural change of the tendon does not explain the response to eccentric exercise training.
-
Treatment progress should be guided by clinical examination and patient reported outcome measures rather than reliance on structural imaging.
-
Adequately powered randomized controlled trial should aim to investigate alternatives to structural change as an explanation for the response to therapeutic tendon loading exercise.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 5
Footnotes
-
Contributor BD contributed to at all stages of the research and is the overall guarantor. TS, CL and BS were all involved in the design of the study and interpretation of data; drafting and revising the study and approval of the final draft.
-
Competing interest None.
-
Provenance and peer review Not commissioned; externally peer reviewed.